Research Article
Sodium and Pottassium Contents of CommonSeasonings Used in Cooking on the Jos Plateau
Basil N Okeahialam1*, George ON Echeonwu2 and Boniface N Duru2
1Department of Medicine, Jos University Teaching Hospital, Jos, Nigeria
2Federal College of Veterinary and Medical Laboratory Technology, National Veterinary Research Institute, Vom, Jos, Nigeria
Corresponding author: Prof. Basil N Okeahialam, Department of Medicine, Jos University Teaching Hospital, Jos, Nigeria. Phone: 234 805 1499 271;; E-mail: basokeam@yahoo.com
Citation: Okeahialam BN, Echeonwu GO, Duru BN. Sodium and Pottassium Contents of Common Seasonings Used in Cooking on the Jos Plateau. Indian J Nutri. 2015;2(2): 115.
Copyright © 2015 Okeahialam BN, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 2, Issue: 2
Submission: 19/11/2015; Accepted: 30/11/2015; Published: 05/12/2015
Abstract
Background: Hypertension is prevalent in Africa with an established role for dietary sodium. Also the low potassium in the diet of Africans is said to playa significant role in the disease and its complications. With most populations unable to meet their potassium needs through fruits and vegetable intake, itbecomes necessary to look for convenient and culturally acceptable means of meeting the requirement. As most sodium intake is through dietary ingestion oftable salt in cooked and processed food, it would be very important to establish sodium and potassium contents of common seasonings used in cooking. Wetherefore sought to determine the sodium and potassium contents of common seasonings used in cooking in our environment. That way we would be in anevidence-based position to know which ones to recommend.
Methods: We procured from the open market in Jos, common seasonings used to cook in our environment, (a commercial seasoning powder, 2commercial seasoning cubes, table salt, traditional rock salt and traditional seasoning powder) analyzing them for sodium and potassium contents aftermaking standard solutions from each.
Results: Table salt had the highest sodium and lowest potassium contents. The sodium levels fell with a slight rise in potassium when it came to thecommercially produced seasonings. The traditional seasonings had yet lower sodium and much higher potassium contents with sodium/potassium ratio beinglowest for “tooka”, a traditional seasoning powder.
Conclusion: Given the foregoing, traditional seasonings especially “tooka” would be the recommended seasoning in our environment for a favourableimpact on individual and population blood pressure by reducing dietary sodium/potassium ratio.
Keywords: Seasonings; Traditional; Commercial; Cooking; Blood pressure
Introduction
It has been known for long that a direct and continuousrelationship exists between dietary sodium (Na) intake and bloodpressure; the result of which is higher prevalence of hypertension andassociated cardiovascular diseases in those whose dietary intake ofsodium is high [1,2]. This dietary salt and blood pressure responsevaries in the population with some individuals more sensitive thanothers [3]. Africans are known to express high salt sensitivity and thisis one of the explanations for a higher prevalence of hypertension inthem [4]. On the contrary, potassium (K) intake is inversely related to systolic and diastolic blood pressures, an effect thought to play asignificant role in the high prevalence of hypertension in blacks [5].Independent of its effect on blood pressure, high intake of potassiumreduces incidence of cardiovascular and cerebrovascular accidents[6]. The effects of both sodium and potassium are closely related; andhuman studies show that blood pressure raising potentials of highsodium intake are blunted by potassium supplementation [7].
One of the patient related barriers to hypertension control inAfricans is dietary especially low potassium and high sodium intake[8]; hence the dietary recommendation to increase potassium and reduce sodium in order to control hypertension. In sub-Saharan Africasalt consumption is mainly in the diet. This is from the addition of saltduring cooking and at table as well as the use of flavourings in cubesand powder form, since the use of processed food is not so common[9]. Since life style and dietary modifications are most successfulif tailored to customs and tradition [10], we decided to comparesodium and potassium contents of common seasonings (traditionaland commercially prepared) used in cooking in our environmentagainst that of table salt. This is to put us in a strong evidence basedposition to advise our patients on dietary salt intake while suggestingculturally sensitive ways to reduce sodium and increase potassium;since the food industry hardly includes appropriate labeling aboutsalt content on products. Successful attainment of these goals helps inhypertension prevention and control. This derives from the fact thatmodest reductions in dietary salt substantially reduce cardiovascularevents thus reducing medical costs [11]; and should be a target forpublic health manipulation.
Methods
Common seasonings used for cooking in our environment wereprocured from the open market in Jos, Nigeria. They included tablesalt, two different popular brands of seasoning cubes and one popularbrand of seasoning powder. Two popular traditional seasoningmaterials were also procured to compare with the commerciallyproduced ones. These were “kanwa” (lake salt) and “tooka”. Theformer is in solid form and is produced by boiling to evaporation,water from salt lakes or in some instances recovered as granules whiledigging under the soil in the same area(s). The latter is in powder formand is produced by cooking the chaff of a local cereal (millet) called“acha” after crushing and mixing with water. This is then sieved todiscard the sediments. The sieved fluid is then boiled to evaporationleaving a golden brown powder used as seasoning in cooking.
One gram of each material was measured and dissolved in 10 mlsof distilled de-ionised water and used as the working solution. Onehundred mls of each working solution was added to 9.9 mls of deioniseddistilled water in separate containers. One hundred mls of thestandard was treated the same way as the working solutions to bringthe standard concentration to 160mmol/l. Sodium and potassiumwere then determined for each working solution by flame photometryin the analytical laboratory of National Veterinary Research Institute,Vom near Jos by BND and GONE.
Results
The table salt expectedly had the highest sodium content andlowest potassium content. This was followed in sodium contentby the commercially prepared seasoning powder with potassiumcontent as low as for table salt. The two seasoning cubes were almostequal in sodium content, roughly seven times less than for table salt.Their potassium content was roughly six times greater than for tablesalt. For the traditional seasonings, the lake salt “kanwa” had sodiumin the same range as the commercially prepared seasoning cubes, buthad double their potassium content. For the traditional seasoningpowder “tooka”, the sodium was markedly less than the rest with veryhigh potassium levels. In order of sodium/potassium ratio, the tablesalt was highest and “tooka” the least. Table 1 shows the details of theresults.
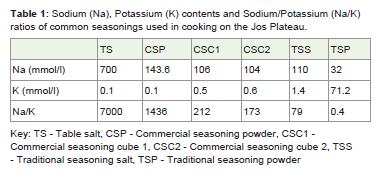
Table 1: Sodium (Na), Potassium (K) contents and Sodium/Potassium (Na/K)ratios of common seasonings used in cooking on the Jos Plateau.
Discussion
Almost in all instances hypertension treatment guidelinesrecommend non-pharmacological measures (life style modification)to control hypertension, a major one being salt restriction in diet[12]. Life style modification is known to work better if tailored tothe individual or group cultural heritage, beliefs and norms [13,14].Salt taste threshold is known to be higher in hypertensives and theiroff springs [15,16]. Taste attitude is a very high predictor of addedsalt in food [17] and determines what individuals or groups use infood as seasoning. The tendency is that individuals at greater risk forhypertension would crave more table salt in food, further fuelling arise in their blood pressures. The above notwithstanding, it is possibleto achieve significant salt reduction in the population; and Adeyemohas shown the feasibility in Nigeria [18].
This study has found that commercially produced seasoningsused in cooking in our environment though better than table saltin sodium and potassium profile could add significantly to thesodium intake if used in addition to table salt in cooking. This ishighest for the seasoning powder. The traditional seasoning salt(kanwa) though with sodium in the same range as the commerciallyprepared seasonings has about double to triple their potassiumcontent; and hence better regarding sodium/potassium profile thanthe commercially prepared seasonings. The best turned out to be thetraditional seasoning powder (tooka) which has very low sodiumand high potassium contents resulting in the least sodium/potassiumratio. This makes it ideal for seasoning in hypertensives and thoseprone to the disease. It is known that high sodium/potassium ratioscontribute to hypertension and several cardiovascular diseases [19].Use of such plant based seasonings with low sodium/potassium ratiocould partly explain the lower prevalence of hypertension in the ruralareas where they are used more commonly than the commerciallyprepared seasonings.
Potassium intake all over the world is lower than desired [20].In the west improved intake is by recommended intake in fruits andvegetables [21]. Unfortunately this is low there [22] as well as in ourenvironment for reasons ranging from cost, lack of storage facilitiesand group food habits. Seasonings used for cooking would seem tobe a convenient way of increasing potassium intake since most ofthe sodium intake is via table salt used in food. Use of traditionalseasonings like “tooka” in this case should be encouraged in ourenvironment and the commercially produced ones discouragedin addition to table salt used for cooking. Where flavor becomes agreat issue, non salt containing seasonings like onion, garlic, curry pepper and nutmeg or various traditional plant based seasoningscould suffice, to prevent high sodium intake in diet with consequenthypertension. Such individual and population intervention in foodhabits would go a long way in keeping hypertension statistics low andby extension its attendant complications; especially in blacks wherea modest reduction in sodium intake is associated with significantdecreases in blood pressure [23]. Smith-Sprangler et al. [24] haveshown how efforts in the population to decrease sodium intake resultin decreased cardiovascular disease burden. The same applies to strokeas Gardener et al have also found that low dietary reduces incidenceof stroke [25].
Until large scale co-operation by the food industry is achieved inthis regard (especially in appropriate sodium labeling of products),our roles as clinicians should hinge on education of the publicregarding dietary choices towards decreasing dietary sodium intake.
Acknowledgement
We are grateful to Matron Bingel, Nursing Services, Jos UniversityTeaching Hospital, Jos for giving details of preparation of “tooka”.
References
- Weinberger MH (2008) Are children doomed by what they eat and drink? Hypertension 51: 616-616.
- Messerli FH, Schmieder RE, Weir MR (1997) Salt a perpetrator of hypertensive target organ disease? Arch Intern Med 157: 2449-2452.
- Sanders PW (2008) Salt sensitivity. It is not always in the genes. Hypertension 51: 823-823.
- Ferdinand KC (2008) Hypertension in Blacks. In: JL Izzo, DA Sicca, HL Blacks (eds). The essentials of high blood pressure. Basic Science, Population Science and Clinical Management. 4th edition. Wolters Kluver/Lippincott Williams & Wilkins. Philadelphia. 279- 280.
- Whelton PK (2008) Potassium and blood pressure. Ibid 4: 304-306.
- Houston MC, Harper KJ (2008) Potassium, magnesium and calcium: their role in both the cause and treatment of hypertension. J Clin Hypertens 10: 3-11.
- Chirinos JA, Townsend R (2010) Sodium, Potassium and Target Organ Damage. A Case for Central Haemodynamics. Hypertens 56: 578-580.
- Appel LJ, Espeland MA, Easter L, Wilson AC, Folmar S, et al. (2001) Effects of reduced sodium intake on hypertension control in older individuals: results from the trial of non-pharmacological interventions in the elderly (TONE). Arch Intern Med 161: 685-693.
- Cappuccio FP, Plange-Rhule J, Philips RO, Eastwood JB (2000) Prevention of Hypertension and Stroke in Africa. Lancet 356: 677-678.
- 10.Gao SK, Fitzpatrick AL, Psaty B, Jiang R, Post W, et al. (2009) Sub-optimal nutritional intake for hypertension control in 4 ethnic groups. Arch Intern Med 169: 702-707.
- Bibbings-Domingo K, Chertow GM, Coxson PG, Moran A, Lightwood JM, et al. (2010) Projected effects of dietary salt reductions on future cardiovascular diseases. N Engl J Med 362: 590-599.
- Elliot WJ, Black WR (2005). Hypertension. In: ND Wong, JM Gardin (eds). Preventive Cardiology. A practical approach. McGraw Hill. New York, Chicago, San Francisco, Lisbon, London, Madrid, Mexico-City, Milan, New Delhi, San Juan, Singapore, Sydney, Toronto. 2nd edition. P 149- 182.
- Scisney-Matlock M, Busworth A, Giger JN, Strickland OL, Harrisson RV, et al. (2009) Strategies for implementing and sustaining therapeutic life style changes as part of hypertension management in African Americans. Postgrad Med 121: 147-159.
- Lee J (2008) An ethnic sensitive approach for the promotion of a healthy life style. Is it warranted? J Hum Hypertens 22: 587-589.
- Olayemi SO, Mabadeje AF (2003) Comparative study of salt threshold of hypertensives, their normotensive relatives and non-relatives. Niger Postgrad Med J 10: 96-98.
- Ukoh VA, Ukoh GC, Okosun RE, Azubike E (2004) Salt intake in first degree relations of hypertensive and normotensive Nigerians. East Afr Med J 81: 524- 528.
- Van der Veen JE, DeGraaf C, Van Dis SJ, Van Staveren WA (1999) Determinants of salt used in cooked meals in the Netherlands: attitudes and practices of food preparers. Eur J Clin Nutr 53: 388-394.
- Adeyemo AA, Prewitt TE, Luke A, Omotade OO, Rotimi CN, et al. (2002) The feasibility of implementing a dietary sodium reduction intervention among free living normotensive individuals in South West Nigeria. Ethn Dis 12: 207-212.
- Eaton SB, Eaton SB 3rd, Kronner MJ (1997) Paleolithic nutrition revisited. A twelve year retrospective on its nature and implications. Eur J Clin Nutr 51: 207- 216.
- Van Mierlo LAJ, Greyling AG, Zock PL, Kok FJ, Geleijnse JM (2010) Sub-optimal potassium intake and potential impact on population blood pressure. Arch Intern Med 170: 1501-1502.
- Kotchen TA, Kotchen JM (2008) Life style modification. Ibid 4: 406-409.
- Kris-Etherton PM, Hilpert KF, Krauss RM (2000) Nutrition. Ibid 9: 256-295.
- He FJ, Maciniak M, Visagie E Markandu ND, Anand V, et al. (2009) Effect of modest salt reduction on blood pressure, urinary albumin and pulse wave velocity in white, black and Asian mild hypertensives. Hypertension 54: 482-488.
- Smith-Spangler CM, Juusola JL, Euns EA, Owens DK, Garber AM (2010) Population strategies to decrease sodium intake and the burden of cardiovascular disease: a cost effectiveness analysis. Ann Intern Med 152: 481-487.
- Gardener H, Rundek T, Wright CB, Elkind MSV, Sacco RL (2012) Dietary sodium and risk of stroke in the Northern Manhattan Study. Stroke 43: 1200-1205.