Research Article
Prevalence, Patterns, and Determinants of Malnutrition Among Children Under Five in the Mal Paharia Community, Littipara, Jharkhand
Khanang Y1, Chakraborty D2*
1Independent Researcher, Azim Premji University, Bengaluru, India
2Regional Head, Sarva Seva Samity Sanstha (4S India), Jharkhand, India
2Regional Head, Sarva Seva Samity Sanstha (4S India), Jharkhand, India
*Corresponding author:Debanjan Chakraborty, Regional Head, Sarva Seva Samity Sanstha (4S India), Jharkhand, India. E-mail Id: chakraborty.debanjan83@gmail.com
Article Information:Submission: 06/06/2026; Accepted: 23/06/2026; Published: 25/06/2026
Copyright: © 2026 Khanang Y, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Malnutrition among Particularly Vulnerable Tribal Groups (PVTGs) remains a major public health challenge in India. Children belonging to tribal communities experience disproportionately high levels of undernutrition due to poverty, food insecurity, poor sanitation, maternal anemia, and inadequate access to healthcare. The Mal Paharia community of Littipara block in Pakur district, Jharkhand, represents one of the most marginalized tribal populations
in eastern India.
A community-based cross-sectional study was conducted from June 1 to June 28, 2025, among 122 children aged 0-59 months from eight villages of Littipara block, Pakur district, Jharkhand. Children were selected through random sampling technique. Anthropometric measurements, including height and weight, were recorded using standard WHO protocols. Nutritional status was assessed by using WHO Child Growth Standards and the Poshan Calculator application. Data regarding maternal health, sanitation, dietary practices, and healthcare access were collected through interview method using close ended questionnaire and field observations.
The study included 67 boys and 55 girls under five years of age. Moderate Acute Malnutrition (MAM) was observed among 19.6% of children, while Severe Acute Malnutrition (SAM) was identified among 3.2% of children. Maternal anemia prevalence exceeded 80% among screened women. Open defecation was practiced by 85.96% of households. Poor dietary diversity, adolescent pregnancies, inadequate breastfeeding practices, recurrent infections, dependence on traditional healers, and weak ICDS implementation emerged as major determinants of malnutrition.
Malnutrition among Mal Paharia children is strongly associated with structural poverty, maternal undernutrition, food insecurity, poor sanitation, and inadequate healthcare access. Community-based nutrition interventions, strengthening of ICDS services, maternal health support, and culturally sensitive public health planning are urgently required to improve nutritional outcomes among PVTG populations.
A community-based cross-sectional study was conducted from June 1 to June 28, 2025, among 122 children aged 0-59 months from eight villages of Littipara block, Pakur district, Jharkhand. Children were selected through random sampling technique. Anthropometric measurements, including height and weight, were recorded using standard WHO protocols. Nutritional status was assessed by using WHO Child Growth Standards and the Poshan Calculator application. Data regarding maternal health, sanitation, dietary practices, and healthcare access were collected through interview method using close ended questionnaire and field observations.
The study included 67 boys and 55 girls under five years of age. Moderate Acute Malnutrition (MAM) was observed among 19.6% of children, while Severe Acute Malnutrition (SAM) was identified among 3.2% of children. Maternal anemia prevalence exceeded 80% among screened women. Open defecation was practiced by 85.96% of households. Poor dietary diversity, adolescent pregnancies, inadequate breastfeeding practices, recurrent infections, dependence on traditional healers, and weak ICDS implementation emerged as major determinants of malnutrition.
Malnutrition among Mal Paharia children is strongly associated with structural poverty, maternal undernutrition, food insecurity, poor sanitation, and inadequate healthcare access. Community-based nutrition interventions, strengthening of ICDS services, maternal health support, and culturally sensitive public health planning are urgently required to improve nutritional outcomes among PVTG populations.
Keywords: Malnutrition; Mal Paharia; PVTG; Maternal Anemia; Child Nutrition; Jharkhand
Introduction
Malnutrition remains one of the leading causes of childhood
morbidity and mortality in developing countries. Children under five
years of age are particularly vulnerable to growth faltering, recurrent
infections, developmental delays, and mortality due to inadequate
nutrition and poor healthcare access. Globally, approximately 149
million children under five years are stunted, 45 million are wasted,
and 462 million are underweight. Tribal populations in India
experience significantly higher rates of malnutrition than non-tribal
communities due to socio-economic deprivation, poor sanitation,
geographic isolation, and limited healthcare infrastructure.
India has 75 officially recognized Particularly Vulnerable
Tribal Groups (PVTGs) distributed across 18 states and one Union
Territory. These communities face severe structural inequalities
affecting nutrition, healthcare, education, and livelihoods. According
to UNICEF reports, nearly 4.7 million tribal children in India suffer
from chronic nutritional deprivation, with high prevalence of
stunting and wasting among under-five children.
The Mal Paharia community residing in the hilly regions of
Littipara block in Pakur district, Jharkhand, is among the most
marginalized PVTGs in eastern India. The community experiences
poor road connectivity, food insecurity, low literacy, early marriage,
maternal anemia, and inadequate access to healthcare services. Despite
the implementation of government schemes such as Integrated Child
Development Services (ICDS) and POSHAN Abhiyaan, nutritional
outcomes among children remain poor.
Limited scientific literature is available regarding malnutrition among the Mal Paharia population. Most tribal nutrition studies in India focus on broader Scheduled Tribe populations, while PVTG specific evidence remains inadequate. Therefore, the present study was conducted to assess the prevalence and determinants of malnutrition among under-five children in the Mal Paharia community of Littipara block.
Limited scientific literature is available regarding malnutrition among the Mal Paharia population. Most tribal nutrition studies in India focus on broader Scheduled Tribe populations, while PVTG specific evidence remains inadequate. Therefore, the present study was conducted to assess the prevalence and determinants of malnutrition among under-five children in the Mal Paharia community of Littipara block.
Objectives
1. To assess the prevalence of malnutrition among under-five
children in the Mal Paharia community.
2. To identify socio-economic, maternal, and environmental determinants associated with malnutrition.
3. To examine access to healthcare and nutrition services among the study population.
4. To evaluate the implementation challenges of ICDS and related nutrition programs in PVTG villages.
5. To explore the intergenerational factors contributing to child malnutrition.
2. To identify socio-economic, maternal, and environmental determinants associated with malnutrition.
3. To examine access to healthcare and nutrition services among the study population.
4. To evaluate the implementation challenges of ICDS and related nutrition programs in PVTG villages.
5. To explore the intergenerational factors contributing to child malnutrition.
Literature Review:
Malnutrition among tribal populations in India continues to
be a major public health challenge, particularly among Particularly
Vulnerable Tribal Groups (PVTGs) residing in geographically isolated
and socio-economically marginalized regions. Despite significant
improvements in national nutrition indicators over the last decade,
tribal communities continue to experience disproportionately high
levels of undernutrition, anemia, infectious diseases, and limited
access to healthcare services. According to UNICEF (2023) [1] tribal
children remain among the most nutritionally vulnerable populations
in India due to persistent poverty, food insecurity, inadequate
sanitation, and poor maternal health.Studies conducted across tribal regions have consistently reported higher prevalence of stunting, wasting, and underweight among children compared to non-tribal populations. Spears (2020) [2] demonstrated a strong association between poor sanitation and childhood undernutrition in India, showing that open defecation contributes significantly to recurrent infections, environmental enteropathy, and impaired nutrient absorption. Such conditions are particularly prevalent in remote tribal settlements where sanitation infrastructure remains weak and access to safe drinking water is limited.
Research among PVTGs in Odisha by Das et al. (2019) [3]
reported alarming levels of wasting, stunting, and anemia among
under-five children. The study highlighted food insecurity, seasonal
hunger, poor dietary diversity, and inadequate maternal nutrition as
major contributors to child malnutrition. Similar observations have
been reported among tribal communities in Jharkhand, Chhattisgarh,
and Madhya Pradesh, where dependence on cereal-based diets and
limited consumption of protein-rich foods have contributed to
chronic nutritional deficiencies.
Maternal health has been widely recognized as a critical determinant of child nutritional outcomes. Madankar et al. (2018) [4] reported that maternal undernutrition, adolescent pregnancies, repeated childbirths, and inadequate antenatal care significantly increase the risk of child malnutrition among tribal populations. Likewise, Didzun et al. (2019) [5] found that maternal anemia is strongly associated with low birth weight, impaired child growth, poor cognitive development, and increased susceptibility to childhood infections. These findings underline the intergenerational nature of malnutrition, where poor maternal nutritional status directly influences child health outcomes.
Maternal health has been widely recognized as a critical determinant of child nutritional outcomes. Madankar et al. (2018) [4] reported that maternal undernutrition, adolescent pregnancies, repeated childbirths, and inadequate antenatal care significantly increase the risk of child malnutrition among tribal populations. Likewise, Didzun et al. (2019) [5] found that maternal anemia is strongly associated with low birth weight, impaired child growth, poor cognitive development, and increased susceptibility to childhood infections. These findings underline the intergenerational nature of malnutrition, where poor maternal nutritional status directly influences child health outcomes.
The Expert Committee on Tribal Health (2018) emphasized
that tribal communities continue to face substantial barriers in
accessing healthcare services due to geographic isolation, shortages of
healthcare personnel, weak infrastructure, and inadequate culturally
sensitive service delivery. Nikitin et al. (2020) [6] further observed that
structural poverty, social exclusion, and poor healthcare accessibility
remain key drivers of nutritional inequities among indigenous
populations.
Although considerable literature exists on tribal nutrition in India, studies specifically focusing on the Mal Paharia community of Jharkhand remain extremely limited. Most available evidence pertains to broader Scheduled Tribe populations, leaving important knowledge gaps regarding the nutritional vulnerabilities of this community. Therefore, the present study seeks to contribute to the existing literature by examining the prevalence, patterns, and determinants of malnutrition among under-five children belonging to the Mal Paharia community of Littipara Block, Jharkhand.
Although considerable literature exists on tribal nutrition in India, studies specifically focusing on the Mal Paharia community of Jharkhand remain extremely limited. Most available evidence pertains to broader Scheduled Tribe populations, leaving important knowledge gaps regarding the nutritional vulnerabilities of this community. Therefore, the present study seeks to contribute to the existing literature by examining the prevalence, patterns, and determinants of malnutrition among under-five children belonging to the Mal Paharia community of Littipara Block, Jharkhand.
Materials and Methods
The present study adopted a community-based cross-sectional
descriptive research design. This design was considered appropriate
for estimating the prevalence and determinants of malnutrition
among under-five children in the Mal Paharia community at a specific
point in time. The study was conducted during June 2025 across eight
villages of Littipara Block, Pakur District, Jharkhand.
Children aged 0–59 months were selected using random sampling
methods for anthropometric assessment. Purposive sampling was
additionally used for focused group discussions and qualitative
interviews with mothers and caregivers. The minimum sample size
was estimated at 122 using Cochran’s sample size formula for large
populations, and a total of 122 children participated in the study.
Anthropometric measurements, including weight and height, were recorded using calibrated digital weighing scales and portable stadiometers following WHO standard protocols. Weight was measured to the nearest 0.1 kg and height/length to the nearest 0.1 cm. Age was verified through parental reporting and cross-checked with available records and senior household members whenever possible.
Data regarding maternal health, dietary diversity, sanitation practices, infant feeding behavior, healthcare access, and socioeconomic conditions were collected through household interviews, focused group discussions, and field observations using semistructured questionnaires.
Nutritional status was assessed using WHO Child Growth Standards. Children with weight-for-height Z-scores below −3 SD were classified as Severe Acute Malnutrition (SAM), while those between −2 SD and −3 SD were categorized as Moderate Acute Malnutrition (MAM). The Poshan Calculator mobile application was used for classification and nutritional assessment. Data were entered and analyzed using Microsoft Excel 2019. Descriptive statistical methods, including frequencies, percentages, means, and standard deviations, were used to assess the prevalence and distribution of malnutrition indicators.
The study was conducted under academic supervision as part of postgraduate field research. Informed verbal consent was obtained from parents and caregivers before participation. Confidentiality and anonymity of respondents were maintained throughout the study.
Anthropometric measurements, including weight and height, were recorded using calibrated digital weighing scales and portable stadiometers following WHO standard protocols. Weight was measured to the nearest 0.1 kg and height/length to the nearest 0.1 cm. Age was verified through parental reporting and cross-checked with available records and senior household members whenever possible.
Data regarding maternal health, dietary diversity, sanitation practices, infant feeding behavior, healthcare access, and socioeconomic conditions were collected through household interviews, focused group discussions, and field observations using semistructured questionnaires.
Nutritional status was assessed using WHO Child Growth Standards. Children with weight-for-height Z-scores below −3 SD were classified as Severe Acute Malnutrition (SAM), while those between −2 SD and −3 SD were categorized as Moderate Acute Malnutrition (MAM). The Poshan Calculator mobile application was used for classification and nutritional assessment. Data were entered and analyzed using Microsoft Excel 2019. Descriptive statistical methods, including frequencies, percentages, means, and standard deviations, were used to assess the prevalence and distribution of malnutrition indicators.
The study was conducted under academic supervision as part of postgraduate field research. Informed verbal consent was obtained from parents and caregivers before participation. Confidentiality and anonymity of respondents were maintained throughout the study.
Limitations of the Study:
The present study has certain limitations that should be considered
while interpreting the findings. First, the study was conducted in only
eight villages of Littipara block with a relatively small sample size of
122 children; therefore, the findings may not be fully generalizable to
the entire Mal Paharia population or other Particularly Vulnerable
Tribal Groups (PVTGs) in Jharkhand. Second, the cross-sectional
design of the study limits the ability to establish causal relationships
between malnutrition and its associated determinants. Third,
information regarding age, feeding practices, dietary intake, and
illness history was largely dependent on parental recall, which may
have introduced recall bias.Due to the limited availability of medical records and birth certificates in remote tribal areas, exact age verification was challenging in some cases. The study also relied primarily on anthropometric indicators and did not include biochemical assessments such as hemoglobin estimation among children. Seasonal variations in food availability and disease burden were not assessed because data collection was conducted within a limited time period. Despite these limitations, the study provides important baseline evidence regarding malnutrition and related structural vulnerabilities among the Mal Paharia community.
Findings:
The present study assessed the nutritional status of 122 children
aged 0–59 months belonging to the Mal Paharia community across
eight villages of Littipara block, Pakur district, Jharkhand. Among the
total participants, 67 were boys and 55 were girls.[Table 1] presents the distribution of under five children by nutritional status. The study identified that 24 children (19.6%) were suffering from Moderate Acute Malnutrition (MAM), while 4 children (3.2%) were classified under Severe Acute Malnutrition (SAM). A total of 94 children (77.0%) were found to have normal nutritional status according to WHO growth standards. Although the majority of children were categorized as nutritionally normal, nearly one-fourth of the study population was affected by acute malnutrition, indicating substantial nutritional vulnerability within the community. The prevalence of MAM reflects chronic nutritional stress and inadequate dietary intake, while the presence of SAM cases indicates severe nutritional deprivation requiring immediate medical and nutritional intervention.
Nearly one out of every five children were identified with Moderate
Acute Malnutrition, indicating widespread nutritional insufficiency
and inadequate dietary diversity. Although the proportion of Severe
Acute Malnutrition cases was comparatively lower, the presence of
SAM remains clinically significant because severely malnourished
children face substantially higher risks of infections, developmental
delays, and mortality.
The table also highlights the broader structural determinants
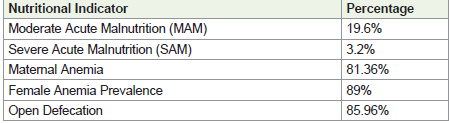
associated with poor nutritional outcomes. Maternal anemia
prevalence exceeded 81%, while anemia among women reached
89%, reflecting severe maternal nutritional deprivation within the
community. Such high levels of anemia among women adversely
affect pregnancy outcomes, breastfeeding practices, and child
growth. Open defecation was practiced by nearly 86% of households,
indicating poor sanitation and increased exposure to water-borne
and infectious diseases. These findings suggest that child malnutrition
in the Mal Paharia community is closely linked with maternal health,
sanitation, poverty, and weak healthcare access rather than food
insecurity alone.
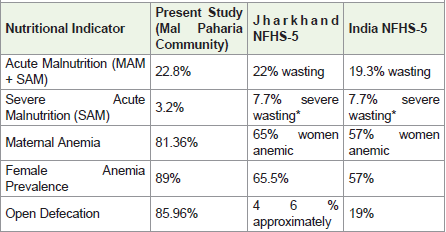
[Table 2] The prevalence of acute malnutrition (22.8%) observed in the present study is comparable to findings reported among PVTG populations in Odisha by Das et al. (2019) [3] and remains higher than national estimates reported in NFHS-5 (2021). These findings indicate that PVTG communities continue to experience disproportionate nutritional deprivation despite the implementation of national nutrition programs.
Maternal anemia prevalence (81.36%) substantially exceeded both state and national averages, supporting observations made by Didzun et al. (2019) regarding the influence of maternal nutritional status on child health outcomes. The high prevalence of open defecation (85.96%) also supports findings by Spears (2020) [2], who reported strong associations between poor sanitation and child undernutrition. Overall, the comparative findings suggest that generalized nutrition interventions may be insufficient for remote tribal populations unless
[Table 2] The prevalence of acute malnutrition (22.8%) observed in the present study is comparable to findings reported among PVTG populations in Odisha by Das et al. (2019) [3] and remains higher than national estimates reported in NFHS-5 (2021). These findings indicate that PVTG communities continue to experience disproportionate nutritional deprivation despite the implementation of national nutrition programs.
Maternal anemia prevalence (81.36%) substantially exceeded both state and national averages, supporting observations made by Didzun et al. (2019) regarding the influence of maternal nutritional status on child health outcomes. The high prevalence of open defecation (85.96%) also supports findings by Spears (2020) [2], who reported strong associations between poor sanitation and child undernutrition. Overall, the comparative findings suggest that generalized nutrition interventions may be insufficient for remote tribal populations unless
supported by culturally sensitive and region-specific public health
strategies.
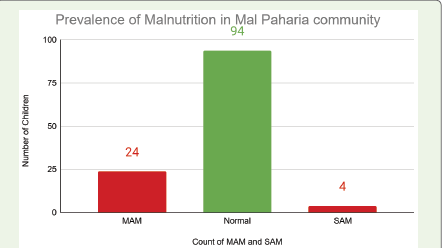
[Figure 1] presents the numerical distribution of nutritional categories among 122 under-five children from the Mal Paharia community. Out of the total children assessed, 94 children (77.0%) were found to have normal nutritional status, while 24 children (19.6%) were categorized under Moderate Acute Malnutrition and 4 children (3.2%) under Severe Acute Malnutrition. The figure indicates that nearly one in every four children in the study area was affected by some form of acute malnutrition.
The comparatively high number of MAM cases suggests persistent nutritional stress within households, likely associated with poor dietary diversity, recurrent infections, and inadequate feeding practices. Although the number of SAM cases was lower, these children remain at high risk of severe infections, developmental impairment, and mortality without timely intervention. The figure further demonstrates that nutritional inequality exists within the same community, where a majority of children maintain normal nutritional status while a substantial minority remains highly vulnerable to undernutrition.
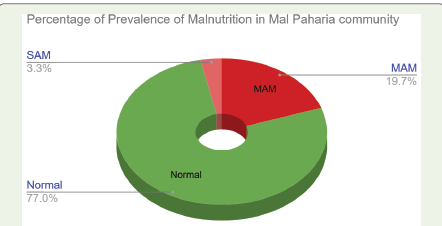
[Figure 2] illustrates the percentage-wise distribution of nutritional status among children in the study area. The chart shows that 77.0% of children were nutritionally normal, whereas 19.7% were affected by Moderate Acute Malnutrition and 3.3% by Severe Acute Malnutrition. Together, approximately 23% of children were suffering from acute malnutrition, highlighting a considerable public health concern within the community.
The figure demonstrates that Moderate Acute Malnutrition constituted the largest proportion of malnutrition cases, affecting nearly one-fifth of the children surveyed. This reflects chronic nutritional insecurity and inadequate intake of micronutrient-rich foods among households. The relatively smaller proportion of SAM cases remains important from a public health perspective because children with severe malnutrition require urgent therapeutic and medical support. The graphical findings also indicate that child malnutrition among the Mal Paharia community is influenced by broader socio-economic and environmental determinants, including maternal anemia, poor sanitation, inadequate healthcare access, and poverty.
[Figure 1] presents the numerical distribution of nutritional categories among 122 under-five children from the Mal Paharia community. Out of the total children assessed, 94 children (77.0%) were found to have normal nutritional status, while 24 children (19.6%) were categorized under Moderate Acute Malnutrition and 4 children (3.2%) under Severe Acute Malnutrition. The figure indicates that nearly one in every four children in the study area was affected by some form of acute malnutrition.
The comparatively high number of MAM cases suggests persistent nutritional stress within households, likely associated with poor dietary diversity, recurrent infections, and inadequate feeding practices. Although the number of SAM cases was lower, these children remain at high risk of severe infections, developmental impairment, and mortality without timely intervention. The figure further demonstrates that nutritional inequality exists within the same community, where a majority of children maintain normal nutritional status while a substantial minority remains highly vulnerable to undernutrition.
[Figure 2] illustrates the percentage-wise distribution of nutritional status among children in the study area. The chart shows that 77.0% of children were nutritionally normal, whereas 19.7% were affected by Moderate Acute Malnutrition and 3.3% by Severe Acute Malnutrition. Together, approximately 23% of children were suffering from acute malnutrition, highlighting a considerable public health concern within the community.
The figure demonstrates that Moderate Acute Malnutrition constituted the largest proportion of malnutrition cases, affecting nearly one-fifth of the children surveyed. This reflects chronic nutritional insecurity and inadequate intake of micronutrient-rich foods among households. The relatively smaller proportion of SAM cases remains important from a public health perspective because children with severe malnutrition require urgent therapeutic and medical support. The graphical findings also indicate that child malnutrition among the Mal Paharia community is influenced by broader socio-economic and environmental determinants, including maternal anemia, poor sanitation, inadequate healthcare access, and poverty.
Major Determinants of Malnutrition:
Field observations revealed that malnutrition among Mal Paharia
children is strongly associated with multiple interrelated socioeconomic
and environmental factors. One of the most significant
determinants identified during the study was maternal anemia. A
health camp conducted among 279 tribal individuals reported anemia
among 81.36% participants, with female anemia prevalence reaching
89%. Women suffering from anemia often experienced fatigue,
weakness, low dietary intake, and poor reproductive health, which
directly affected child nutrition outcomes. Maternal undernutrition
contributed to low birth weight, poor breastfeeding practices, andintergenerational transmission of malnutrition.
Poor dietary diversity emerged as another major determinant. Most households depended primarily on rice, lentils, and seasonal forest produce for survival. Although protein-rich crops such as bajra, kurti, and arhar were cultivated, these were often sold in local markets for income generation instead of household consumption. Consumption of fruits, milk, eggs, and animal protein remained extremely limited among children. As a result, children were deprived of essential micronutrients necessary for growth and immunity.
The study also observed widespread early marriage and adolescent pregnancy among Mal Paharia women. Many girls became mothers before the age of 20 years, increasing risks of maternal undernutrition, low birth weight deliveries, and poor child health outcomes. Repeated pregnancies and lack of antenatal care further weakened maternal nutritional status.
Sanitation conditions in the villages were extremely poor. Open defecation was practiced by 85.96% households, and access to safe drinking water remained limited. Frequent infections such as diarrhea, typhoid, skin diseases, and malaria were commonly reported among children. These recurrent illnesses reduced nutrient absorption and weakened immunity, thereby worsening malnutrition.
Geographic isolation and poor transportation significantly restricted access to healthcare services. Several villages lacked nearby Anganwadi centres and healthcare facilities. Community dependence on traditional healers and informal practitioners delayed treatment for malnutrition and infectious diseases. Operational challenges within ICDS services, including inadequate staffing, poor monitoring, and irregular food distribution, further limited the effectiveness of nutrition interventions in the study area.
Overall, the findings of the present study indicate that the nutritional burden among Mal Paharia children remains comparable to or worse than broader tribal and state-level averages. The prevalence of acute malnutrition observed in the study highlights the persistent exclusion of PVTGs from mainstream nutrition and healthcare interventions. High maternal anemia, poor dietary diversity, inadequate sanitation, and weak healthcare access further intensify the nutritional crisis within the community.
Poor dietary diversity emerged as another major determinant. Most households depended primarily on rice, lentils, and seasonal forest produce for survival. Although protein-rich crops such as bajra, kurti, and arhar were cultivated, these were often sold in local markets for income generation instead of household consumption. Consumption of fruits, milk, eggs, and animal protein remained extremely limited among children. As a result, children were deprived of essential micronutrients necessary for growth and immunity.
The study also observed widespread early marriage and adolescent pregnancy among Mal Paharia women. Many girls became mothers before the age of 20 years, increasing risks of maternal undernutrition, low birth weight deliveries, and poor child health outcomes. Repeated pregnancies and lack of antenatal care further weakened maternal nutritional status.
Sanitation conditions in the villages were extremely poor. Open defecation was practiced by 85.96% households, and access to safe drinking water remained limited. Frequent infections such as diarrhea, typhoid, skin diseases, and malaria were commonly reported among children. These recurrent illnesses reduced nutrient absorption and weakened immunity, thereby worsening malnutrition.
Geographic isolation and poor transportation significantly restricted access to healthcare services. Several villages lacked nearby Anganwadi centres and healthcare facilities. Community dependence on traditional healers and informal practitioners delayed treatment for malnutrition and infectious diseases. Operational challenges within ICDS services, including inadequate staffing, poor monitoring, and irregular food distribution, further limited the effectiveness of nutrition interventions in the study area.
Overall, the findings of the present study indicate that the nutritional burden among Mal Paharia children remains comparable to or worse than broader tribal and state-level averages. The prevalence of acute malnutrition observed in the study highlights the persistent exclusion of PVTGs from mainstream nutrition and healthcare interventions. High maternal anemia, poor dietary diversity, inadequate sanitation, and weak healthcare access further intensify the nutritional crisis within the community.
Discussion
The present study highlights the substantial burden of malnutrition
among under-five children belonging to the Mal Paharia community
of Littipara Block, Pakur District, Jharkhand. The findings revealed
that 22.8% of children were affected by acute malnutrition, including
19.6% with Moderate Acute Malnutrition (MAM) and 3.2% with
Severe Acute Malnutrition (SAM). These findings indicate persistent
nutritional vulnerability among this Particularly Vulnerable Tribal
Group (PVTG) and reflect continuing inequalities in nutrition,
healthcare access, and socio-economic development. The prevalence
observed in the present study underscores the fact that despite
ongoing national nutrition programmes, significant disparities
continue to exist among marginalized tribal communities.
The prevalence of acute malnutrition observed in the study was
slightly higher than the wasting prevalence reported for Jharkhand
in NFHS-5 (2021) [7] and notably higher than the national average.
Similar findings have been reported among tribal and PVTG
populations in Odisha, Madhya Pradesh, and Chhattisgarh. Das et al.
(2019) documented high levels of wasting and undernutrition among
PVTG children in Odisha, while UNICEF (2023) [1] highlighted
that tribal children continue to experience a disproportionate
burden of malnutrition compared to non-tribal populations. The
findings of the present study therefore reinforce existing evidence
that tribal communities remain nutritionally disadvantaged despite
improvements observed at the national level.
One of the most significant findings of the study was the extremely high prevalence of maternal anemia. More than 81% of screened individuals were found to be anemic, while anemia among women reached 89%, substantially exceeding both state and national averages reported in NFHS-5. Maternal anemia has long been recognized as a critical determinant of child nutrition and survival. Didzun et al. (2019) demonstrated that maternal anemia is significantly associated with low birth weight, impaired child growth, and increased susceptibility to infections during early childhood. Similarly, recent studies on maternal and child nutrition have emphasized that maternal undernutrition contributes directly to the intergenerational transmission of malnutrition. The findings of the present study therefore highlight the urgent need to strengthen maternal nutrition interventions among PVTG populations.
Poor dietary diversity emerged as another major determinant of child malnutrition. Most households depended primarily on rice, lentils, and seasonal forest produce, while regular consumption of milk, eggs, fruits, and animal protein remained limited. Although protein-rich crops such as bajra, arhar, and kurti were cultivated locally, these were frequently sold in local markets to meet household cash requirements rather than consumed domestically. Similar observations have been reported by Dasra (2021) [8], which noted that economic constraints often compel tribal households to prioritize income generation over nutritional consumption. Such dietary patterns increase the risk of deficiencies in protein, iron, zinc, and other micronutrients essential for growth, cognitive development, and immunity.
Early marriage and adolescent pregnancy further intensified nutritional vulnerability within the community. Many women became mothers before the age of twenty years and experienced repeated pregnancies with inadequate antenatal care. Madankar et al. (2018) [4] reported similar findings among tribal populations and observed that adolescent pregnancy significantly increases the likelihood of maternal undernutrition, low-birth-weight deliveries, and poor child growth outcomes. WHO has also identified adolescent motherhood as an important risk factor for adverse maternal and child health outcomes. These observations suggest that improving adolescent health and delaying the age of marriage may contribute significantly to breaking the cycle of intergenerational malnutrition.
One of the most significant findings of the study was the extremely high prevalence of maternal anemia. More than 81% of screened individuals were found to be anemic, while anemia among women reached 89%, substantially exceeding both state and national averages reported in NFHS-5. Maternal anemia has long been recognized as a critical determinant of child nutrition and survival. Didzun et al. (2019) demonstrated that maternal anemia is significantly associated with low birth weight, impaired child growth, and increased susceptibility to infections during early childhood. Similarly, recent studies on maternal and child nutrition have emphasized that maternal undernutrition contributes directly to the intergenerational transmission of malnutrition. The findings of the present study therefore highlight the urgent need to strengthen maternal nutrition interventions among PVTG populations.
Poor dietary diversity emerged as another major determinant of child malnutrition. Most households depended primarily on rice, lentils, and seasonal forest produce, while regular consumption of milk, eggs, fruits, and animal protein remained limited. Although protein-rich crops such as bajra, arhar, and kurti were cultivated locally, these were frequently sold in local markets to meet household cash requirements rather than consumed domestically. Similar observations have been reported by Dasra (2021) [8], which noted that economic constraints often compel tribal households to prioritize income generation over nutritional consumption. Such dietary patterns increase the risk of deficiencies in protein, iron, zinc, and other micronutrients essential for growth, cognitive development, and immunity.
Early marriage and adolescent pregnancy further intensified nutritional vulnerability within the community. Many women became mothers before the age of twenty years and experienced repeated pregnancies with inadequate antenatal care. Madankar et al. (2018) [4] reported similar findings among tribal populations and observed that adolescent pregnancy significantly increases the likelihood of maternal undernutrition, low-birth-weight deliveries, and poor child growth outcomes. WHO has also identified adolescent motherhood as an important risk factor for adverse maternal and child health outcomes. These observations suggest that improving adolescent health and delaying the age of marriage may contribute significantly to breaking the cycle of intergenerational malnutrition.
Poor sanitation and environmental health conditions also
emerged as important contributors to malnutrition. Open defecation
was practiced by nearly 86% of households, while access to safe
drinking water remained inadequate. Frequent illnesses such as
diarrhea, malaria, typhoid, and skin infections were commonly
reported during field observations. Spears (2020) [2] demonstrated
that poor sanitation and exposure to open defecation contribute
substantially to childhood stunting and growth faltering through
recurrent infections and environmental enteropathy. Recurrent
illness reduces nutrient absorption, increases metabolic stress, and
compromises immunity, thereby worsening nutritional outcomes.
The sanitation profile observed in the present study therefore
represents a significant public health concern requiring immediate
attention.
Limited healthcare accessibility further aggravated the nutritional burden in the study villages. Geographic isolation, poor road connectivity, and long distances from healthcare facilities restricted access to maternal and child healthcare services. Several villages lacked adequately functioning Anganwadi Centres and health subcentres. The Expert Committee on Tribal Health (2018) highlighted similar barriers among tribal populations across India and emphasized the need for culturally appropriate and geographically accessible healthcare services. Dependence on traditional healers and informal healthcare providers often delayed treatment for infections and malnutrition. Weak implementation of ICDS services, including irregular growth monitoring and inconsistent supplementary nutrition distribution, further reduced the effectiveness of government nutrition interventions.
The findings of the present study indicate that malnutrition among the Mal Paharia community is deeply rooted in structural poverty, social exclusion, maternal deprivation, inadequate healthcare infrastructure, poor sanitation, and food insecurity. The study contributes important baseline evidence regarding nutritional vulnerabilities among the Mal Paharia community, for which scientific literature remains limited. The findings emphasize that generalized nutrition interventions alone may be insufficient unless accompanied by culturally sensitive, community-based, and region specific strategies. Long-term improvements in child nutrition among PVTGs will require coordinated investments in maternal health, adolescent nutrition, sanitation, healthcare accessibility, livelihood enhancement, women’s empowerment, education, and effective implementation of nutrition programmes such as ICDS and POSHAN Abhiyaan.
Limited healthcare accessibility further aggravated the nutritional burden in the study villages. Geographic isolation, poor road connectivity, and long distances from healthcare facilities restricted access to maternal and child healthcare services. Several villages lacked adequately functioning Anganwadi Centres and health subcentres. The Expert Committee on Tribal Health (2018) highlighted similar barriers among tribal populations across India and emphasized the need for culturally appropriate and geographically accessible healthcare services. Dependence on traditional healers and informal healthcare providers often delayed treatment for infections and malnutrition. Weak implementation of ICDS services, including irregular growth monitoring and inconsistent supplementary nutrition distribution, further reduced the effectiveness of government nutrition interventions.
The findings of the present study indicate that malnutrition among the Mal Paharia community is deeply rooted in structural poverty, social exclusion, maternal deprivation, inadequate healthcare infrastructure, poor sanitation, and food insecurity. The study contributes important baseline evidence regarding nutritional vulnerabilities among the Mal Paharia community, for which scientific literature remains limited. The findings emphasize that generalized nutrition interventions alone may be insufficient unless accompanied by culturally sensitive, community-based, and region specific strategies. Long-term improvements in child nutrition among PVTGs will require coordinated investments in maternal health, adolescent nutrition, sanitation, healthcare accessibility, livelihood enhancement, women’s empowerment, education, and effective implementation of nutrition programmes such as ICDS and POSHAN Abhiyaan.
Conclusion
The present study highlights the significant burden of malnutrition
among under-five children in the Mal Paharia community of Littipara
block, Pakur district, Jharkhand. The findings revealed that 19.6% of
children were affected by Moderate Acute Malnutrition (MAM) and
3.2% by Severe Acute Malnutrition (SAM), indicating substantial
nutritional vulnerability among this Particularly Vulnerable Tribal
Group (PVTG). The study further identified extremely high levels
of maternal anemia (81.36%), widespread open defecation (85.96%),
poor dietary diversity, recurrent infections, adolescent pregnancy,
and limited healthcare access as major determinants contributing to
child malnutrition.
The findings demonstrate that malnutrition among the Mal Paharia community is not merely a consequence of inadequate food intake but is deeply associated with structural poverty, maternal undernutrition, poor sanitation, weak healthcare infrastructure, and social exclusion. Geographic isolation, irregular functioning of ICDS services, and dependence on informal healthcare providers further increase nutritional risks among children and mothers.
The study carries important policy implications for tribal health and nutrition planning in Jharkhand and similar PVTG-dominated regions. Existing nutrition interventions need to move beyond generalized approaches and adopt culturally sensitive, communitybased, and region-specific strategies. Strengthening ICDS and Poshan Abhiyaan implementation in remote tribal areas, improving maternal and adolescent nutrition services, ensuring regular anthropometric monitoring, enhancing sanitation and safe drinking water access, and increasing healthcare outreach through mobile and community health systems are urgently required.
Focused investments in women’s education, livelihood support, nutrition awareness, and tribal healthcare infrastructure are essential to break the intergenerational cycle of malnutrition. Sustainable improvement in nutritional outcomes among PVTGs will require integrated policy approaches combining nutrition, public health, sanitation, social protection, and community participation.
The findings demonstrate that malnutrition among the Mal Paharia community is not merely a consequence of inadequate food intake but is deeply associated with structural poverty, maternal undernutrition, poor sanitation, weak healthcare infrastructure, and social exclusion. Geographic isolation, irregular functioning of ICDS services, and dependence on informal healthcare providers further increase nutritional risks among children and mothers.
The study carries important policy implications for tribal health and nutrition planning in Jharkhand and similar PVTG-dominated regions. Existing nutrition interventions need to move beyond generalized approaches and adopt culturally sensitive, communitybased, and region-specific strategies. Strengthening ICDS and Poshan Abhiyaan implementation in remote tribal areas, improving maternal and adolescent nutrition services, ensuring regular anthropometric monitoring, enhancing sanitation and safe drinking water access, and increasing healthcare outreach through mobile and community health systems are urgently required.
Focused investments in women’s education, livelihood support, nutrition awareness, and tribal healthcare infrastructure are essential to break the intergenerational cycle of malnutrition. Sustainable improvement in nutritional outcomes among PVTGs will require integrated policy approaches combining nutrition, public health, sanitation, social protection, and community participation.
Acknowledgment
The authors express sincere gratitude to the members of the Mal
Paharia community for their participation, cooperation, and support
during the study. The authors also acknowledge the support provided
by Azim Premji University, Sarva Seva Samity Sanstha (4S India),
field teams, frontline workers, and changemakers who assisted during
data collection and field activities.
Special thanks are extended to Dr. Smitana Saikia for academic guidance and to all community stakeholders and well-wishers who contributed directly or indirectly to the successful completion of the study.
Special thanks are extended to Dr. Smitana Saikia for academic guidance and to all community stakeholders and well-wishers who contributed directly or indirectly to the successful completion of the study.
References
Citation
Khanang Y, Chakraborty D. Prevalence, Patterns, and Determinants of Malnutrition Among Children Under Five in the Mal Paharia Community, Littipara, Jharkhand. Indian J Nutri. 2026;13(2): 346.