Review Article
A Review on the Practical Approach toNutritional Management of Preterm Infants: Indian Perspective
Vaidya U1*, Maralakunte H2 and Garg P3
1Department of Neonatology, KEM Hospital, Jawaharlal Nehru Road, Somwar Peth, Pune, India
2Department of Neonatology, Sagar Hospitals, No. 44/54, 30th Cross, Tilaknagar, Jayanagar Extension, Bangalore, India
3Department of Neonatology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India
Corresponding author: Dr. Umesh Vaidya, Department of Neonatology, KEM Hospital, Jawaharlal Nehru Road,Somwar Peth, Pune, India, Tel: 09822031151; E-mail: kemnicu@gmail.com
Citation: Vaidya U, Maralakunte H, Garg P. A Review on the Practical Approach to Nutritional Management of Preterm Infants: Indian Perspective. 02 Indian J Nutri. 2017;4(1):151.
Copyright © 2017 Vaidya U, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 3, Issue: 2
Submission: 07/11/2016; Accepted: 07/02/2017; Published: 09/02/2017
Abstract
Worldwide, more than 15 million babies are born prematurely every year. Of these, 1 million die, and many surviving infants face a lifetime of disability. A striking 24% of the world’s preterm births occur in India, which represents a total of 3.5 million preterm births every year. Infants born prematurely are at a higher risk than term infants for infections, impaired neurodevelopment, and poor growth.
Short and long-term health outcomes can be improved by initiating feeds promptly and advancing progressively. Feeding usually involves multiple approaches such as early parenteral nutrition, orogastric or nasogastric enteral tube feeding, and ultimately oral feeding. The starting feed and the timing of progression depend on an infant’s age and weight at birth, the baby’s ability to coordinate breathing with sucking and swallowing, and gut maturity. The nutrient needs of preterm infants are higher than that of term infants. Parenteral nutrition must supply adequate amino acids and energy. For enteral feeds, mother’s milk is ideal but must be fortified with additional protein, energy, vitamins, and minerals. When the infant is ready for oral feeding, fortified mother’s milk is the first choice. Human milk banks, wherever available, should be considered as the first alternative when mother’s milk is unavailable or insufficient. If both options are not available, the use of nutrient-rich preterm formula is appropriate. To promote intact survival among infants born prematurely, our paper includes a stepwise feeding plan and tools for decision making.
Keywords: Preterm nutrition; Progressive feeding; Growth and development monitoring; Human milk fortification and India
Introduction
Worldwide, more than 15 million babies are born prematurelyevery year-approximately 1 in every 10 newborns. Of these, approximately 1 million die, and many surviving infants face a lifetime of disability [1]. Infants born early are at a higher risk than term infants for infection, sepsis, and death; impaired neurodevelopment;and poor weight gain and body growth [2-4]. The incidence of premature births ranges between 5% and 18% worldwide; Incidence rates in India are mid-range at approximately 13% [5,6], which accounts for 24% of the world’s preterm births. This represents a total of 3.5 million per year, the highest number for any country in the world [5]. There is much room for improvement in the care of preterm babies in India.
The neonatologists from India aim to highlight affordable and effective ways to reduce death and disability among babies born prematurely i.e. increase intact survival. To improve outcomes in thisvulnerable infant population, the focus has been set particularly on nutrition. Prompt and progressive feeding for preterm infants has been endorsed, and the importance of human milk in the feeding regimen has been underscored [7,8].
It is also important to recognize that’s election of how, when, and what to feed depends on the preterm infant’s gestational age and the clinical status at birth and in the weeks there after. Prompt feeding means initiating feeding within hours of birth to emulate in uteronutrient availability. Progressive feeding calls for stepwiseadjustment of nutrient delivery after birth to ensure that nutritional needs of the preterm infant are fully met. In general, the step wise feeding pattern for infants had born prematurely progresses from parenteral to enteral to oral feeding.
Unmet nutritional needs predict poor outcomes
Infants born prematurely, especially with low birth weight, are predisposed to poor outcomes. Notably, they are at risk for infection/ sepsis [9]. Among those who survive, many experience Extra Uterine Growth Restriction (EUGR) or postnatal growth failure, especially if their nutritional intake is low [10,11] and have impaired cognitive development and compromised learning, vision, and hearing [2,12-14].
Infection, sepsis, and mortality
Threats to prematurely born infants such as risk for infection, sepsis, inadequate nutrition, and death are interwoven. Sepsis is a leading cause of preterm infant mortality worldwide [15]. In India, researchers at a tertiary care hospital found that even late preterm infants (n=250) were at 5-fold greater risk for sepsis as compared to term newborns [16]. In another study, low energy intake during the first week of life among preterm infants was correlated with slow growth velocities and risk of adverse outcomes such as sepsis and death [9].
Growth restriction
EUGR is common among preterm infants, occurring in more than 50% of Very Low Birth Weight (VLBW; <1500 g) babies [11].Inadequate postnatal nutrition is an important factor contributing togrowth failure [17]. Results of a large study of Extremely Low Birth Weight (ELBW; <1000 g) infants showed that nearly 90% of Smallfor-Gestational-Age (SGA) babies displayed growth failure at 36weeks of gestational age [18,19].
Impaired neurodevelopment
Approximately 7% of infants born prematurely worldwide are estimated to have some degree of neurodevelopmental impairment, which represents a large social and economic burden [2]. All nutrients support brain development, but certain macro- and micronutrients are particularly important in preterm infants, i.e. protein, glucose, polyunsaturated fatty acids, iron, zinc, iodine, and folate [14]. Evidence shows that nutrient sufficiency in preterminfants positively affects development of sensory, visual, and auditoryfunctions [13,20,21]. Poor early weight gain in preterm infants is associated with abnormal vascularization of the eye, i.e. retinopathy of prematurity, an observation that underscores the importance of nutrients in visual development [22].
Long-term economic burden of preterm birth
In addition to lasting health care costs of preterm birth, thereare long-term financial costs. Health economists have tracked the cost burden of preterm birth based on growth impairment and neurodevelopmental disabilities. In Canada, the added healthcare costs from birth through 2 years were estimated at $13,700 [23]. In the UK, healthcare costs from birth through 18 years were estimated at more than £45,000 ($70,000) [24], whereas lifetime medical cost in the USA was estimated at more than $51,000 [25]. Exact figures of economic burden of preterm births are not available for India, but given the fact that preterm babies require specialized care, there is little doubt that the cost of managing these babies is high.
Nutrition care improves outcomes for preterm infants
Research shows that appropriate nutritional care of preterm infants can positively influence early growth and development as well as long-term outcomes. There is an ever-growing body of evidence showing that prompt provision of parenteral nutrition to preterm infants can improve survival and early outcomes such as growth [26], pulmonary function [27], neurodevelopment [11], and bone maturation [28]. Likewise, early enteral feeding (smallvolume trophic feeds) with gradual progression to full enteral feeding (tube or oral) also yields well-evidenced benefits, such as improving maturation of the gastrointestinal tract and its immune tissues [29],enhancing feeding tolerance [30], assuring adequate growth (weight and length) [31], decreasing the risk of infection and sepsis [10], helping avert cholestasis [31], and lowering the risk of Necrotizing Enterocolitis (NEC) [32]. In babies born prematurely, early enteral feedings enriched with calcium and phosphorus significantly increase bone mineral content during the first 3 months of growth [33].
Breast milk offers benefits to preterm infants. However, studies have shown that the greatest benefits (increased growth and bone mineral content) occur only when human milk is fortified to meet the higher needs of preterm infants [34,35].
Protein and energy intakes in the first week after birth have been shown to influence mental development at age 18 months; specifically, there was a 4.6-point increase in mental development index for every 10 kcal/kg body weight/day of energy intake and an 8.2-point increase for every g/kg body weight/day of protein intake [36].
Cost savings
To date, few studies have examined the cost benefit of specializedparenteral feeding for infants born prematurely. While financial costs of parenteral nutrition therapy are high, health outcome benefits of parenteral feeding for Low Birth Weight (LBW) infants are clearly substantiated [37]. Broader use of standardized parenteral components may help contain costs [37,38]. As preterm infants mature to tolerate enteral feeding, fortified human milk becomes the preferred feeding, and preterm feeding formulas are considered an effective alternative; such special enteral feedings do increase the cost of nutrition care but are likely to be offset by lower short and longterm healthcare use [11].
There is a need for future health economics and outcomes related research studies to assess the "value of nutrition" for preterm infants.In addition, one of the pertinent questions in the current scenario is whether the added costs of prompt and progressive feeding (parenteral feeding, human milk fortifiers, preterm formulas) are offset by lower healthcare costs that go along with improved survival, growth, and development.
In-Hospital and Post-Discharge Preterm Feeding:Practical Issues
Higher nutrient needs
Intrauterine accretion of nutrients occurs mainly in the later part of the third trimester; preterm infants have low body stores of macro and micronutrients at birth, yet they have high requirements to support growth and development [Table 1]. Needs for key nutrients have been estimated on the basis of fetal growth, fetal accretion rate, and intestinal absorption for preterm infants and on thebasis of human milk composition for term infants [39]. Over time, individual infant’s needs may become even greater due to build-up of nutrient deficits resulting from medical and physiological conditions [11,18,40].
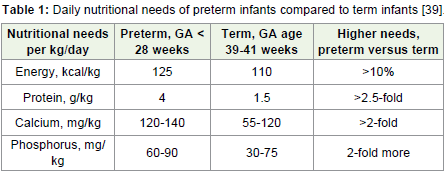
Table 1: Daily nutritional needs of preterm infants compared to term infants [39].
How to feed preterm infants?
Infants born prematurely may lack adequate feeding skills, including sucking and swallowing difficulties, and may experience feeding intolerance due to gut immaturity [11,18,40]. Short- and long-term outcomes can be improved by starting nutrition promptly and advancing progressively [7,11,41]. The initial feeding method depends of the feeding skill of the baby [Table 2] [40].
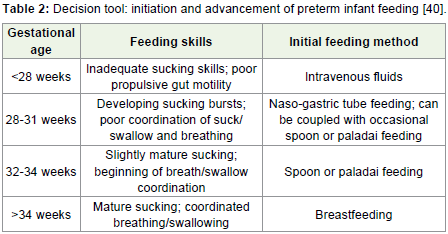
Table 2: Decision tool: initiation and advancement of preterm infant feeding [40].
When to feed preterm infants?
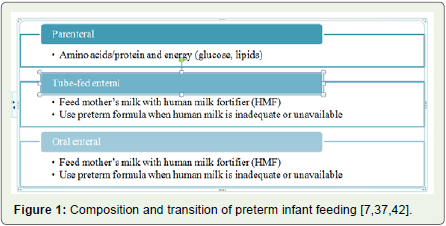
Feeding should be started within 1 to 2 hours of birth [Figure 1] [7,37,42].
Breastfeeding: The gold standard
Some experts advise that all stable LBW infants should be put on their mothers’ breasts. Even in very immature infants who cannot get adequate fluid and nutrients from breastfeeding, sucking at the breast is thought to help build infant feeding skills and enhance milk secretion by the mother (non-nutritive sucking) [40].
Frequency of feeding
The frequency of feeding is decided based on the weight,gestational age, and clinical condition of the infant. The feeds throughnasogastric or orogastric tubes are given as a bolus over 10 to 20minutes. The feeding volumes and frequency of feeds according tothe birth weight have been given in Table 3 [43].
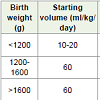
Table 3: Feeding volumes and frequency as per the birth weight of preterm infants [43].
What to feed?
Parenteral nutrition
According to the European Society of Paediatric Gastroenterology,Hepatology and Nutrition (ESPGHAN), European Society for Clinical Nutrition and Metabolism (ESPEN), and the European Society of Paediatric Research (ESPR) guidelines on pediatric parenteral nutrition, amino acid supply initiated on the first postnatal day is generally safe. A minimum of 1.5 g/kg/day to prevent negative nitrogen balance and a maximum of 4 g/kg/day are recommended [44]. Feeding outcomes must be monitored to avoid hyper or hypoglycemia [41]. Parenteral nutritional intake in preterm infants as per National Neonatology Forum (NNF) is given in Table 4 [44].
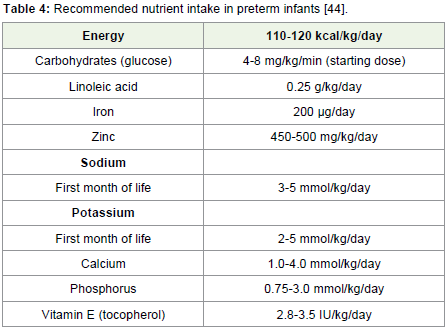
Table 4: Recommended nutrient intake in preterm infants [44].
Enteral and oral feedings
Adequate enteral feeding of preterm low birth weight infants requires attention to supplies of protein and energy, along with specific vitamins and minerals for growth and brain/body development [Table 5] [45].
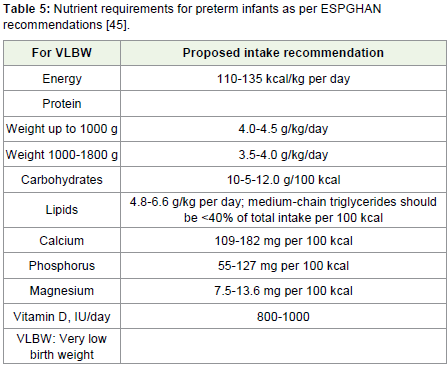
Table 5: Nutrient requirements for preterm infants as per ESPGHAN recommendations [45].
Preterm infants, especially VLBW infants, are at risk of iron deficiency, which may have adverse effects on brain development and function. Dietary intake of iron should be 2 mg/kg/day for infants with birth weight of 1500-2500 g and 2-3 mg/kg/day for infants with birth weight <1500 g. The iron status should be monitored routinely in preterm infants [46]. Although there are no specificrecommendations for the assessment of iron status in preterm infants, initial screening of iron status at 2 months or at discharge (whicheveris earlier) is considered prudent. A recheck of hematological status can be considered at the age of 6 months [47].
Fortified human milk or preterm formula
For low birth weight infants (ELBW and VLBW), neither human milk nor standard term infant formula can provide necessary levels of nutrients for catch-up growth [10]. For this reason, there is a need to provide feedings fortified with extra proteins (or amino acids), energy, vitamins, and minerals.
Fortified human milk
There is considerable evidence supporting the benefits of mother’s milk that has been fortified, usually using a commercial formulation of Human Milk Fortifier (HMF) [46]. Fortification increases the nutrient content of milk without compromising on its benefits. Experimental studies suggest that the net nutrient retention with HMF is nearly more than the expected intrauterine rates of accretionin preterm infants [40]. A Cochrane review in 2004 suggested a short term but significantly greater weight gain, head circumference gain, and linear growth in preterm infants fed with fortified human milk as compared to the breast milk only group [34]. However, in a recent update of this Cochrane review, the authors concluded that the data available on human milk fortification is limited and does not provide strong evidence on the benefits of multi-nutrient fortified breast milk compared with unfortified breast milk in preterm infants [48]. The review suggested that human milk fortification was associated with slightly higher in-hospital growth rates. The manufacturers of HMF in India are limited, and there is an urgent need of introducing a high quality HMF in the Indian market.
Human milk fortification in preterm infants <32 weeks is started once they reach 150 mL/kg/day of enteral feeds at a dose recommended by the manufacturer. They are also started on iron at 4-6 weeks at a dose of 2 mg/kg/day. Fortification is continued until the infant reaches 40 weeks or attains 2.5 kg, whichever is earlier [40].
Preterm formula
When the supply of mother’s milk is insufficient or unavailable, an infant formula designed for preterm infants is considered the next best option, as advised by both European and US pediatric nutrition experts [10,41,45].Although there is little evidence on when the HMF or preterm formula should be stopped, it is preferable to change the preterm formula to standard formula or stop adding HMF when infants reach 2.5 kg of weight and 40 weeks of gestational age [49].
In summary, preterm infants have high requirements for macroandmicronutrients to promote survival, maintain growth, and support brain and body development. Regardless of whether the infant is being fed parenterally, enterally, or orally, caregivers must be mindful of providing nutrient content that will meet each infant’s needs. For enteral tube feeding and oral feeding, mother’s milk is always preferred and considerable evidence supports its benefits. However, nutrients must be added by mixing expressed breast milk with HMF to achieve adequate supplies of protein, energy, and vital vitamins and minerals.
Human Milk Banking: The Viable Alternative
Pasteurized donor human milk is considered the next best option when mother’s milk is unavailable or insufficient [49]. The World Health Organization (WHO) states that human milk from other sources should be the first alternative when mother’s milk is unavailable and Human Milk Bank‘s (HMBs) should be available in appropriate situations [50].
Given the highest number of low birth weight infants in India with significant morbidity and mortality, the concept of human milk banking can be beneficial in this population. However, human milk banking is still in its infancy in India owing to the lack of awareness and leadership, infrastructural and maintenance costs. The first HMB was founded in the year 1989 in Mumbai and currently there are approximately 25 HMBs across India. Currently, there is a dire need for HMBs at all levels, including level II and III facilities [50].
Outcome Monitoring and Post-Discharge Follow-Up
The guiding principles for feeding preterm infants are (1) to provide nutrients to approximate the rate of growth for a normal fetus of the same postmenstrual age, (2) to maintain normal concentrations of nutrients in blood and tissues, and (3) to achieve acceptable functional development [51].
Monitoring
For anthropometric measures, daily monitoring of weight and weekly measurement of length and head circumference are recommended in the Neonatal Intensive Care Unit (NICU), with measurement of all 3 parameters at each clinical visit after discharge. For growth assessment, plotting results (by sex) for weight-for-age, length-for-age, and head circumference by gestational age using the Fenton 2013 charts for preterm infants up to 50 weeks of gestation is advised [Figure 2] [52].
Growth restriction is flagged by plots falling downward across percentile lines, and growth failure is likely for infants who fall belowthe 10th percentile. For infants older than 50 weeks of gestation, growth is plotted for corrected age on the WHO growth charts for infants (http://www.who.int/childgrowth/standards/en/).
Importance of Catch-Up Growth
The term "catch-up growth" refers to increase in the weight or length gain velocity after a period of nutrition restriction. Majority of preterm infants have poor growth with a weight that is lower than the infant’s birth centile at discharge. In addition, catch-up growth in preterm infants after discharge occurs at a different phase compared to term infants after birth and therefore, the long-term consequences also vary accordingly [52,53]. The extent to which catch-up growth occurs depends on several factors, including the severity and duration of restriction. A weight gain of at least 20 g/day is typically acceptable in a healthy breast fed preterm infant after discharge [52].
Follow-Up with Infants and Parents
Early nutritional deficits in preterm infants have serious adverseconsequences [2,12,14,17-19], and nutritional interventions can improve outcomes [10,11,26-28,31,32]. Thus, regular post-discharge follow-up is highly important for preterm infant growth monitoring and for parent counseling on feeding [54].
Summary and Conclusion
Neonatologists from India have designed nutrition care guidelines and decision tools for feeding infants who are born prematurely. The rates of premature births range between 5% and 18% worldwide. The rates of premature births in India are mid-range at 13%; therefore, there is much room for improvement in India as compared toelsewhere in the world.
• Recommendations for feeding preterm infants include prompt and progressive feeding by way of early parenteral feeding, advancing to orogastric or nasogastric enteral tube feeding, and ultimately the use of oral feeding.
• The importance of human milk for feeding infants born prematurely is emphasized, but fortification with Human MilkFortifier (HMF) to ensure healthy growth and development is also advised. If mother’s milk is not available and donor milk is available, it should be used. However, if human milk is limited in supply or unavailable, the use of preterm infant formulas is advised.
• The objective of providing adequate and timely nutrients and maintaining hygiene in preterm infants is to reduce the risk of infection/sepsis, improve catch-up growth, and reduce the incidence of cognitive impairment and developmental delays among infants born prematurely in India.
• Attentive monitoring of growth and development through the first year of life and beyond is advised to ensure that each infant is fed nutrients sufficient to support both physical growth and neurodevelopment.
Prompt progressive feeding along with robust follow-up and outcome monitoring is an effective strategy to promote intact survival of infants born prematurely. Moving forward, this up-todate preterm feeding guidance can be used as a basis for nutrition education and training programs for physicians and other neonatal care professionals throughout India. Importantly, there is a need for the development of Indian policies and direct support to enhance hospital and community sites for the care of preterm infants,including equipment, staff training, infant follow-up, and parent counseling services.
Acknowledgements
We would like to thank Abbott Healthcare Pvt. Ltd. for fundingthe work. We would like to acknowledge BioQuest Solutions Pvt. Ltd.for its manuscript review and editing services.
References
- World Health Organization, March of Dimes, PMNCH, Save the Children (2012) Born too soon: The Global Action Report on Preterm Birth. Genev 1-112.
- Blencowe H, Lee AC, Cousens S, Bahalim A, Narwal R, Zhonget N, et al. (2013) Preterm birth-associated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatr Res 74 Suppl 1: 17-34.
- Ochiai M, Kinjo T, Takahata Y, Iwayama M, Abe T, et al. (2014) Survival and neurodevelopmental outcome of preterm infants born at 22-24 weeks of gestational age. Neonatology 105: 79-84.
- Saigal S, Doyle LW (2008) An overview of mortality and sequeale of preterm birth from infancy to adulthood. Lancet 371: 261-269.
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, et al. (2012) National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 379: 2162-2172.
- Healthy Newborn Network (2012) Born too soon wall chart of preterm birth by country.
- Ehrenkranz RA (2007) Early, aggressive nutritional management for very low birth weight infants: what is the evidence? Semin Perinatol 31: 48-55.
- Bhatia J (2013) Human milk and the premature infant. Ann Nutr Metab 62 Suppl 3: 8-14.
- Ehrenkranz RA, Das A, Wrage LA, Poindexter BB, Higgins RD, et al. (2011) Early nutrition mediates the influence of severity of illness on extremely LBW infants. Pediatr Res 69: 522-529.
- Groh-Wargo S, Sapsford A (2009) Enteral nutrition support of the preterm infant in the neonatal intensive care unit. Nutr Clin Pract 24: 363-376.
- Su BH (2014) Optimizing nutrition in preterm infants. Pediatr Neonatol 55: 5-13.
- Keunen K, van Elburg RM, van Bel F, Benders MJ (2015) Impact of nutrition on brain development and its neuroprotective implications following preterm birth. Pediatr Res 77: 148-155.
- Algarin C, Peirano P, Garrido M, Pizzaro F, Lozoff B (2003) Iron deficiency anemia in infancy: long-lasting effects on auditory and visual system functioning. Pediatr Res 53: 217-223.
- Ramel SE, Georgieff MK (2014) Preterm nutrition and the brain. World Rev Nutr Diet 110: 190-200.
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. (2015) Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet 385: 430-440.
- Femitha P, Bhat BV (2012) Early neonatal outcome in late preterms. Indian J Pediatr 79: 1019-1024.
- Cooke RJ, Ainsworth SB, Fenton AC (2004) Postnatal growth retardation: a universal problem in preterm infants. Arch Dis Child Fetal Neonatal Ed 89: F428-430.
- Dusick AM, Poindexter BB, Ehrenkranz RA, Lemons JA (2003) Growth failure in the preterm infant: can we catch up? Semin Perinatol 27: 302-310.
- Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, et al. (2007) Trends in neonatal morbidity and mortality for very low birth weight infants. Am J Obstet Gynecol 196: 147 e141-e148.
- O'Connor DL, Weishuhn K, Rovet J, Mirabella G, Jefferies A, et al. (2012) Visual development of human milk-fed preterm infants provided with extra energy and nutrients after hospital discharge. JPEN J Parenter Enteral Nutr 36: 349-353.
- Verner A, Craig S, McGuire W (2007) Effect of taurine supplementation on growth and development in preterm or low birth weight infants. Cochrane Database Syst Rev CD006072.
- Hellstrom A, Ley D, Hansen-Pupp I, Niklasson A, Smith L, et al. (2010) New insights into the development of retinopathy of prematurity--importance of early weight gain. Acta Paediatr 99: 502-508.
- Johnston KM, Gooch K, Korol E, Pamela Vo, Oghenowede Eyawo, et al. (2014) The economic burden of prematurity in Canada. BMC Pediatr 14: 93.
- Mangham LJ, Petrou S, Doyle LW, Draper ES, Marlow N (2009) The cost of preterm birth throughout childhood in England and Wales. Pediatrics 123: e312-e327.
- McCabe ER, Carrino GE, Russell RB, Howse JL (2014) Fighting for the next generation: US prematurity in 2030. Pediatrics 134: 1193-1199.
- Adamkin DH (2007) Early aggressive nutrition: parenteral amino acids and minimal enteral nutrition for extremely low birth weight (<1 000 g) infants. Minerva Pediatr 59: 369-377.
- Eleni-dit-Trolli S, Kermorvant-Duchemin E, Huon C, K Husseini, M-L Brunet, et al. (2009) Early individualized parenteral nutrition for preterm infants. Arch Dis Child Fetal Neonatal Ed 94: F152-153.
- Pereira-da-Silva L, Costa A, Pereira L, Filipe A, Virella D, et al. (2011) Early high calcium and phosphorus intake by parenteral nutrition prevents short-term bone strength decline in preterm infants. J Pediatr Gastroenterol Nutr 52: 203-209.
- Lafeber HN, Westerbeek EA, van den Berg A, Fetter WP, van Elburg RM (2008) Nutritional factors influencing infections in preterm infants. J Nutr 138: 1813S-1817S.
- Schanler RJ, Shulman RJ, Lau C, Smith EO, Heitkemper MM (1999) Feeding strategies for premature infants: randomized trial of gastrointestinal priming and tube-feeding method. Pediatrics 103: 434-439.
- Loomis T, Byham-Gray L, Ziegler J, Parrott JS (2014) Impact of standardized feeding guidelines on enteral nutrition administration, growth outcomes, metabolic bone disease, and cholestasis in the NICU. J Pediatr Gastroenterol Nutr 59: 93-98.
- Schurr P, Perkins EM (2008) The relationship between feeding and necrotizing enterocolitis in very low birth weight infants. Neonatal Netw 27: 397-407.
- Lapillonne A, Salle BL, Glorieux FH, Claris O (2004) Bone mineralization and growth are enhanced in preterm infants fed an isocaloric, nutrient-enriched preterm formula through term. Am J Clin Nutr 80: 1595-1603.
- Kuschel CA, Harding JE (2004) Multicomponent fortified human milk for promoting growth in preterm infants. Cochrane Database Syst Rev CD000343.
- Liu TT, Dang D, Lv XM, Wang TF, Du JF, et al. (2015) Human milk fortifier with high versus standard protein content for promoting growth of preterm infants: A meta-analysis. J Int Med Res 43: 279-289.
- Stephens BE, Walden RV, Gargus RA, Tucker R, McKinley L, et al. (2009) First-week protein and energy intakes are associated with 18-month developmental outcomes in extremely low birth weight infants. Pediatrics 123: 1337-1343.
- Adamkin DH, Radmacher PG (2014) Current trends and future challenges in neonatal parenteral nutrition. J Neonatal Perinatal Med 7: 157-164.
- Simmer K, Rakshasbhuvankar A, Deshpande G (2013) Standardized parenteral nutrition. Nutrients 5: 1058-1070.
- Lapillonne A (2014) Feeding the preterm infant after discharge. World Rev Nutr Diet 110: 264-277.
- Sankar MJ, Agarwal R, Mishra S, Deorari AK, Paul VK (2008) Feeding of low birth weight infants. Indian J Pediatr 75: 459-469.
- American Academy of Pediatrics Committee on Nutrition. Pediatric Nutrition (2014) 7th ed. Elk Grove Village, IL
- Newborn nursing for facility based care Level II units (2015) Who Collaborating Centre for Training and Research in Newborn Care. All India Institute of Medical Sciences, New Delhi.
- 43.Evidence based Clinical Practice Guidelines (2015) National neonatology Forum, India.
- Koletzko B, Goulet O, Hunt J, Krohn K, Shamir R, et al. (2005) Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J Pediatr Gastroenterol Nutr 41 Suppl 2: S1- S87.
- Agostoni C, Buonocore G, Carnielli VP, De Curtis M, Darmaun D, et al. (2010) Enteral nutrient supply for preterm infants: Commentary From the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr 50: 85-91.
- Giribaldi M, Cavallarin L, Baro C, Di Nicola P, Coscia A, et al. (2012) Biological, nutritional and clinical aspects of feeding preterm infants with human milk. J Biol Regul Homeost Agents 26: 9-13.
- Rao R, Georgieff MK (2009) Iron therapy for preterm infants. Clin Perinatol 36: 27-42.
- Brown JVE, Embleton ND, Harding JE, McGuire W (2016) Multi-nutrient fortification of human milk for preterm infants. Cochrane Database of Systematic Reviews.
- Gupta ML (2015) Care of low birth weight (LBW) babies. Module for training of specialist in pediatrics on newborn care. 1-42.
- Bharadva K, Tiwari S, Mishra S, Mukhopadhyay K, Yadav B, et al. (2014) Human milk banking guidelines. Ind Pediatr 51: 469-474.
- Ehrenkranz RA (2014) Nutrition, growth and clinical outcomes. World Rev Nutr Diet 110: 11-26.
- Fenton TR, Kim JH (2013) A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr 13: 59.
- Moyer-Mileur LJ (2007) Anthropometric and laboratory assessment of very low birth weight infants: the most helpful measurements and why. Semin Perinatol 31: 96-103.
- Ahmed AH, Sands LP (2011) Effect of pre- and postdischarge interventions on breastfeeding outcomes and weight gain among premature infants. J Obstet Gynecol Neonatal Nurs 39: 53-63.