Research Article
Glycemic Response and Satiety to Traditional and High Fiber Cereal Preparations of Kerala Cuisine in Healthy Volunteers
Nivedita*, Harish Kumar, Sundaram KR and Arun S Menon
Amrita Institute of Medical Sciences, Amrita University, Kochi, Kerala
Corresponding author: Nivedita, Clinical Nutritionist, Amrita Institute of Medical Sciences and Research Centre, AIMS Ponekkara P.O, Kochi, Kerala-682041, India, E-mail: brinivedita@aims.amrita.edu
Citation: Nivedita, Kumar H, Sundaram KR, Menon AS. Glycemic Response and Satiety to Traditional and High Fiber Cereal Preparations of Kerala 02 Cuisine in Healthy Volunteers. Indian J Nutri. 2017;4(1): 154.
Copyright © 2017 Nivedita, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 4, Issue: 1
Submission: 10/12/2016; Accepted: 21/02/2017; Published: 23/01/2017
Abstract
Objective: To determine the glycemic response and satiety of the selected traditional and high fiber preparations of Kerala cuisine in healthy volunteers.
Methodology: Ten healthy volunteers working at Amrita Institute of Medical Sciences (AIMS) who met the inclusion and exclusion criteria were chosen for the study. Blood glucose response was studied after a 12 h overnight fast. Ten traditional and ten high fiber cereal preparations were tested. Capillary blood glucose were tested at 30, 60, 90 and 120 mins after consuming the food item using finger prick test. Hunger/satiety scale was used to record hunger, fullness and desire to eat after each meal.
Results: Out of the 10 volunteers who participated in the study 6 were females. The mean age of these subjects were 25.2+1.5. Mean BMI of these healthy volunteers were 20.69+1.51. On comparison with the traditional and high fiber cereal preparations of Kerala cuisine there was a significant difference in the mean blood glucose values at 120 mins between food items dosa - chutney and wheat dosa - tomato chutney (p=0.001), dosa, chutney and ragi dosa - tomato chutney (p=0.041), puttu - banana and corn puttu - kadala curry (p=0.045), puttu - banana and corn puttu - cherupayar curry (p=0.037). The high fiber cereals of similar preparations were compared at 120 mins and it was shown that there is a significant difference in the mean blood glucose of ragi dosa and rava dosa (p=0.004), wheat dosa and ragi dosa p 0.001 and wheat dosa and lentil dosa (p=0.004). When the satiety scores of traditional and high fiber preparations were analyzed there was significant difference with (p=.001).
Conclusion: High fiber cereal preparations definitely may have a good glycemic response when compared with regular food items. Though there was no significant difference in the glycemic response of other foods, the satiety provided by certain foods like oats, broken wheat, yavam, lentils can have a beneficial impact on the glycemic control for patients with diabetes. High fiber cereal preparations of Kerala cuisine had a higher satiety score compared to traditionalpreparations which should reduce the quantity of food consumed thereby bringing a better glycemic control.
Keywords:
Glycemic response; Satiety; Kerala cuisine; Traditional foods; High fiber preparations
Introduction
Diabetes Mellitus is the most common metabolic disorderaffecting humankind and creating health hazard. The prevalence of diabetes in India found to be 32 million in urban and rural areas during 2000 and predicted to reach 79.4 million by 2030. Kerala is the diabetes capital of India with a prevalence of diabetes as high as 20% - double the national average of 8% [1,2]. In a large multi-center study involving nearly 20,000 subjects, the prevalence of diabetes in Thiruvananthapuram was 17% compared to 15% in Hyderabad and New Delhi, 4% in Nagpur and 3% in Dibrugarh. One study from central Kerala reported a prevalence of diabetes at 20% and prediabetes at 11% [3]. Another study from southern Kerala, showed a wide urban-rural gradient in age-standardized (30-64 years) prevalence of diabetes indicating an important role of lifestyle factors [4]. Though diabetes is associated with aging the recent hike can be attributed to change in life styles, poor dietary habits and increased levels of professional and personal stress events among the youngsters (25-40 years) thus leading to premature deaths and disabling complications. Dietary management is a good strategy in monitoring diabetes and avoiding further complications. Studies indicated that minor millets such as foxtail, little and barnyard are nutritionally superior to conventional food grains and exhibit hypoglycemic effect due to presence of higher proportion of complex carbohydrate, resistant starch and slow rising sugars [5,6]. In addition, millets contain water soluble gum called glucans which improve glucose metabolism. Therefore, the millets are suitable in diabetic diet to improve metabolic control of glucose. We are overfed and under nourished. There is a shift in the staple grains. Earlier we used to eat ragi, bajra, thina, millet, jowar etc. along with rice and wheat. Now we eat mainly polished rice. Satiety is the fullness that persists after eating. It is the quality or state of being fed or gratified to or beyond capacity. This is the most important factor for good glycemic control.
Hence the present study was conducted with objective to compare the glycemic response and satiety of the commonly consumed traditional preparations with that of the high fiber cereal grains in Kerala cuisine.
Need for the study
As there is a paucity of data on glycemic response of Kerala culinery, we selected 10 common traditional Kerala preparations and 10 high fiber cereal preparations containing broken wheat, ragi, yavam, barley and sooji for characterizing glycemic response.
Materials and Methods
Ten healthy volunteers working at Amrita Institute of Medical Sciences (AIMS), aged between 18-55 years of both genders and within a BMI range of 18.5-29.9 kg/m2 were chosen for the study. These subjects had a plasma glucose < 100 mg/dl and had no infection or gastrointestinal disorders. An informed consent approved by the Institutional Ethics Review Committee (IERC) was obtained from each participant.
Subjects having a fasting blood sugar > 126 mg/dl, with lifestylediseases, infections, acute illness, smokers, alcoholics, those on atherapeutic diet, having a family history of diabetes and who had recent weight gain or loss > 3 kg over the past 3 months were excluded from the study.
Ten healthy volunteers were chosen for each recipe. On their first visit, an oral glucose tolerance test was carried out for all the subjects, using 50 g glucose. All the subjects remained on their usual diets, but fasted overnight before the study. Fasting blood samples were taken at 0 min before consumption of the food and the baseline value taken as a mean of these two values. The reference food was consumedimmediately after this and further blood samples were taken at 30, 60, 90 and 120 mins after starting to eat. Blood was obtained by finger-prick using single-use lancing device. Prior to the finger-prick, subjects were encouraged to warm their hand to increase blood flow. Fingers were not squeezed to extract blood from the fingertip in order to minimize plasma dilution.
The same subjects were given 50 g carbohydrate portions of boththe traditional and healthy preparations on separate mornings afterthe oral glucose tolerance test. They consumed the test food over a 10min period. The traditional foods were rice based preparations witha difference only in the method of preparation. On the other hand,the high fiber foods were not rice based but had similar method ofpreparation as that of traditional foods. The preparation method ofthe test foods were as follows: Idli - Make a batter of rice and uraddal, ferment for few hours, and pour it into and idli mould and steam.Appam: Make a thin batter of rice flour with tender coconut, fermentand cook in a frying pan. Idiappam - Make dough of rice flour withwarm water, extrude and steam. Dosa - Make a batter of rice and uraddal, ferment and spread a ladle of batter in a frying pan. Tapioca - Cuttapioca into small cylindrical pieces cook and season. Pathiri - Makedough of rice flour and cook in a frying pan. Upma: Fry rava in a pan,add vegetables and water. Cover and cook till done. The same methodof preparation was followed with ingredients like oats, broken wheat,corn, ragi and barley. The carbohydrate content of the test foodscomputed on the basis of Nutritive Value of Indian Foods (NVIF) isgiven in Table 1.
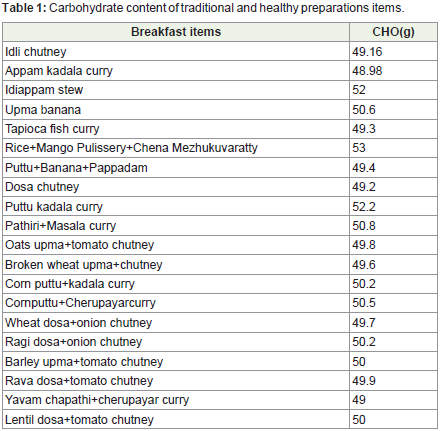
Table 1: Carbohydrate content of traditional and healthy preparations items.
The area under the 2-hour glucose stimulation curve (AUC) was calculated for each subject by summing up the four glucose values obtained after stimulation and similarly for each test meal. Glycemic response of each food item was calculated as follows.
Satiety factor of traditional and high fiber cereal recipes was carried out from each healthy volunteer using the hunger/satiety scaleadapted from Geneen roth. The ratings are as follows:
1 - Hungry, 2-5 - Neutral and 6-10 - Satiety. The preparationswere considered to provide satiety if the values were above 6.
Statistical analysis
Data was analyzed using SPSS 20.0 for windows. Non-parametrictests were used. Comparison of blood glucose response of traditionaland high fiber cereal preparations within groups was done by Wilcoxon signed rank tests.
Results and Discussion
12 healthy volunteers were recruited out of which there were2 drop outs. Out of 10 volunteers who participated in the study 4were males and 6 were females. The mean age of these subjects were25.2+1.5. The anthropometric measurements of healthy volunteersare given in Table 2.
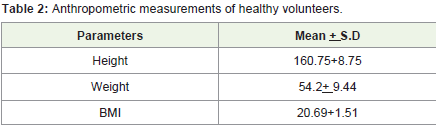
Table 2: Anthropometric measurements of healthy volunteers.
Mean glycemic response of traditional and high fibercereal preparations
The glycemic response of the 10 traditional preparations tested in healthy volunteers is graphically represented in Figure 1. The mean blood glucose values of all traditional preparations at 120 mins were < 105 mg/dl. There was no significant difference in any of these preparations.
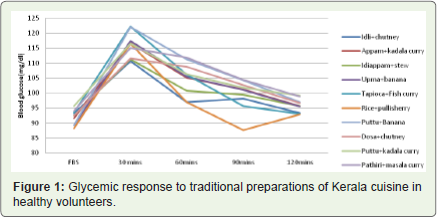
Figure 1: Glycemic response to traditional preparations of Kerala cuisine in healthy volunteers.
Glycemic response of high fiber cereal preparations are shown in Figure 2. From the graph it is observed that foods like oats upma, broken wheat upma, barley upma, rava dosa, yavam chapathi and lentil dosa had a better glycemic response of < 100 mg/dl at 120 mins compared to foods like oats upma, corn puttu, wheat dosa and ragi dosa.
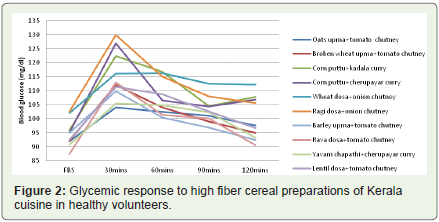
Figure 2: Glycemic response to high fiber cereal preparations of Kerala cuisine in healthy volunteers.
Comparison of mean blood glucose between traditional and high fiber preparations
On comparison with the traditional and high fiber cereal preparations of Kerala cuisine there was a significant difference in the mean blood glucose values at 120 mins between dosa - chutney and wheat dosa - tomato chutney (p=0.001) Figure 3, dosa chutney and ragi dosa - tomato chutney (p=0.041), puttu banana and corn puttu kadala curry (p=0.045) which is shown in Figure 4, puttu bananaand corn puttu - cherupayar curry (p=0.037) depicted in Figure 5. There was no difference in the mean blood glucose values at 120 mins between upma, oats upma and broken wheat upma, dosa and ravadosa, puttu kadala curry and corn puttu kadala curry and cherupayar curry.
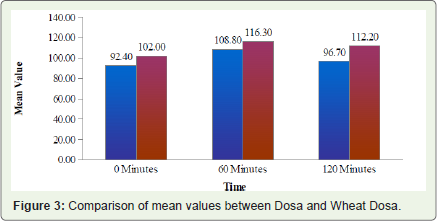
Figure 3: Comparison of mean values between Dosa and Wheat Dosa.
Figure 4: Comparison of mean values between Puttu and Corn puttu kadala curry.
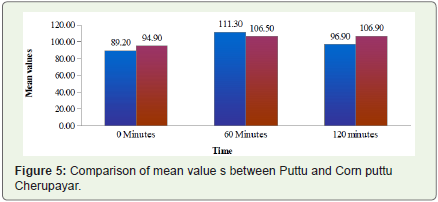
Figure 5: Comparison of mean value s between Puttu and Corn puttu Cherupayar.
Comparison of mean blood glucose between high fiber preparations
The high fiber cereals of similar preparations were compared at 120 mins and it was shown that there is a significant difference in the mean blood glucose of ragi dosa and rava dosa (p=0.004) shown in Figure 6, wheat dosa and ragi dosa with p value 0.001 shown in Figure 7 and wheat dosa and lentil dosa (p=0.004) shown in Figure 8. However there was no difference in the blood glucose values at 120 mins between oats and broken wheat upma. Preparations of corn puttu with cherupayar and kadala curry also did not show any difference. There was no difference in blood glucose values oncomparing wheat dosa with ragi or rava dosa.
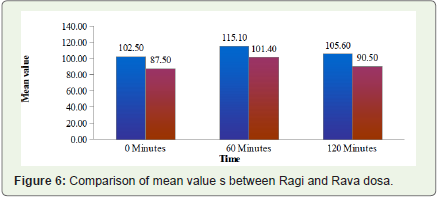
Figure 6: Comparison of mean value s between Ragi and Rava dosa.
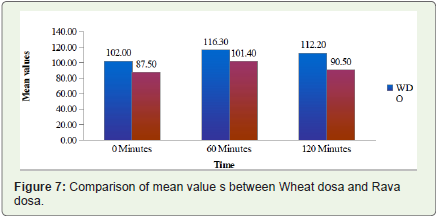
Figure 7: Comparison of mean value s between Wheat dosa and Rava dosa.
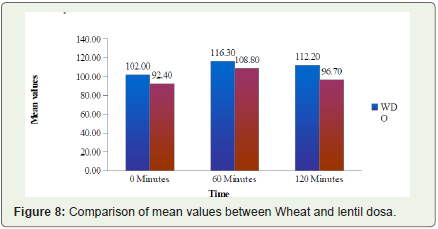
Figure 8: Comparison of mean values between Wheat and lentil dosa.
Hunger and satiety score
The high fiber cereal preparations such as oats upma, broken wheat upma, barely upma, yavam chapathi and lentil dosa had a satiety score of 5.71±0.57 which indicates good satiety on comparison with traditional preparations (3.78±0.46) with a significant difference (P > 0.001) as depicted in Figure 9.
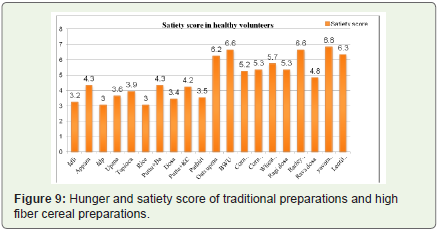
Figure 9: Hunger and satiety score of traditional preparations and high fiber cereal preparations.
Discussion
In our study the preparations from millets and whole grains like broken wheat upma, corn puttu, wheat dosa and ragi dosa showed a better glycemic response when compared with rava upma, puttu and dosa due to low glycemic index in the high fiber preparations of Kerala cuisine.
Oats upma had a better glycemic response than semolina upma as the fiber content in oats is higher than semolina. Also the particle size of oats is bigger than semolina which contributes to a better glycemic response. Diabetic individuals can benefit from diets that are high in(β-glucan, which, as a component of oats) [10].
Broken wheat upma had a significant difference compared to semolina upma. Broken wheat and other whole grains are good sources of magnesium. This mineral is essential to more than 300 enzymes, especially those that contribute to insulin secretion and the release of glucose into the bloodstream. The risk of developing type II diabetes can be up to 30 percent lower in people who consume cracked wheat and other whole grains regularly.
The preparation with millets had a good glycemic response. The millet based diet lowered HbA1c (19.14%), fasting glucose (13.5%), insulin (1.9%) concentrations, total cholesterol concentrations (13.25%), triglyceride concentration (13.51%) and very-low-density lipoprotein cholesterol concentration by 4.5% in the patients with type 2 diabetes [11]. In our study, wheat dosa had a better glycemicresponse compared to dosa made of rice flour and black gram. New research confirms that refined grains, like white rice, pasta or breads, are linked to increased rates of metabolic syndrome, a predictor of both cardiovascular disease and type II diabetes. Metabolic syndrome is far more common in people who eat refined grains instead of whole grains. Cracked wheat and other whole grains decrease the rate of metabolic syndrome when added to a daily diet [12].
Over the past decades, the state of Kerala has witnessed a substantial increase in the prevalence of diabetes mellitus and other non-communicable diseases. This is because of the shift in the consumption pattern of Kerala foods from low cost whole grain cereals to high glycemic index foods. Dietary management is an indispensable tool for the control of glycemia and prevention of complications of diabetes glucose. Since foods with low GI caused significantly lower post prandial glycaemic response, they are considered better for people with diabetes. It has been demonstrated by several researchers over the past decades that consumption of foods having lower glycaemic response and the higher unavailable carbohydrate diets are associated with reductions in body weight, improvement in glycemic control and insulin sensitivity [6]. It has also been shown that low GI diets are associated with reduced risk of type II diabetes and cardiovascular disease [7,8]. GI has become an important tool for helping people select the right food to stabilize blood sugars [9].
The results in our study show that high fiber cereal preparationsof Kerala cuisine had higher satiety similar to a study by M. Bacardi-Gascon with low GI foods [13]. As in our study Ludwig observed 53% and 81% lower food intake after low GI breakfast and lunch respectively, when compared to the intermediate and high GI foods[14].
In a pilot study un published data six healthy subjects ate a 420-calorie breakfast bar after an overnight fast, and then at lunch were offered an all-you-can-eat buffet. When subjects ate a barley bar at breakfast they subsequently ate 100 calories less at lunch than whenthey ate a traditional granola bar for breakfast. Barley high in betaglucan fiber may digest more slowly than standard barley varieties. Researchers at USDA and the Texas Children’s Hospital (TCH)compared the two and concluded that barley may indeed be especiallyappropriate for obese and diabetic patients. These results were similarstudy where the satiety and glycemic response was better with barley upma. Similar to our study, USDA researchers fed barley flakes, barleyflour, rolled oats, oat flour, and glucose to 10 overweight middle-agedwomen, then studied their bodies’ responses. They found that peak glucose and insulin levels after barley were significantly lower than those after glucose or oats. Particle size did not appear to be a factor, as both flour and flakes had similar effects [8].
Holt did not find an association between glucose AUC and satiety scores [9]. Stubbs and Cols (2001). pointed out that more than 26 studies have shown that complex carbohydrates have the highest effect for reducing hunger and limiting the subsequent consumption of energy [10]. In the study conducted by Buyken and cols. an association was observed between low GI foods, with low A1C [11]. In our study the effect on satiety was attributed to the consumption of carbohydrates and fiber. Our results suggest that inclusion of high fiber cereals in Kerala preparations increases the perception on satiety and might be a low cost approach for the control of diabetes [15].
This is the first study in India which has studied the glycemic response of the traditional and healthy preparations of Kerala cuisine.Dietary intervention was focused on the intake from local low-costresources such as nutritionally rich millets, legumes/lentils, and whole grains. Moreover this research recommended foods that are locally available, which provided a better glycemic control.
These data thus provide information helpful in the design of diets for people with diabetes which contain unrefined carbohydrates in a form which is digested and absorbed slowly. However, food culture and preference would still need to be considered [16].
Conclusion
There was a significant difference in the glycemic response at 120 minutes high fiber cereal preparations of Kerala cuisine with fooditems like wheat dosa, ragi dosa and corn puttu. High fiber cerealpreparations definitely showed a good glycemic response. Though there was no significant difference in the glycemic response of other foods, the satiety provided by certain foods like oats, broken wheat, yavam, lentils surely will have a beneficial impact on the glycemic control for patients with diabetes.
References
- Mohan V, Sandeep S, Deepa R, Shah B, Varghese C (2007) Epidemiology of type 2 diabetes: Indian scenario. Indian J Med Res 125: 217-230.
- Reddy KS, Prabhakaran D, Chaturvedi V, Jeemon P, Thankappan KR, et al. (2006) Methods for establishing a surveillance system for cardiovascular diseases in Indian industrial populations. Bull World Health Organ 84: 461-469.
- Menon VU, Kumar KV, Gilchrist A, Sugathan TN, Sundaram KR, et al. (2006) Prevalence of known and undetected diabetes and associated risk factors in central Kerala--ADEPS. Diabetes Res Clin Pract 74: 289-294.
- Kutty VR, Soman CR, Joseph A, Pisharody R, Vijayakumar K (2000) Type 2 diabetes in southern Kerala: variation in prevalence among geographic divisions within a region. Natl Med J India 13: 287-292.
- Kumari S.K, Thayumanavan B (1997) Comparative study of resistant starch from minor millets on intestinal responses, blood glucose, serum cholesterol and triglycerides in rats. J Sci Food Agric.
- Livesey G, Taylor R, Hulshof T, Howlett J (2008) Glycemic response and health--a systematic review and meta-analysis: relations between dietary glycemic properties and health outcomes. Am J Clin Nutr 87: 258S-268S.
- Würsch P, Pi-Sunyer FX (1997) The role of viscous soluble fiber in the metabolic control of diabetes: A review with special emphasis on cereals rich in β-glucan. Diabetes Care 20: 1774-1780.
- Brand-Miller J, McMillan-Price J, Steinbeck K, Caterson I (2009) Dietary glycemic index: health implications. J Am Coll Nutr Suppl: 446S-449S.
- Safraj S, Anish Ts, Vijayakumar K, Kutty VR, Soman CR (2012) Socioeconomic position and prevalence of self-reported diabetes in rural Kerala, India: results from the PROLIFE study. Asia Pac J Public Health 24: 480-486.
- Food and Agriculture Organization of the United Nations (1998) The role of the glycemic index in food choice: Carbohydrates in human nutrition. FAO/WHO pp. 25-30.
- Jimenez-Cruz A, Bacardi-Gascon M, Turnbull WH, Rosales-Garay P, Severino-Lugo I (2003) A flexible, low glycemic index Mexican-style diet in overweight and obese with type 2 diabetes improves metabolic parameters during a 6-week treatment period. Diabetes Care 26: 1967-1970.
- Ludwig DS, Majzoub JA, Al- Zahrani A, Dallal GE, Blanco I, et al. (1999) High glycemic index foods, overeating and obesity. Pediatrics 103: E261-E266.
- Inspiring Good Health Through Cultural Food Traditions (2010) Barley controls blood sugar better. Am J Clin Nutr 91: 90-97.
- Holt SH, Brand Miller JC, Petcoz P (1996) Interrelationships among postprandial satiety, glucose and insulin responses and changes in subsequent food intake. Eur J Clin Nutr 50: 788-797.
- Stubbs JR, Mazlan N, Whybrow S (2001) Carbohydrates, appetite and feeding behavior in humans. J Nutr 131: 2775S-2781S.
- Buyken AE, Toeller M, Heitkamp G, Karamanos B, Rottiers R, et al. (2001) Glycemic index in the diet of European outpatients with type 1 diabetes: relations to glycated hemoglobin and serum lipids. Am J Clin Nutr 73: 574-581.