Research Article
Relationship between Calcium or Vitamin C Supplement Use and Blood Pressure in Japanese Elderly People: Results from the National Health and Nutrition Survey, 2003-2010
Yoko Sato*, Tsuyoshi Chiba, and Keizo Umegaki
Information Center, National Institute of Health and Nutrition, National Institutes of Biomedical Innovation, Health andNutrition, Japan
Corresponding author: Yoko Sato, Information Center, National Institute of Health and Nutrition, National Institutes ofBiomedical Innovation, Health and Nutrition, 1-23-1 Toyama, Shinjuku-ku, Tokyo 162-8636, Japan, Tel: +81-3-3203-5721;Fax: +81-3-3202-3278; E-mail: satoyoko@nih.go.jp
Citation: Sato Y, Chiba T, Umegaki K. Relationship between Calcium or Vitamin C Supplement use and Blood Pressure in Japanese Elderly People: Results from the National Health and Nutrition Survey, 2003-2010. Indian J Nutri. 2015;2(1): 112.
Copyright © 2015 Yoko Sato, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 2, Issue: 2
Submission: 14/09/2015; Accepted: 30/09/2015; Published: 06/10/2015
Abstract
A higher intake of calcium or vitamin C has been associated with reductions in blood pressure (BP). However, the relationship between calcium or vitamin C supplement use and BP has not yet been confirmed. We herein investigated this relationship in elderly Japanese people. Data from the National Health and Nutrition Survey in Japan, 2003-2010 were used. Systolic/Diastolic BP (SBP/DBP) was compared by the usage of calcium or vitamin C supplements separately for antihypertensive medication use. Linear regression models were adjusted for sex, age, antiarrhythmic medication, drinking habits, smoking status, exercise habits, body mass index (BMI), sodium intake, and potassium intake. A total of 17067 people aged 60 years or older were included, among whom 40.4% took antihypertensive medication. Calcium or vitamin C supplement use did not correlate with SBP/DBP. On the other hand, non-drinkers and those with a lower BMI had a lower BP. These results indicated that the intake of calcium or vitamin C supplements was not involved in the regulation of BP. The results of the present study suggest that improving dietary habits is more effective as a public health measure than using dietary supplements.
Keywords: Blood pressure; Calcium/vitamin C supplements; Elderly people; National Health and Nutrition Survey in Japan
Introduction
Blood pressure (BP) control is an important public health issuebecause hypertension is one of the risk factors for cardiovasculardisease [1-3]. Japan is the most rapidly aging country in theworld, and the marked increase in medical expenses has become asignificant problem. A report by the Estimates of National MedicalCare Expenditure 2012 in Japan showed that hypertensive treatmentsaccounted for approximately 5% of medical expenses, and mostpatients with hypertension were elderly [4].
The intake of food with health-promoting effects is increasinglybeing used as a countermeasure against hypertension, and concertedefforts have been made to reduce medical costs through theutilization of various forms of dietary supplements such as tablets,capsules, and powders. Dietary supplements contain not onlyvitamins and minerals, but also herbs, botanicals, enzymes, andanimal extracts. Dietary supplement use is prevalent, with elderlypeople using supplements to prevent various diseases [5]. However,evidence in support of the efficacy and safety of non-vitamin/mineralsupplements enriched with specific components such as natural substances is limited, and, as such, further studies are warranted. Onthe other hand, vitamins and minerals are essential nutrients thatour body needs in small amounts to work properly, and evidenceof their safety is well established. Therefore, if people take dietarysupplements, vitamin/mineral supplements would be safer thannatural products.
Calcium or vitamin C are known to play a role in the regulationof BP; an inverse relationship was previously reported between thedietary intake of or supplementation with calcium and/or vitaminC and BP in cross-sectional studies [6-8], randomized controlledtrials [9,10] and meta-analyses[11-13]. Calcium and vitamin Csupplements are popular with elderly Japanese people because of theirbone health-promoting and antioxidant effects. If these supplementsactually contribute to reductions in BP, they may help reduce medicalcare expenditure. Therefore, it is considered important to determinewhether calcium and vitamin C supplements are effective tools for theprevention of hypertension. Previous studies on calcium or vitaminC dietary and supplemental intake by the Japanese population havebeen limited in their comprehensiveness because they were onlyregional [7,10]. Furthermore, to the best of our knowledge, a nationalsurvey report has not yet been conducted on the association withcalcium or vitamin C supplement use and BP.
In the present study, we examined the relationship between theuse of calcium or vitamin C supplements and BP among elderlypeople based on data from the National Health and Nutrition Survey(NHNS) in Japan 2003-2010.
Methods
Study population
The present study used NHNS data between 2003 and 2010 withpermission from the Ministry of Health, Labour and Welfare, Japan.The NHNS is conducted every November as a cross-sectional surveyof a nationally representative sample of the non-institutionalizedJapanese population; it includes a physical examination, dietarysurvey, and questionnaires on health-related behaviors [14]. Detailsof the NHNS study protocol, data collection design, and otherdocumentation are available online (in Japanese) [14-21]. The qualityassurance of data processing has been described elsewhere [22]. Thesample included 26670 elderly people aged 60 years or older. Weexcluded participants whose data on dietary supplement use, BP, andantihypertensive medication were unreported. The final sample sizefor analyses was 17067 elderly people.
Sociodemographic and Health Status
In the NHNS, sociodemographic and health status data wereobtained by questionnaires. Sociodemographic items included sex(men/women) and age. Health status included current medication(antihypertensive and antiarrhythmic drugs; yes/no), BP, drinkingstatus (current/past, never), smoking habit (current/past, never), andexercise habit (yes/no).
Nutrient and Supplement Intakes
A semi-weighed, 1-day household dietary record withapproximate proportions by which family members shared each dish was used [22]. Nutrient intake for each family member was estimatedbased on the Standard Tables of Food Composition in Japan, FifthRevised (NHNS 2003-2004), and Fifth Revised and Enlarged Edition(NHNS 2005-2010) [23]. We used calcium (mg/day), vitamin C(mg/day), sodium (mg/day) , and potassium (mg/day) intake data.Calcium and vitamin C intakes from food were calculated as all intake(mg) - intake from dietary supplements (mg).
The intake of dietary supplements containing calcium orvitamin C was also collected using the 1-day dietary record in theNHNS. There is no clear definition of dietary supplements in Japan.Therefore, in the present study, dietary supplements were defined as“supplements, including drugs or quasi-drugs, intended for ingestionin pill, capsule, tablet, powder, or liquid form”, as per the NHNSdefinition [14-21].
Blood pressure
In the NHNS, Systolic/Diastolic BP (SBP/DBP) weremeasured by health care providers using the Riva-Rocci mercurialsphygmomanometer and Japanese Industrial Standards manchette(BP cuff) instrument. Two measurements were taken and the secondmeasurement was used.
Statistical analysis
All analyses were performed separately for antihypertensivemedication use. The sociodemographic status, health status, andnutrition intake (calcium, vitamin C, sodium, and potassium) werecompared between supplement users and non-users of calcium orvitamin C supplements. The χ2 and one-way ANOVA tests wereperformed for categorical and continuous variables, respectively.
The adjusted mean values of BP by dietary supplement usewere calculated by ANCOVA. Mean BP values were unadjusted(Unadjusted) and adjusted for sex and age (Adjusted 1); for sex, age,antiarrhythmic drugs, drinking status, smoking habit, exercise habits,BMI, sodium intake, and potassium intake (Adjusted 2).
Multivariable regression models were used to assess therelationship between calcium or vitamin C supplement use and BP.The confounding variables included were the same as Adjusted 2.
All statistical analyses were performed using PASW statistics forWindows (version 18.0J, 2009; SPSS Inc., Chicago, IL, USA), and thelevel of significance was set at p < 0.05.
Results
Characteristics associated with calcium supplement use
Antihypertensive medication users accounted for 40.4% (n=6898)of the elderly population examined. Among antihypertensivemedication non-users, the utilization ratio of calcium supplementswas 3.4% (n=350), and their mean calcium intake from foods was671.5 (SD=283.5) mg/day. Among antihypertensive medication users,2.9% (n=198) elder people used calcium supplements, and their meancalcium intake from foods was 684.9 (SD=291.1) mg/day. Regardlessof the antihypertensive medication use, calcium supplement userswere more likely to be female, not taking antiarrhythmic medication,not smoking, than non-users. Calcium supplement users were alsomore likely to have a higher potassium intake and calcium intakefrom food, than non-users (Table 1).
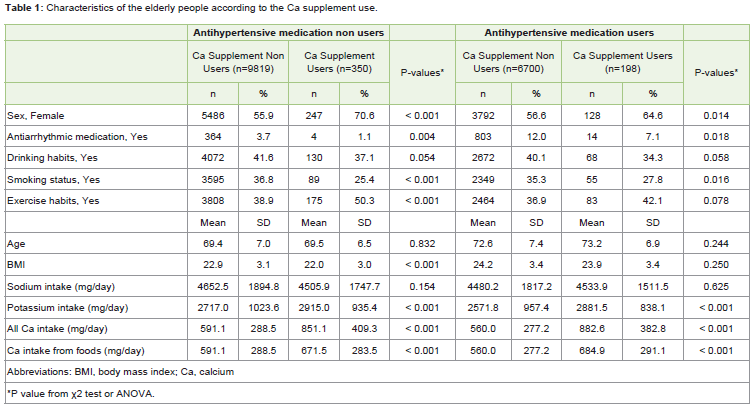
Table 1: Characteristics of the elderly people according to the Ca supplement use.
BP and calcium
No significant differences were observed in SBP betweencalcium supplement users and non-users in Adjusted 2, whereascalcium supplement users had a lower SBP than that of non-usersin Unadjusted and Adjusted 1, among antihypertensive medicationnon-users (Table 2). A multivariate analysis showed that calciumsupplement use was not associated with SBP (Table 3).
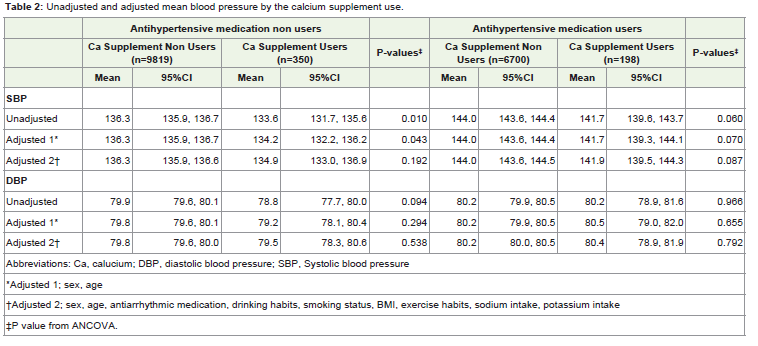
Table 2: Unadjusted and adjusted mean blood pressure by the calcium supplement use.
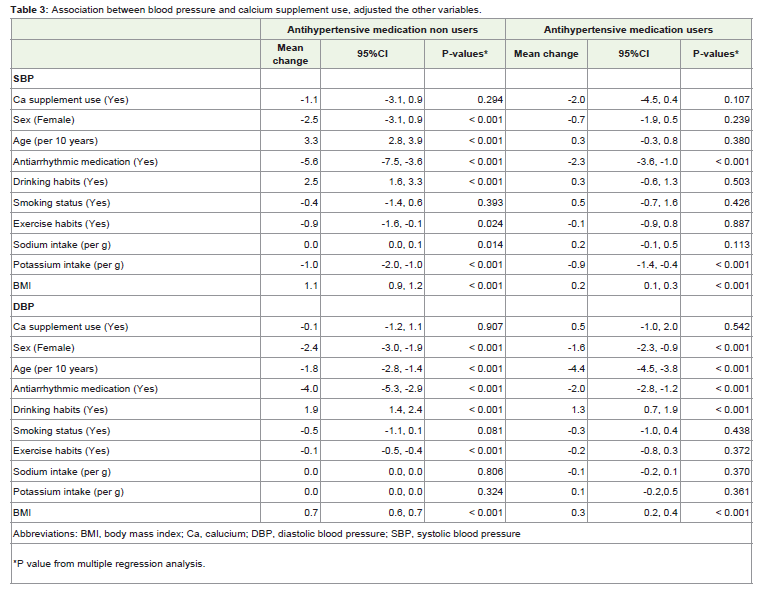
Table 3: Association between blood pressure and calcium supplement use, adjusted the other variables.
DBP was not significant associated with calcium supplement usein all analyses (Table 2,3).
Characteristics associated with vitamin C supplement use
The utilization ratio of vitamin C supplements was 4.8% (n=493),and their mean vitamin C intake from foods was 171.6 (SD=129.4)mg/day among antihypertensive medication non-users. Theircharacteristics were more likely to be female, not smoking, and havemore exercise habits, a lower BMI, intake of sodium, and a higherintake of potassium and vitamin C from food, than non-users. Amongantihypertensive medication users, 4.0% (n=275) elder people usedvitamin C supplements, and their mean vitamin C intake from foodswas 153.9 (SD=179.1) mg/day. Their characteristics were more likelyto have more exercise habits, and a higher potassium intake thannon-users (Table 4).
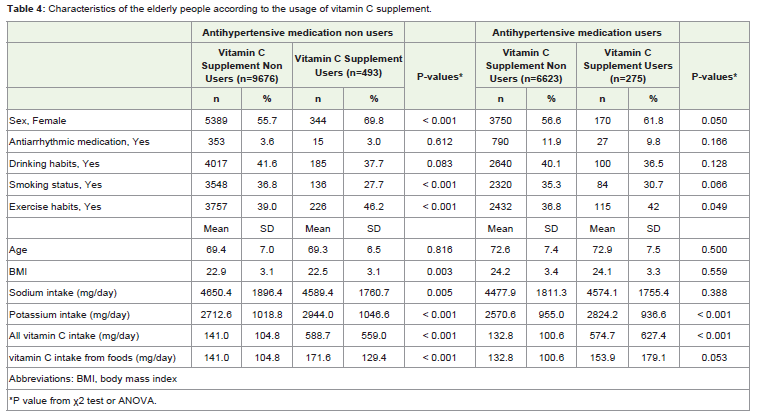
Table 4: Characteristics of the elderly people according to the usage of vitamin C supplement.
BP and vitamin C
No significant differences were observed in adjusted mean SBPbetween vitamin C supplement users and non-users; however,vitamin C supplement users had a lower SBP than non-users inUnadjusted only, among antihypertensive medication non-users(Table 5). Among antihypertensive medication users, there were nosignificant differences in SBP between vitamin C supplement users and non-users in Adjusted 2, whereas vitamin C supplement usershad a lower SBP than that of non-users in Unadjusted and Adjusted 1(Table 5). A multivariate analysis showed that vitamin C supplementuse was not associated with SBP (Table 6).
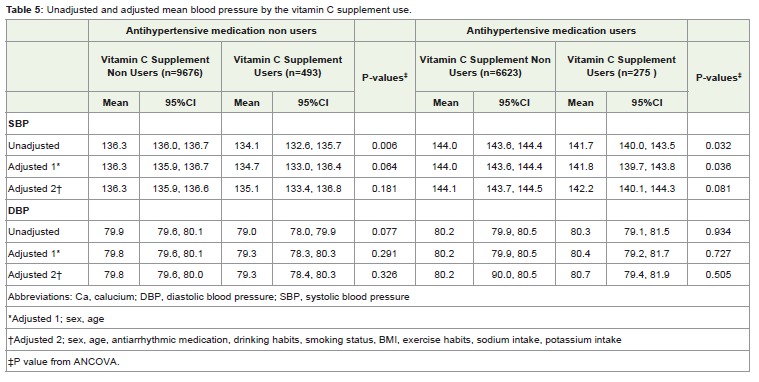
Table 5: Unadjusted and adjusted mean blood pressure by the vitamin C supplement use.
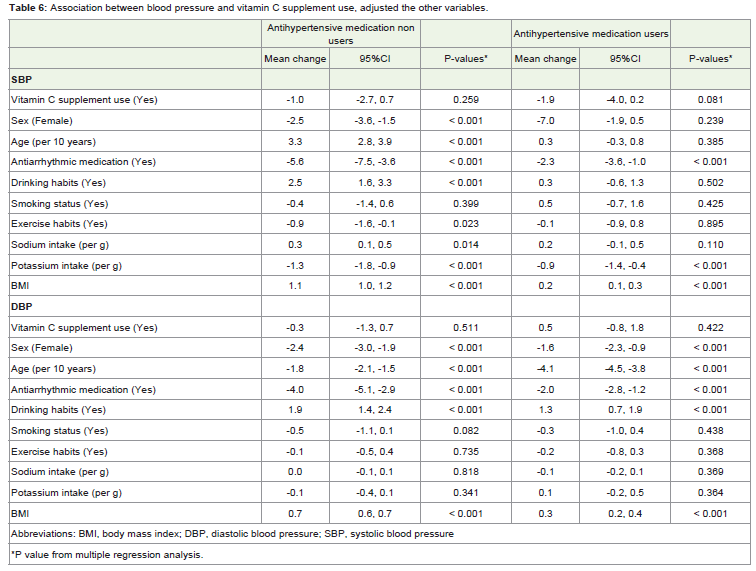
Table 6: Association between blood pressure and vitamin C supplement use, adjusted the other variables.
DBP was not significant associated with vitamin C supplementuse in all analyses (Table 5,6).
Discussion
This cross-sectional study of a representative sample of theJapanese population revealed that the use of calcium or vitamin Csupplements was not associated with BP reductions among elderlypeople.
Japan is an aging society, and the marked increase in medicalexpenses has become a big problem [4]. Concerted efforts have beenmade to reduce medical costs through the utilization of food withphysiological functions. The prevention of hypertension representsa particularly important measure because many elderly people aretreated for hypertension [24]. Accumulated evidence has indicatedthat vitamins and minerals are safer than natural products for useas dietary supplements. Therefore, we herein determined whethercalcium and vitamin C supplements, which were previously reportedto have an inverse relationship with high BP [6-13] were an effectivetool for the prevention of hypertension.
In the elderly people who take antihypertensive medication, theblood pressure is controlled with those medicines and hard to beaffected by the food. Therefore, we analyzed the data separately forantihypertensive medication use. Regardless of the antihypertensivemedication use, our results showed that calcium or vitamin Csupplement use was not associated with BP. Although, some previous study suggested that calcium or vitamin C supplements reducedBP [9-13]. The reasons for this difference currently remain unclear.Calcium or vitamin C supplement users had a lower systolic BPthan that of the non-users in the unadjusted analysis. Therefore, weconsidered the apparent effects of dietary supplements to disappearby adjustments for various factors influencing BP or that the BPreducingeffects of calcium/vitamin C supplements were very few [11,12]. Excessive amounts of vitamin C are immediately flushed outof our body through urination [25-27], suggesting that the influenceof supplements was not significant because participants had asufficient nutrient intake from food. Hence, reductions in BP may notoccur with the intake of calcium or vitamin C supplements, especiallyin those with an adequate nutritional status. Another reason is thatthis difference may be due to small group size for analysis of calcium or vitamin C supplement users.
In antihypertensive medication non-users, non-drinkers, thosewith a lower BMI, with exercise habits, with lower sodium intake, andhigher potassium intake had a lower SBP. Even in antihypertensivemedication users, a lower BMI and a higher potassium intakewere associated with a lower SBP. Furthermore, non-drinkers andthose with a lower BMI had a lower DBP among all groups. Theseresults suggested that improving dietary habits is more effective forcontrolling BP than the use of dietary supplements.
Previous studies have suggested that calcium supplement use withhigh dietary calcium intake increases the risk of cardiovascular disease[28-31]. The present study did not show that calcium supplementusers had a higher BP than that of non-users. However, the intakeof calcium from food was higher by calcium supplement users thanby non-users, with a mean amount of 851 or 883 mg/day. Theseresults suggested that elderly people use supplements without neededthem, and also that supplement usage may lead to excessive mineralconsumption, resulting in adverse effects. Many elderly peoplemake efforts to increase their intake of calcium from their diets inan attempt to prevent osteoporosis; therefore, supplemental calcium may have detrimental effects in these individuals [28-32]. In the caseof vitamin C, supplement users took about 420 mg/day of vitamin Cfrom supplements, whereas the recommended dietary allowance is100 mg/day in Japan [23]. Guidance regarding appropriate intake anddecisions for dietary supplement use is necessary.
Elderly people are more likely to use dietary supplements [5,33].A previous study reported that 46% of elderly Japanese people useddietary supplements [34]. However, calcium or vitamin C supplementusers accounted for less than 5% of our study population. The reasonfor this may have been that many elderly people used supplementswith natural substances rather than vitamins and minerals [34]. Sincedietary supplements are not drugs, manufacturers cannot claim thatthe supplements treat or cure diseases in Japan; however, some peopleuse them to treat their disease due to the flood of advertisementsimplying that supplements are effective for various diseases suchas hypertension, diabetes, arthritis, and cancer [35]. Most elderlypeople visit a hospital to be treated, therefore they are likely to betaken in by such advertisements. Calcium and vitamin C are essentialnutrients, and their beneficial effects are well-known. However, theireffectiveness for other diseases is controversial as are effects of natural products. Since this is not quoted by the mass media, sufficientinformation may not be available to elderly people. Therefore, theinformation system for elderly people who do not use social networkservices needs to be improved.
The present study had several limitations. First, the NHNS wasa cross-sectional survey and did not allow for the determination ofcausal effects. Second, as the NHNS was a 1-day survey, the intakeresults of dietary supplements and food may not reflect habitual intakeby the individual. There is a doubt that intra-individual variation ofdietary supplement users may be larger than that of nonusers, becausedietary supplements contain large amounts of specific nutrients.Although, it was reported that almost Japanese dietary supplementusers were daily users [36]. Therefore, we thought the methodologicallimitation of a 1-day survey is unlikely to have largely skewed theresults. Furthermore, seasonal variations may also have influencedthe results obtained. Nutrient intakes were not exact, but estimatedby calculations. Additionally, the brand names of specific dietarysupplements were not reported. Thus, the results of the present studyneed to be interpreted with these limitations in mind.
In conclusion, the present study showed that calcium orvitamin C supplement use did not correlate with SBP/DBP in elderlyJapanese people. Additionally, calcium or vitamin C supplementusers had a higher intake of calcium or vitamin C from food thanthat of non-users. The use of calcium or vitamin C supplements isnot recommended for the prevention and treatment of hypertensionin Japan. Continuous recommendation to improve dietary habitsis considered more effective as a public health measure than usingdietary supplements.
Acknowledgments
This work was supported by a Health and Labour Sciences Research Grants (Research on Food Safety) from the Ministry of Health, Labour and Welfare, Japan.
References
- He J, Whelton PK (1999) Elevated systolic blood pressure as a risk factor for cardiovascular and renal disease. J Hypertens Suppl 17: S7-13.
- Lawes CM, Bennett DA, Lewington S, Rodgers A (2002) Blood pressure and coronary heart disease: A review of the evidence. Semin Vasc Med 2: 355-368.
- Lawes CM, Bennett DA, Feigin VL, Rodgers A (2004) Blood pressure and stroke: an overview of published reviews. Stroke 35: 1024-1033.
- Ministry of Health, Labour and Welfare. Estimates of National Medical calciumre Expenditure 2012.
- Dickinson A, MacKay D (2014) Health habits and other characteristics of dietary supplement users: A review. In Nutr J 13: 14.
- McCarron DA, Morris CD, Henry HJ, Stanton JL (1984) Blood pressure and nutrient intake in the united states. Science 224: 1392-1398.
- Iso H, Terao A, Kitamura A, Sato S, Naito Y, et al. (1991) Calcium intake and blood pressure in seven japanese populations. Am J Epidemiol 133: 776-783.
- da Silva Ferreira T, Torres MR, Sanjuliani AF (2013) Dietary calcium intake is associated with adiposity, metabolic profile, inflammatory state and blood pressure, but not with erythrocyte intracellular calcium and endothelial function in healthy pre-menopausal women. Br J Nutr 110: 1079-1088.
- Duffy SJ, Gokce N, Holbrook M, Huang A, Frei B, et al. (1999) Treatment of hypertension with ascorbic acid. Lancet 354: 2048-2049.
- Sato K, Dohi Y, Kojima M, Miyagawa K, Takase H(2006) Effects of ascorbic acid on ambulatory blood pressure in elderly patients with refractory hypertension. Arzneimittelforschung 56: 535-540.
- Bucher HC, Cook RJ, Guyatt GH, Lang JD, Cook DJ, et al. (1996) Effects of dietary calcium supplementation on blood pressure. A meta-analysis of randomized controlled trials. JAMA 275: 1016-1022.
- Allender PS, Cutler JA, Follmann D, Cappuccio FP, Pryer J, et al. (1996) Dietary calcium and blood pressure: A meta-analysis of randomized clinical trials. Ann Intern Med 124: 825-831.
- Juraschek SP, Guallar E, Appel LJ, Miller ER, 3rd (2012) Effects of vitamin c supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am J Clin Nutr 95: 1079-1088.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2010.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2003.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2004.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2005.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2006.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2007.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2008.
- Ministry of Health, Labour and Welfare. Annual Report of the National Health and Nutrition Survey in 2009.
- Iwaoka F, Yoshiike N, Date C, Shimada T, Tanaka H (2001) A validation study on a method to estimate nutrient intake by family members through a household-based food-weighing survey. J Nutr Sci Vitaminol 47: 222-227.
- Ministry of Health, Labour and Welfare. Dietary Reference Intakes for Japanese, 2010.
- Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions 2013.
- Levine M, Conry-Cantilena C, Wang Y, Welch RW, Washko PW, et al. (1996) Vitamin c pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proc Natl Acad Sci U S A 93: 3704-3709.
- Levine M, Wang Y, Padayatty SJ, Morrow J (2001) A new recommended dietary allowance of vitamin C for healthy young women. Proc Natl Acad Sci U S A 98: 9842-9846.
- Blanchard J, Tozer TN, Rowland M (1997) Pharmacokinetic perspectives on megadoses of ascorbic acid. Am J Clin Nutr 66: 1165-1171.
- Bolland MJ, Avenell A, Baron JA, Grey A, MacLennan GS, et al. (2010) Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 341: c3691.
- Michaelsson K, Melhus H, Warensjo Lemming E, Wolk A, et al. (2013) Long term calcium intake and rates of all cause and cardiovascular mortality: community based prospective longitudinal cohort study. BMJ 346: f228.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, et al. (2013) Dietary and supplemental calcium intake and cardiovascular disease mortality: the national institutes of health-aarp diet and health study. JAMA Intern Med 173: 639-646.
- Li K, Kaaks R, Linseisen J, Rohrmann S (2012) Associations of dietary calcium intake and calcium supplementation with myocardial infarction and stroke risk and overall cardiovascular mortality in the heidelberg cohort of the european prospective investigation into cancer and nutrition study (epic-heidelberg). Heart 98: 920-925.
- Ohtake T, Kobayashi S, Negishi K, Moriya H (2005) Supplement nephropathy due to long-term, high-dose ingestion of ascorbic acid, calcium lactate, vitamin d and laxatives. Clin Nephrol 64: 236-240.
- Tsubota-Utsugi M, Nakade M, Imai E, Tsuboyama-Kasaoka N, Nozue M, et al. (2013) Distribution of vitamin E intake among japanese dietary supplement and fortified food users: A secondary analysis from the national health and nutrition survey, 2003-2009. J Nutr Sci Vitaminol 59: 576-583.
- Hirayama F, Lee AH, Binns CW, Watanabe F, Ogawa T (2008) Dietary supplementation by older adults in japan. Asia Pac J Clin Nutr 17: 280-284.
- Chiba T, Sato Y, Nakanishi T, Yokotani K, Suzuki S, et al. (2014) Inappropriate usage of dietary supplements in patients by miscommunication with physicians in japan. Nutrients 6: 5392-5404.
- Anraku M, Inoue H, Sato E, Hata T, Tsuchiya D, et al.(2010) Surveillance study in collaboration with a university-daycare center for elderly people and nursery school for children on the use of over-the-counter drugs and health food in fukuyama. Yakugaku Zasshi 130: 1093-1103.