Research Article
Health Status of School Going Girls
Abha Khetarpal *
Corresponding author: Dr. Abha Khetarpal, Associate Professor, DAV College, Yamunanagar-135001(Haryana), India; E-mail: abhakhetarpal@rediffmail.com
Citation: Khetarpal A. Health Status of School Going Girls. Indian J Nutri. 2015;2(1): 109.
Copyright © 2015 Abha Khetarpal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | Volume: 2, Issue: 1
Article Information: Submission: 03/06/2015; Accepted: 20/07/2015; Published: 30/07/2015
Abstract
The diet for a child should be focused on natural, fresh sources of energy and nutrients. Drastic dieting must be avoided. A positive attitude to healthyeating should be encouraged from an early stage. A nutritious diet and daily practice of yoga can raise the health status of school going girls. Sixty girls of agegroup 7-9 Years belonging to low Socio economic group in Yamunanagar district of State Haryana were divided equally into control (C) and experimental (E)group .The experimental group comprised of 30 girls and they along with their mothers were imparted nutrition counseling which included dietary counselingand teaching yoga twice a month for a period of four months Assessment of nutritional status was done before and after imparting nutrition counseling. Themean height of subjects in C and E group was 116.1cm and 117.1 cm in the beginning of the study and 116.2cm and 117.9 cm at the end. The averageweight of subjects in both the groups was 20.1 kg in the beginning which significantly increased to 21.7 kg in E group after nutrition counseling . However, allthe indices were lower than the standard parameters. Thus it can be inferred that nutrition counseling should be imparted for a longer duration and should beincluded in school curriculum.
Keywords: Nutrition counseling; Nutritional status; Height, Weight
Introduction
In India, weight for age has been the most widely used indicatorfor assessment of nutritional status, detection of under nutrition andmonitoring the improvement following interventions in children.The question whether in Indian children with high stunting rates dueto past chronic under nutrition, BMI for age is a more appropriateindicator for assessment of current under nutrition and improvementfollowing interventions is often debated among nutrition scientistsin the country. While there is global acceptance that body massindex (BMI) should be used for assessment of obesity/adiposity inchildren19, there has not been a similar consensus regarding use ofBMI for assessment of under nutrition in children. Indian infantsbegin life with a disadvantage due to poor intrauterine growth; atbirth one third of Indian infants are under weight and wasted and20% are stunted. Maternal factors associated with low birth weight(LBW) such as low maternal height and low pre-pregnancy weightcannot be modified during pregnancy. To develop to their optimalpotential, it is vital that children are provided with nutritionally sounddiets. Diet and exercise patterns during childhood and adolescencemay spell the difference between health and risk of disease in later years. Different stages of the life cycle dictate differing nutrient needs.Dietary habits, which affect food preferences, energy consumptionand nutrient intakes, are generally developed in early childhood. Oneof the most frequently missed meal is breakfast. Studies show thatbreakfast plays an important role in providing needed energy andnutrients after an overnight fast and can aid in concentration andperformance at school. Snacks generally form an integral part of mealpatterns for both children and teenagers. Younger children cannoteat large quantities at one sitting and often get hungry long beforethe next regular mealtime. Mid-morning and mid-afternoon snackscan help to meet energy needs throughout the day. Fast-growing andactive children often have substantial energy and nutrition needs andthe teaching of food and nutrition in the school curricula will enablechildren to have the knowledge to make informed choices about thefoods in their regular meals and snacks.
Nutrition plays a vital role as inadequate nutrition duringchildhood may lead to malnutrition, growth retardation, reducedwork capacity and poor mental and social development [1]. Nutrition education also needs to be included in school curriculum as children are better able to retain nutrition knowledge gained at school level, when it is reinforced by favorable conditions in the home [2]. Keeping this in view, the present study was conducted to see theimpact of nutrition counseling on the health status of school goinggirls. Normally, the energy requirements of children tend to parallelwith their growth rate, and individuals meet their energy needs bymeans of their appetite with adequate precision. As a result, majorityof them maintain energy balance, and a varied food intake providessufficient nutrients to ensure optimal growth and development. Stressand emotional upsets however can seriously affect the energy balancein children, resulting in the consumption of too little or too muchfood. Mild or severe infections, nervousness, dental or skin problems(acne) can result in alterations of appetite and those on marginaldiets are the most vulnerable. Emotional stress is often associatedwith food faddism and slimming trends, both of which can lead toeating disorders such as anorexia nervosa. On the other hand, theprevalence of overweight and obesity in children and adolescents isnow a major nutritional problem and the condition is likely to persistinto adulthood. Developing children are particularly concerned abouttheir body image and excessive weight can have profound effects ontheir emotional well being as well as on their physical health. The causeof obesity is multifactorial and socio-economic, biochemical, genetic,and psychological factors all closely interact. Lack of activity plays animportant role in the development, progression and perpetuation ofobesity during childhood.
Surveys of young people have found that the majority islargely inactive and health professionals and governments arenow encouraging higher levels of physical activity among childrenand adolescents. Physical inactivity does not only have a primerole in the development of overweight and obesity, but also onthe development of chronic diseases such as heart disease, certaincancers, diabetes, hypertension, bowel problems and osteoporosis inlater life. In addition, physical activity is related to improvements inbody flexibility, balance, agility and co-ordination and strengtheningof bones. The current recommendation is for children to try to bephysically active for at least 60 minutes daily.
Materials and Methods
For the study sixty girls of 7-9 years belongings to low socioeconomic group were selected randomly from two GovernmentSchools of Yamunanagar district. They were divided into Experimental (E) and control (C) Group Comprising of 30 girls each. Girls in Experimental Group along with their mothers were imparted nutrition counseling twice a month for a period of four months through lecture cum - discussion method with the use ofcharts, posters and demonstrations. Interview-cum-questionnairemethod was used for collecting background information of thesubjects. Anthropometric measurements like height, weight,Mid upper Arm Circumference (MUAC) and Triceps Skin FoldThickness (TSFT) of the school girls were recorded before and afternutrition counseling using the techniques given by Jelliffe [3]. Datawas analyzed statistically. Mean and standard error were calculatedfor each variable. Comparison of anthropometric parameters ofsubjects in E and C group was done. Monitoring of growth by serialmeasurements of anthropometric parameters particularly height andweight are routinely used to assess the nutritional status of a child. At the community level, it is used to identify children who mightbenefit from a nutrition or medical intervention. These assessmentsare usually made using the NCHS data as a reference standard upto10 years of age. There is however no agreement on the parameters tobe used for the assessment of growth and development in adolescenceas there exists a wide variation amongst different populations in timeof onset of puberty. These anthropometric parameters are thereforecompared with a cross-sectional study conducted by the ICMR in theseventies as well as with the growth of affluent children of India andthe NCHS standard.
Results and Discussion
The anthropometric parameters of school girls is presented inTable 1.
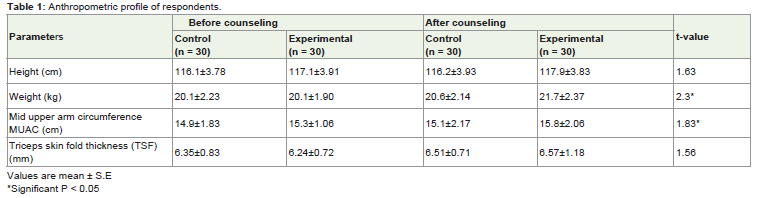
Table 1: Chemical composition of Dahi Samples.
Height
The mean height of the respondents in C and E Group beforecounseling was 116.1cm and 117.1 cm and after nutrition educationit increased to 116.2 cm and 117.9 cm respectively. The difference inaverage height of the subjects in E group before and after NutritionCounseling (NC) was statistically non -significant. It is evident fromTable 2 that the height of the respondents was 92.64% of NCHSstandards in E Group before counseling that increased to 93.27% aftercounseling for 4 months. These findings were supported by Sanghaet al. [4] who reported that mean height was 90 percent of NCHSstandards in primary school children in Ludhiana.
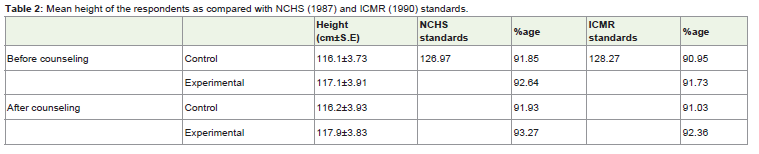
Table 2: Mean height of the respondents as compared with NCHS (1987) and ICMR (1990) standards.
Table 3 indicates that before counseling 16.7% girls were innormal category in E group, which increased to 20% after nutritioncounseling while there was no change in C group. Also an increasein percentage of respondents having mild malnutrition was observedin E group after Counseling. However percentage of respondentsdecreased in moderate and severe malnutrition category in E groupafter Nutrition education. The impact of Nutrition education wasevident as more respondents in E group shifted to normal and mildmalnourished category with none of the respondents in severelymalnourished category. Dutta and Kumar [5] also reported similarfindings that in Uttar Pradesh, 20% primary school children werenormal and remaining were suffering from different grades ofmalnutrition.
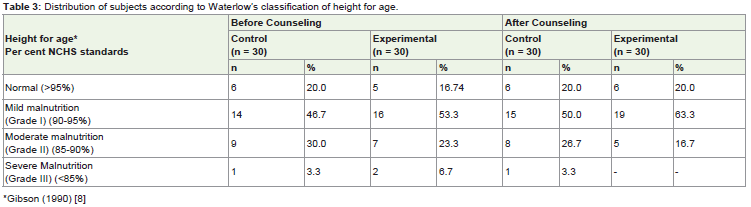
Table 3: Distribution of subjects according to Waterlow’s classification of height for age.
Weight
Table 4 shows that before imparting nutrition education themean weight of the respondents in C and E group was same i.e. 20.1kg and after counseling the weight of the girls in E group significantly(P< 0.05) increased to 21.7 kg while in C group no significant changewas observed. Both the groups were having less weight as comparedto NCHS and ICMR standards. Weight of respondents in E groupwas 80.3% of NCHS standards before counseling which increased to86.7% after imparting nutrition education.
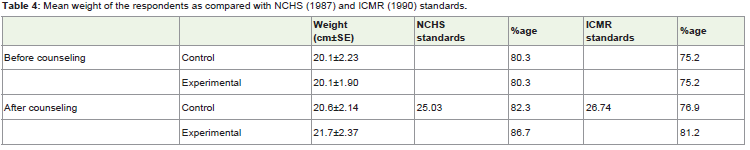
Table 4: Mean weight of the respondents as compared with NCHS (1987) and ICMR (1990) standards.
Table 5 shows the distribution of respondents according toGomez Classification of weight for age. Before counseling, 16.7%and 23.3% school girls in C and E group, respectively were in normalcategory which significantly increased to 33.3 percent in E group aftercounseling, while no significant change was observed in C group.After imparting nutrition education, the percentage of respondents in mild malnutrition category increased whereas and in moderatemalnutrition category decreased. Similar to present findings 25% girlsof Kumaon hill were normal [1] rest were suffering from differentgrades of malnutrition.
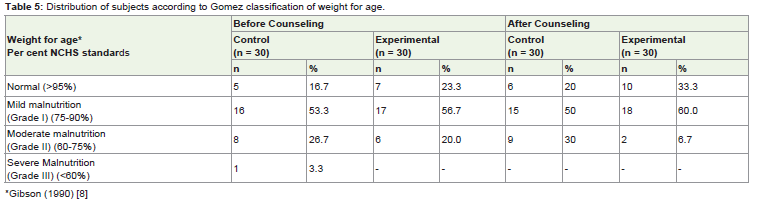
Table 5: Distribution of subjects according to Gomez classification of weight for age.
Mid Upper Arm Circumference (MUAC)
Table 6 shows that the mean MUAC of school girls in C andE group was 14.9 cm and 15.3 cm before counseling and thecorresponding values were 15.1 cm and 15.8 cm after impartingnutrition education which were less than the [3] standards of18.43 cm. A significant (p< 0.05) increase to 85.72% was noted aftercounseling. Similar findings were reported by Parvathi and Poorani[6], Awasthi and Kumar [1].
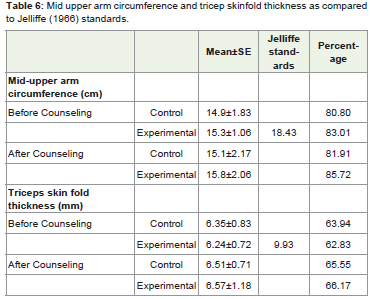
Table 6: Mid upper arm circumference and tricep skinfold thickness as comparedto Jelliffe (1966) standards.
Triceps Skin Fold Thickness (TSFT)
The mean TSFT in C and E group was 6.35 mm and 6.24 mmbefore counseling and 6.51 mm and 6.57 mm after counseling,indicating no significant change in E group. It is evident from Table6 that the TSFT was 62.83 and 66.17% of Jelliffe standards in E groupbefore and after imparting nutrition education, respectively. Rao[7] reported TSFT of 6.5 mm among primary school children inMaharashtra which was in accordance with the present study.
Conclusion
The anthropometric measurements of school girls was belowthe standards in both the groups. However, a significant increasein weight and MUAC was observed in E group after nutritioncounseling. This was due to increased food and nutrient intakeand also due to adoption of desirable nutritional practices like useof sprouted grains and other nutritious foods like milk and pulsesby subjects in E group. Thus nutrition counseling imparted to girlsalong with their mothers helped to improve the dietary status ofschool girls. With improvement in nutrition knowledge and dietarypractices, anthropometric profile of girls improved. Children havea high energy requirement because they are growing quickly andbecoming more active. A diet which is low in fat and high in fibre willnot provide enough energy for a young child but a family approach to a healthy diet is important at this stage because food preferencesare often established very early in life. Ideally, children should restrictthe number of times a day that they have foods and drinks containingsugar and then only have them at meal times. Young children shouldnot be put on weight reduction diets, but a healthy family approach tofood and regular physical activity are important in avoiding excessiveweight gain and obesity.
Instructions for Pragya Yoga Vyayama
The practice of pragya yoga vyayama starts with the mantrasand the body-mind awareness with the following instructions, Standerect, close the eyes and meditate on the brilliance of Lord Savita(power source of rising sun). Have the faith and inner felling thatthe spiritual power of Savita is rejuvenating the body, mind and soul.All chantings of Gayatri mantra syllable made with deep mentalengrossment, steady and deep breathing. Follow-with each syllableof Gayatri mantra- the sequence of pragya yoga vyayama asanas asfollows:
1. Tadasana: Stand on the toes. Chant ‘bhuh’ and raise your bothhands upward while inhaling gradually and deeply. Look upward tothe sky. (All the four actions should take place simultaneously). Holdyour breath inside.
2. Padahastasana: Chanting ‘bhuvah’, bring both the handsdownward from the posture of tadasana and exhale at the same slowand consistent pace and bow the head down to touch the knees, alsoattempt making the palms touch the floor. Do not bend your knees.Hold this position for some time.
3. Vajrasana (sawah): With the chant of ‘Swah’, place the toescompletely on the floor and set the haunches on the feet. Both the legsshould be in closed contact. Keep the backbone erect and place thepalms on the knees. Breathe normally during this posture.
4. Ustrasana: Now get up slightly from the vajrasana with a chanttof ‘tat’. Stand on your knees with the toes touching the floor and theheels facing backwards. Almost simultaneously, bend backwards toplace the palms on the heels from the backside. Inhale deeply whilelooking upwards. This will inflate your chest. Hold the breath for fewseconds.
5. Yogamudrasana: With the chanting of ‘Savituh’, exhale slowlyand sit on as in vajrasana at the same time, clench together both thepalms at the back and stretch upwardly and place the head on thefloor so that the chest and the stomach touch the thighs.
6. Ardhatadasana: Chanting ‘varenyam’, inhale deeply. Beingseated in the posture of vajrasana, raise both the arms and eyesupwards. Hold the breath inside and stretch the arms as much as youcan without pain. Focus your eyes on the hands.
7. Shashankasana: Chanting ‘bhargo’, exhale at the same pace asinhalation in the preceding asana. Simultaneously, sit in the postureof vajrasana and keep both the arms stretched outwardly in front ofthe chest. Place the palms on the floor, bend from the waist to makethe stomach touch the thighs and the head touch the floor.
8. Bhujangasana: Chanting ‘devasya’, inhale deeply and pullyour waist upwards. Toes and palm should remain at the same place where these were in the previous posture but now the arms arestraightened. The knees and thighs should touch the floor. Draw yourchest and head upwards and raise head like a snake’s hood. Hold thebreath inside and bend the head backwards slightly to stare at the sky.Do not strain to achieve this. Try to bring the hips as near to the flooras possible.
9. Tiryak bhujangasana- left: In the posture of bhujangasanaexhale slowly. Now inhale and with the chant ‘dhimahi’, turn theneck towards the left and try looking at the heel of right foot.
10. Tiryakbhujangasana- right: Chant ‘dhiyo’, inhale and turnthe neck towards the right to see the heel of the left foot.
11. Shashankasana: Chant ‘Yonaha’, Without moving yourlegs and hand bend your kees back and come back to sashangasanaposition as in posture of step 7.
12. Ardhatadasana: Chant ‘Prachodayat’, Deeply inhale andcome to the ardhatadasana position as in posture of step 6.
13. Utkathasana: After ardha tadasana in step 12, exhale slowly.Now chant ‘bhuh’, and with normal breathing sit on the toes. Theheel should not touch the floor. Let the calves touch the buttocks.Place both the palms on the knees. Bend the arms on elbows and keepthe hands in front of the chest with palm placed on each other in theposture of namaskar. Back, neck and head should be erect. Breathingshould be deep and continued at a consistent pace.
14. Padahastasana: Chanting ‘bhuwha’, keeping your palmsdown on the earth and raise your feet and legs simultaneously withexhalation similar as position in step 2.
References
- Awasthi N, Kumar AR (1999) Indian J Nutr Dietet 364: 59.
- Variyam JN (1999) Amer J Agric Eco 81: 84.
- Jelliffe DB (1966) The assessment of the nutritional status of the community. World Health Organisation, Geneva.
- Sangha JK (1999) Indian J Maternal Child Health 10: 55.
- Dutta A, Kumar J (1997) Indian J Nutr Dietet 34: 26.
- Parvathi EP, Poorani R (1991) Indian J Nutr Dietet 28: 14.
- Rao VK (1993) Indian J Nutr Dietet 30: 47.
- Gibson RS (1990) Principles of Nutritional Assessment, University Press, Oxford.