Research Article
A Case Control Study on Macro Nutrients Intake of Children with Autism Spectrum Disorder
Komal Srivastava1, Meera Raman2, Anjan Bhattacharya3
1Senior Dietician, Apollo Gleneagles Hospitals, Kolkata, West Bengal, India
2Head, Department of Foods and Nutrition, RVS College of Arts and Science, Sulur, Coimbatore, India
3Consultant Developmental Paediatrician, Apollo Gleneagles Hospitals, Kolkata, West Bengal, India
Corresponding author: Komal Srivastava, Senior Dietician, Apollo Gleneagles Hospitals, Kolkata, West Bengal, India; E-mail: komal_srivastava2007@yahoo.com
Citation: Srivastava K, Raman M, Bhattacharya A. A Case Control Study on Macro Nutrients Intake of Children with Autism Spectrum Disorder. IndianJ Nutri. 2016;3(2): 134.
Copyright © 2016 Srivastava K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 3, Issue: 2
Submission: 07/07/2016; Accepted: 05/08/2016; Published: 10/08/2016
Abstract
Background: Children with Autism Spectrum Disorder (ASD) have various eating abnormalities like restrictive eating habits, poor table behaviour, foodrefusal and food selectivity.
Objective: The present study relates to a survey of 24 hours diet recall and daily nutritional intake (total calories, protein) in ASD children against normalhealthy children within the age group of 2-6 years of age.
Method: 40 diagnosed cases of ASD children were selected with similar sample size of normal healthy children free from any disease or disorder.Questionnaire was prepared, validated and then survey on 24 hours diet recall was conducted. The data was obtained from mothers of children in both groupsafter the signing of consent form.
Results: The analysis was conducted using SPSS 20.0. The result showed that ASD children were deficient in all categories of daily supply of nutrients ascompared to controls. The mean standard deviation was done as a part of analysis. The data was further analysed using “t” test. The mean standard deviationof energy and proteins was calculated separately which showed deficiency in both domains. There was subsequent statistical difference found in nutrient intakebetween two groups at 5 % level of significance.
Conclusion: The survey conducted showed significant difference in the dietary intake of macronutrients among the ASD children.
Keywords: Autism Spectrum Disorder; Calories; Proteins; 24 hours diet recall.
Introduction
Nutrition is what we get from food we eat. It’s that part of food that gives our bodies what they need to function- to live and movearound, to think and breathe, play and work. Without nutrition wecould not survive for very long [1].
The science of nutrition helps us to improve our food choices byidentifying and amount of nutrition we need, the best source of thosenutrients and the other components in foods that may be helpful orharmful [2].
Good nutrition is of paramount importance for both infants andchildren [3].
Optimum nutrition is important during childhood for threemajor reasons:
• It allows the child to grow and develop and reach its geneticpotential for physical size and intelligence.
• Childhood offers an important opportunity to establishhealthy eating patterns and food preferences. Diet habitslearned during this period often become lifelong habits.
• A poor quality diet can increase risk of chronic disease laterin life [2].
Malnutrition includes both under and over nutrition. Indeveloping countries under nutrition is a major public healthproblem. Under nutrition which is better understood than intelligencebehavior or cognition is defined as a state wherein adequate nutrientsare not delivered to the cells to provide the substrate for optimalfunctioning [4].
A diet survey provided information about dietary intake patternsof specific food consumed and estimated nutrients intakes. Itindicates relative dietary inadequacies, which is helpful in planninghealth education activities. Diet history are the diet recalls, generallycovering 24 hours. It can be easily elicited from most subjects. 3days food records provided a reasonable way to obtain a qualitativeestimate of nutrient intakes. Food record maintained by subjects for 1to 7 days can be used to know the diet history.
In 24 hours diet recall method, a set of standardized cups suited tolocal conditions are used. Information on the total cooked amount ofeach preparations is noted in terms of standardized cups. The intakeof each food items by specific individual in the family such as thepre school child, adolescent girl or pregnant or lactating woman isassessed by using cups [5].
In 24 hours diet recall method, dietary data is obtained from therespondent through an oral questionnaire of diet survey using a set ofstandardized cups suited to local conditions [6].
24 hours diet recall method is also a report of daily habits, butinterviewed or written information about the previous day’s intake.The participants has to remember the actual food consumed andgive information on portion weights from memory. The respondentsburden for a single 24 hour recall is less than for several days for foodrecords and the method is typically used for determining averageusual intake of a large population / group [7].
The term Autism Spectrum disorder (ASD) refers to range of neurodevelopmental disorders that include the more specific diagnoses ofautism, Asperger syndrome, and pervasive developmental disordernot otherwise specified [8]. The defining features of ASD includeimpairments in social interaction, communication, imagination,restricted interest, and stereotypic behaviours. These symptomsrange in severity from mild to debilitating and usually persistthroughout the lifespan [9]. In addition to the symptoms used indiagnosis, several serious co morbid conditions are also commonlyassociated with ASD including intellectual disability, depression, andepilepsy [10]. Current estimates suggest that the prevalence of ASD isapproximately 6.7 cases per 1000 children or approximately 1 in every150 children [11].
While the etiology of ASD remains unknown, emerging evidencesuggests multiple gene defects may be involved in tandem with anenvironmental catalyst [12]. The ongoing confusion regarding theetiology of ASD has lead to the consideration of many possible causes.Often these potential causes are translated into treatments andthen propagated to the public before sufficient evidence regardingeffectiveness or safety exists [13].
Food preferences are shaped by a combination of geneticand environmental factors. The development of children’s foodpreferences involves a complex interplay of genetic, familial andenvironmental factors. There is evidence of a strong genetic influenceon appetite traits in children, but environment plays an important inmodelling children’s eating behaviour. Satiety is closely related to dietcomposition, and foods with low energy density contribute to preventovereating. Food preferences are the product of an interplay betweengenetic and environmental factors that result in substantial individualdifferences in the extent to which children are suspicious and fussyabout food in general and their likes and dislikes for specific foods.To encourage a healthy attitude to food and prevent overweight, oneshould monitor children’s growth, dietary habits and life style andparents strategies (control or disinhibition). A child’s dietary practiceshould be investigated at different ages with particular attention tothe overall diet quality (how many times, the variety of foods) and selfregulation [14].
The purpose of this study was to ascertain, if there is any statisticalco relation between the macronutrients intake of calories and proteinin ASD and normal children of same age group. The focus of thisstudy is to explore these macronutrient deficiencies in these childrenin Indian set up as there are literally very few studies done on it. Thiswill help in turn give an insight of their dietary patterns and helpidentify malnutrition if any and thus will help care givers and parentsto these ASD children to overcome it.
Methods
The study was approved by Ethics Committee. 40 diagnosed casesof ASD children from the age group of 2-6 years of age were includedin the study. The normal subjects/ control (n=40) were selected fromthe school randomly. Questionnaire and was designed to collect datafrom mothers. Consent from mothers were taken prior to the survey.After preparing the questionnaire and validating it with a pilot study,the survey was carried out to collect information. The data wascollected in one to one process by speaking to mothers of each child.24 hours diet recall was taken from mothers in order to calculateon energy and protein intake of children. Cups and glasses werestandardized and were used for collecting information accurately.The data was analysed statistically using SPSS Version 20.0. The meanstandard deviation of macronutrients (calories and proteins) wascalculated. Each of them were further subjected to “t” test to see thesignificance (p < 0.05).
Results and Discussion
Table 1 shows the mean standard distribution of energy andprotein intake of ASD and normal children. The mean of energywas found to be significantly on the lower side compared to normalchildren of the same age group. The mean (s.d) of daily energy intakewas 895.00 (147.54) and 1388.75 (149.13) for cases and control grouprespectively.
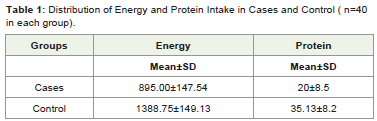
Table 1: Distribution of Energy and Protein Intake in Cases and Control ( n=40in each group).
Similarly, the intake of protein was also calculated and the mean(s.d) was found to be 20 (8.5) and 35.13 (8.2) in cases and controlgroup children.
Parents of children with ASD commonly report concerns regarding feeding difficulties and poor nutrition. Feeding difficulties,in the form of undesirable mealtime behaviours and/or skill deficits,can cause parental concern and impact on family dynamics. Poornutrition can have an impact on development and health issues [15].
Figure 1 and Figure 2 depicts the energy and protein intake within two groups.
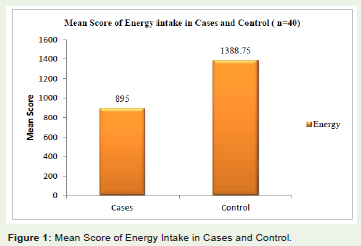
Figure 1: Mean Score of Energy Intake in Cases and Control.
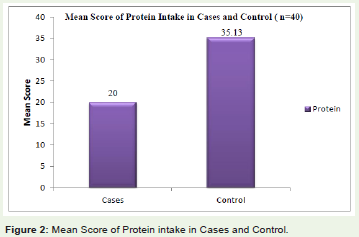
Figure 2 : Mean Score of Protein intake in Cases and Control.
The data collected was further analysed using “t” test. Table 2 andTable 3 represents the energy and protein intake of children of bothgroups. These macronutrients intake were found to be statisticallysignificant.
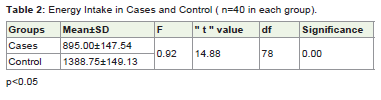
Table 2: Energy Intake in Cases and Control ( n=40 in each group).
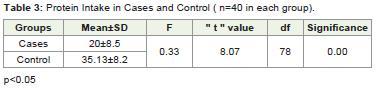
Table 3: Protein Intake in Cases and Control ( n=40 in each group).
(p< 0.05) thus proving to malnutrition in ASD children.
Inadequate nutrient intake of children with autism spectrumdisorder (ASD) have been reported. The study examined thenutritional statuses of children with ASD and nutritional intake.These children consumed significantly fewer macronutrientscompared with children without ASD. Thus results suggests thatreduced macronutrient intake are quite common among childrenwith ASD [16].
Conclusion
Over all, according to the study there seems to be existingsignificant difference between the macronutrient intake of AutismSpectrum Disorder and normal children within the same agegroup in Indian children. Further research can be conducted to seeother nutrient intake and there deficiencies in the ASD children inIndia. Apart from it, the parents and care givers should be givenregular counseling/ training sessions by health professionals whichwill educate them regarding healthy eating habits to overcomemalnutrition within these children.
This article is for Phd study
There is no conflict of interest to be declared
This is a self funded study
References
- Simons R (2009) Nutrition and Poverty. (1st edition) Alpha House Publishing: New York.
- Insel P, Ross D, Mohan KM, Bernstein M (2011) Nutrition. (4th edition) Jones and Bartelett Publishers, USA.
- Lutz CA, Przytulski KRF (2011) Nutrition and Diet Therapy- Evidence Based Application. (4th edition) Jaypee Publication: New Delhi.
- Banji MS, Swamy KK, Brahmman GNV (2009) Text book of Human Nutrition (3rd edition) Oxford and IBH Publishing Co. Pvt. Ltd: New Delhi.
- Srilakshmi B (2012) Nutrition Science. ( 4th edition) New Age International Publishers: New Delhi.
- Thimmayamma BVS, Rav P, Damayanti K (2009) Dietary Assessment as a part of Nutritional Status. In: Text book of Human Nutrition (3rd edition) Oxford and IBH Publishing Co. Pvt. Ltd: New Delhi.
- Bingham S, Dietary Assessment. In: Jim Mann and A. Steward Trusswell (eds) (2008) Essential of Human Nutrition ( 3rd edition) Oxford University Press: New York.
- Sturmey P, Fitzer A (2007) Autism Spectrum disorders: Applied Behaviour Analysis, Evidence and Practice. Austin Tx: Pro Ed.
- National Research Council. In C. Lord and J.P. Mc Gee (Eds.) (2001) Educating children with autism. Washington, DC: National Academy Press.
- Filipeck PA, Accardo PJ, Baaraneck GT, Cook EH Jr, Dawson G, et al. (1999) The screening and diagnosis of Autism spectrum Disorders. J Autism Dev Disord 129: 439-484.
- Centres for disease Control and Prevention, Prevalence of Autism Spectrum Disorders- Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2007. Morbidity and Mortality Weekly Reports. CDC Surveillance Summaries. 56: 1-11.
- Cusco I, Medrano A, Gener B, Vilardell M, Gallastegui F, et al. ( 2009) Autism Specific Copy number variants further implicate the phosphatidylinositol signalling pathway and the glutamatergic synapase in the eitiology of the disorder. Hum Mol Genet 18: 1795-1804.
- Heflin LJ, Simpson RL (1998) Intervention for children with autism: Prudent choice in the world of exaggerated claims and empty promises. Part 1: Intervention and treatment option review. Focus on Autism and Other Developmental Disabilities. 13: 194-211.
- Scaglioni S, Arrizza C, Vecchi F, Tedeschi S (2011) Determinants of children’s eating behaviour. Am J Clin Nutr 94: 6.
- Marshall J, hill RJ, Zivani J, Dodrill P (2014) Features of feeding difficulty in children with Autism Spectrum Disorder. In J S speech Lang Pathol 16: 151-158.
- Liu X, Liu J, Xiong X, Yang T, Hou N, et al. (2016) Correlation between Nutrition and Symptoms : Nutritional Survey of Children with Autism Spectrum Disorder in Chongqing, China. Nutrients 8: 294.