Research Article
Anaemia in Marginalized Communities: Evidence from the Mal Pahariya PVTG in Littipara Block, Jharkhand
Chakraborty D*, Kar SC and Sengupta M
Sarva Seva Samity Sanstha (4S India) and all Village Development Committees of involved villages, Jharkhand, India
*Corresponding author:Debanjan Chakraborty, Sarva Seva Samity Sanstha (4S India) and all Village Development Committees of involved villages, Jharkhand, India, Email: debanjan4sindia@gmail.com
Article Information:Submission: 08/04/2026; Accepted: 05/05/2026; Published: 07/05/2026
Copyright: ©2026 Chakraborty D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Anaemia remains a persistent public health issue in India, disproportionately affecting women, children, and marginalized communities. According to the National Family Health Survey-5 (NFHS-5), 65.3% of women aged 15-49 and 31.1% of men aged 15-49 in Jharkhand are anaemic. However, granular data on anaemia prevalence among Particularly Vulnerable Tribal Groups (PVTGs), such as the Mal Pahariya community in Jharkhand’s Littipara Block, is limited. This study aims to bridge that limited disaggregated data by presenting field-based haemoglobin screening results from eight remote villages across two panchayats, namely Littipara and Karmatarn in Pakur district.
A total of 278 individuals from villages including Makhnipahar, Keradoli, Jhapri, Kathalpara, Durio, Bada Pokhariya, Chota Pokhariya, and Gadapahari were tested for haemoglobin levels through community health camps in June 2025. The collected blood samples were analyzed to identify cases of anaemia based on World Health Organization (WHO) thresholds (<12 g/dL for women and <13 g/dL for men). The findings reveal a significant public health challenge, with an 82% overall anaemia prevalence. Gender-disaggregated data highlights that 90.1% of women and 67% of men tested were anaemic—significantly higher than state averages. Anaemia rates were especially alarming among adolescent girls, women, and elderly women, suggesting chronic nutritional deficiencies compounded by limited access to healthcare, clean water, and dietary diversity. This study highlights the urgent need for nutritional and preventive health interventions in PVTG-dominated geographies and reinforces the call for disaggregated, community-level health data to shape responsive state and national programs. The insights from this research can inform policymakers, health departments, and non-profits to initiate anaemia control strategies tailored to the socio-cultural realities of the Mal Pahariya community.
Keywords:Anaemia; Tribal Health; Mal Pahariya; Haemoglobin; Jharkhand
Introduction
Globally, anaemia remains a major public health concern.
In 2021, an estimated 1.92 billion people—about one-fourth of
the world’s population-were anaemic, with women and children
disproportionately affected despite some declines among adult men
(GBD 2021, IHME, 2023). [1,2] In 2023, 30.7% of women aged 15-
49 years were anaemic, including 35.5% of pregnant women (WHO,
2025) [3].
Anaemia, particularly iron-deficiency anaemia, is one of India’s
most pressing public health challenges, disproportionately affecting
women, children, and marginalized groups. While national programs
like Anaemia Mukt Bharat aim to reduce anaemia, communities
such as the Particularly Vulnerable Tribal Groups (PVTGs) often
remain outside the reach of structured health services. A significant
data gap exists for these populations, limiting the design of effective,
community-tailored interventions (Sharma et al., 2020; Singh and
Roy, 2021) [4,5].
Jharkhand, a tribal-majority state, reports one of the highest
anaemia prevalence rates in the country. According to NFHS-5
(2020–21), over 65% of women and 67.5% of children under five in
the state are anaemic. The Mal Pahariya community, classified as a
PVTG, inhabits forested regions of Pakur, especially Littipara Block,
where systemic neglect, socio-economic marginalization, and poor
access to nutrition and healthcare services persist.
Field-level observations have long indicated poor nutritional
status among the Mal Pahariya. A frontline health worker from
Durio noted, “We’ve seen girls faint during school mid-day meals,
and pregnant women walking 4–5 km just to get water. But no one
really checks their blood.” These observations provided the impetus to
initiate systematic testing for anaemia in the region.
This study was conceptualized to address this knowledge gap through direct village-level testing of haemoglobin levels in Mal Pahariya-inhabited villages. By generating empirical evidence from the field, it seeks to provide a foundation for targeted health interventions, community nutrition planning, and inclusive policy formulation. The objectives of the study include:
a) To assess the prevalence of anaemia among residents of 8 tribal villages.
b) To analyse gender and age-wise trends in Haemoglobin levels.
c) To provide evidence-based recommendations for local health policy.
This study was conceptualized to address this knowledge gap through direct village-level testing of haemoglobin levels in Mal Pahariya-inhabited villages. By generating empirical evidence from the field, it seeks to provide a foundation for targeted health interventions, community nutrition planning, and inclusive policy formulation. The objectives of the study include:
a) To assess the prevalence of anaemia among residents of 8 tribal villages.
b) To analyse gender and age-wise trends in Haemoglobin levels.
c) To provide evidence-based recommendations for local health policy.
Methods
This study adopted a quantitative clinical research design to
assess the prevalence of anaemia among the Mal Pahariya community
inhabiting remote villages of Littipara Block, Pakur district, Jharkhand.
A total of 278 individuals from eight villages under Littipara and
Karmatarn panchayats participated in the study. The villages include
Makhnipahar, Keradoli, Jhapri, Kathalpara, Durio, Bada Pokhariya,
Chota Pokhariya, and Gadapahari. All participants were primarily
from the Mal Pahariya community, a Particularly Vulnerable Tribal
Group (PVTG). Selection was done through community mobilization
with the support of local changemakers and participation was
voluntary, based on informed consent.
Data was collected through field-based health camps conducted across eight villages under Littipara and Karmatarn panchayats between 26th May and 31st May 2025. Blood sample collection was carried out by trained phlebotomists from Dr. Lal Path Labs, following standard clinical procedures. Venous blood was drawn from each participant using sterile equipment and promptly transported under cold-chain conditions to a certified laboratory in Dumka for sameday Haemoglobin analysis. This approach ensured high accuracy and reliability of test results. No interviews, surveys, or focus group discussions were conducted to avoid response bias and to maintain an exclusive focus on clinical indicators, specifically Haemoglobin concentration, as the core parameter for assessing anaemia prevalence.
Data was collected through field-based health camps conducted across eight villages under Littipara and Karmatarn panchayats between 26th May and 31st May 2025. Blood sample collection was carried out by trained phlebotomists from Dr. Lal Path Labs, following standard clinical procedures. Venous blood was drawn from each participant using sterile equipment and promptly transported under cold-chain conditions to a certified laboratory in Dumka for sameday Haemoglobin analysis. This approach ensured high accuracy and reliability of test results. No interviews, surveys, or focus group discussions were conducted to avoid response bias and to maintain an exclusive focus on clinical indicators, specifically Haemoglobin concentration, as the core parameter for assessing anaemia prevalence.
Venous blood samples were collected using standardized
phlebotomy kits, including sterile vacutainers, disposable syringes,
and tourniquets, as per protocols followed by Dr. Lal Path Labs.
The collection process adhered to biomedical waste management
and aseptic techniques to ensure safety and accuracy. Samples were
labelled and maintained under cold-chain conditions before being
transported daily to a certified diagnostic laboratory in Dumka for
Haemoglobin analysis.
Haemoglobin levels were measured using automated hematology analyzers at the laboratory, providing precise and reliable results. Unlike portable devices such as HemoCue, which are commonly used in field settings, this approach ensured higher diagnostic accuracy and laboratory-grade testing consistency. All results were compiled and documented systematically based on village-wise participant lists, enabling easy disaggregation for data analysis. Informed consent was obtained from all participants prior to testing. Anonymity and confidentiality of participants were strictly maintained. Individuals found to be anaemic were advised to seek medical attention and were referred to nearby public health facilities. Ethical protocols were strictly followed throughout the study to ensure the dignity, rights, and confidentiality of all participants. For minors, consent was taken from parents or guardians. The study adhered to the ethical standards laid down by the Indian Council of Medical Research (ICMR) for community-based health assessments.
Data from laboratory reports were compiled village-wise and organized using Microsoft Excel for data entry, cleaning, and sorting. Each participant’s Haemoglobin level was categorized as normal or anaemia based on WHO thresholds (<13 g/dL for men, <12 g/ dL for women). The cleaned dataset was then analyzed using SPSS to generate descriptive statistics. The results offer baseline insights for public health planning in tribal communities. No inferential or multivariate statistical tests were applied, as the study’s primary goal was observational and diagnostic. The results offer baseline insights for Substantially higher than the public health planning in tribal communities.
Haemoglobin levels were measured using automated hematology analyzers at the laboratory, providing precise and reliable results. Unlike portable devices such as HemoCue, which are commonly used in field settings, this approach ensured higher diagnostic accuracy and laboratory-grade testing consistency. All results were compiled and documented systematically based on village-wise participant lists, enabling easy disaggregation for data analysis. Informed consent was obtained from all participants prior to testing. Anonymity and confidentiality of participants were strictly maintained. Individuals found to be anaemic were advised to seek medical attention and were referred to nearby public health facilities. Ethical protocols were strictly followed throughout the study to ensure the dignity, rights, and confidentiality of all participants. For minors, consent was taken from parents or guardians. The study adhered to the ethical standards laid down by the Indian Council of Medical Research (ICMR) for community-based health assessments.
Data from laboratory reports were compiled village-wise and organized using Microsoft Excel for data entry, cleaning, and sorting. Each participant’s Haemoglobin level was categorized as normal or anaemia based on WHO thresholds (<13 g/dL for men, <12 g/ dL for women). The cleaned dataset was then analyzed using SPSS to generate descriptive statistics. The results offer baseline insights for public health planning in tribal communities. No inferential or multivariate statistical tests were applied, as the study’s primary goal was observational and diagnostic. The results offer baseline insights for Substantially higher than the public health planning in tribal communities.
Limitation of the study
This study is limited by its cross-sectional design, which restricts
causal inference. The reliance solely on Haemoglobin testing, without
additional biomarkers such as serum ferritin or C-reactive protein
(CRP), constrains the ability to distinguish iron-deficiency anaemia
from anaemia of chronic disease. The absence of dietary recall,
morbidity histories, and socio-cultural context further narrows the
explanatory scope of findings. Additionally, the lack of qualitative
narratives beyond anecdotal accounts limits the understanding of lived
experiences and behavioural determinants. Future research should
adopt longitudinal and mixed-methods approaches, incorporating
dietary surveys, biomarker panels, and qualitative inquiry to generate
a more comprehensive picture of anaemia determinants in PVTG
populations.
Results
[Table 1] presents the gender-wise distribution of 278 blood
samples collected from eight villages under Littipara and Karmatarn

panchayats. Out of the total participants, 181 were female (65.1%) and
97 were male (34.9%). The significantly higher proportion of female
participants reflects two key dynamics: first, the study’s intentional
focus on assessing anaemia among women, given their increased
biological vulnerability and reproductive health needs; and second,
greater responsiveness of women to community health outreach
efforts, particularly in tribal contexts where men often migrate for
labor or are less engaged with routine health screenings.
This gender distribution is consistent with national and state level
priorities under programs like Anaemia Mukt Bharat, which
emphasize testing and treating anaemia among adolescent girls
and women of reproductive age. The higher female participation
also provides a robust dataset to evaluate gendered disparities in
Haemoglobin levels, which are explored in subsequent tables and
figures.
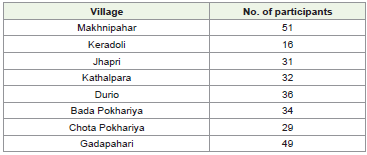
[Table 2] presents a comparative view of the number of blood samples collected across eight villages. Makhnipahar (51 samples) and Gadpahari (49 samples) recorded the highest participation, likely due to better mobilization and community interest and consent. In contrast, Keradoli (16 samples) had the lowest, possibly reflecting challenges like lack of awareness and interest. The relatively balanced distribution across villages suggests effective field mobilization. This village-wise breakdown is essential for planning targeted health interventions and understanding the geographic spread of anaemia in the Mal Pahariya community of Littipara Block, ensuring no location is overlooked.
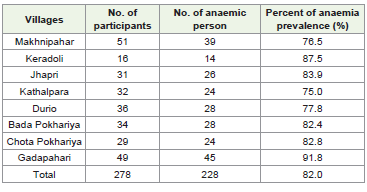
[Table 3] reveals a consistently high prevalence of anaemia across all eight villages surveyed. Gadapahari (91.8%) and Keratoli (87.5%) reported the highest number of anaemic individuals, reflecting a critical nutritional burden. Villages like Kathalpara (75%) and Makhnipahar (76.5%) also indicate a severe public health concern, with minimal normal cases. Even in smaller sample villages like Keradoli, anaemia remains dominant (14 out of 16). The uniformly high anaemic counts suggest that anaemia is widespread and systemic across the region, rather than isolated to specific pockets. This calls for comprehensive, village-level interventions to address dietary gaps and strengthen rural health outreach.
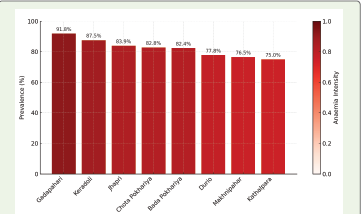
As depicted in (Figure 1), the prevalence of anaemia is acute in all villages. Gadapahari, Keratoli and Jhapri shows prevalence of anaemia among 83 to 90 percent of tested individuals. Lowest prevalence is depicted in Chota Pokhariya and Bada Pokhariya which is again more than 59%.
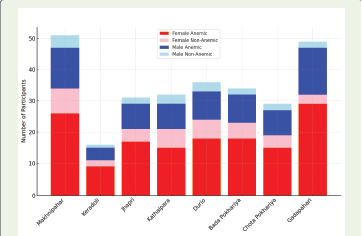
[Figure 2] presents a village-wise comparison of anaemia prevalence by gender. The stacked bar chart highlights that, across all surveyed villages, women consistently show a disproportionately higher burden of anaemia compared to men. This reinforces the systemic and gendered nature of anaemia in the Mal Pahariya community, complementing the overall prevalence patterns shown in [Table 3] .
[Table 2] presents a comparative view of the number of blood samples collected across eight villages. Makhnipahar (51 samples) and Gadpahari (49 samples) recorded the highest participation, likely due to better mobilization and community interest and consent. In contrast, Keradoli (16 samples) had the lowest, possibly reflecting challenges like lack of awareness and interest. The relatively balanced distribution across villages suggests effective field mobilization. This village-wise breakdown is essential for planning targeted health interventions and understanding the geographic spread of anaemia in the Mal Pahariya community of Littipara Block, ensuring no location is overlooked.
[Table 3] reveals a consistently high prevalence of anaemia across all eight villages surveyed. Gadapahari (91.8%) and Keratoli (87.5%) reported the highest number of anaemic individuals, reflecting a critical nutritional burden. Villages like Kathalpara (75%) and Makhnipahar (76.5%) also indicate a severe public health concern, with minimal normal cases. Even in smaller sample villages like Keradoli, anaemia remains dominant (14 out of 16). The uniformly high anaemic counts suggest that anaemia is widespread and systemic across the region, rather than isolated to specific pockets. This calls for comprehensive, village-level interventions to address dietary gaps and strengthen rural health outreach.
As depicted in (Figure 1), the prevalence of anaemia is acute in all villages. Gadapahari, Keratoli and Jhapri shows prevalence of anaemia among 83 to 90 percent of tested individuals. Lowest prevalence is depicted in Chota Pokhariya and Bada Pokhariya which is again more than 59%.
[Figure 2] presents a village-wise comparison of anaemia prevalence by gender. The stacked bar chart highlights that, across all surveyed villages, women consistently show a disproportionately higher burden of anaemia compared to men. This reinforces the systemic and gendered nature of anaemia in the Mal Pahariya community, complementing the overall prevalence patterns shown in [Table 3] .
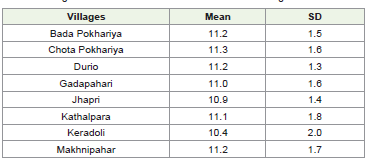
[Table 4] depicts the mean Haemoglobin levels across the villages
range from 10.4 g/dL to 11.3 g/dL, indicating relatively modest
variation among villages. Chota Pokhariya recorded the highest
mean Haemoglobin level at 11.3 g/dL, closely followed by Bada
Pokhariya, Durio, and Makhnipahar, each with 11.2 g/dL. Keradoli
had the lowest mean Haemoglobin level, at 10.4 g/dL and the highest
variability (SD = 2.0), suggesting a potential concern for anaemia or
lower nutritional/health standards in that area.
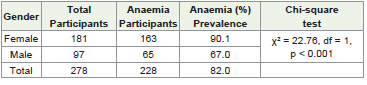
[Table 5] reveals a disturbingly high prevalence of anaemia among both female and male participants. Out of 181 female participants, 163 (90.1%) were found to be anaemic. Among 97 male participants, 65 (67%) were anaemic. These figures significantly exceed national averages. The chi-square test indicates a statistically significant association between gender and anaemia prevalence, with females showing a higher prevalence than males.
[Table 6] show that the mean haemoglobin level for males is 12.3 g/dL (SD ±1.5), while for females it is 10.5 g/dL (SD ±1.3). The mean haemoglobin level for males (12.3 g/dL) is below the WHO threshold (13 g/dL), indicating that on average, males in the study population are anaemia. The mean Haemoglobin level for females (10.5 g/dL) is also below the WHO threshold (12 g/dL for non-pregnant and 11 g/ dL for pregnant women), suggesting widespread anaemia among women, regardless of pregnancy status (WHO, 2011).
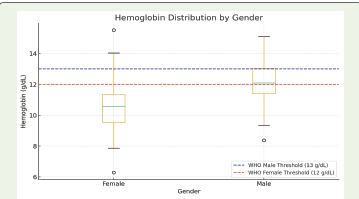
[Figure 3] presents a boxplot of Haemoglobin distribution by gender. The visualization highlights that women’s Haemoglobin levels are consistently lower, with the interquartile range falling below the WHO threshold (12 g/dL). In contrast, men’s distribution shows slightly higher values but still includes a significant proportion below the 13 g/dL cut-off. This graphical evidence reinforces the gender gap observed in anaemia prevalence.
[Table 5] reveals a disturbingly high prevalence of anaemia among both female and male participants. Out of 181 female participants, 163 (90.1%) were found to be anaemic. Among 97 male participants, 65 (67%) were anaemic. These figures significantly exceed national averages. The chi-square test indicates a statistically significant association between gender and anaemia prevalence, with females showing a higher prevalence than males.
[Table 6] show that the mean haemoglobin level for males is 12.3 g/dL (SD ±1.5), while for females it is 10.5 g/dL (SD ±1.3). The mean haemoglobin level for males (12.3 g/dL) is below the WHO threshold (13 g/dL), indicating that on average, males in the study population are anaemia. The mean Haemoglobin level for females (10.5 g/dL) is also below the WHO threshold (12 g/dL for non-pregnant and 11 g/ dL for pregnant women), suggesting widespread anaemia among women, regardless of pregnancy status (WHO, 2011).
[Figure 3] presents a boxplot of Haemoglobin distribution by gender. The visualization highlights that women’s Haemoglobin levels are consistently lower, with the interquartile range falling below the WHO threshold (12 g/dL). In contrast, men’s distribution shows slightly higher values but still includes a significant proportion below the 13 g/dL cut-off. This graphical evidence reinforces the gender gap observed in anaemia prevalence.
The cumulative distribution functions (CDFs) of Haemoglobin
levels are shown [Figure 4] for male (n=97) and female (n=181)
participants from the Mal Pahariya community in Littipara Block,
Jharkhand. Vertical dashed lines represent WHO thresholds for
anaemia: 13 g/dL for men and 12 g/dL for women. The curve shift
illustrates that the majority of women fall below the anaemia
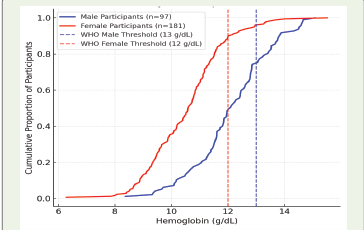
threshold, while a substantial proportion of men also remain under
their cut-off.
Anaemia, particularly iron-deficiency anaemia, is one of India’s most pressing public health challenges, disproportionately affecting women, children, and marginalized groups. According to NFHS- 5 (2020–21), over 65% of women and 67.5% of children under five in Jharkhand are anaemic. While national programs like Anaemia Mukt Bharat aim to reduce anaemia, communities such as the Particularly Vulnerable Tribal Groups (PVTGs) often remain outside the reach of structured health services. A significant lack of localized evidence exists for these populations, limiting the design of effective, community-tailored interventions (Sharma et al., 2020; Singh and Roy, 2021) [4,5]. However, the significantly high anaemia prevalence in males also signals broader dietary deficiencies and chronic undernutrition in the community — an issue often overlooked in anaemia-related health programming.
These findings underscore the need for gender-inclusive anaemia control strategies, especially for PVTG communities like the Mal Pahariya, where structural marginalization exacerbates health inequalities for both sexes.
A greater proportion of females are anaemia compared to males; highlights gender-based nutritional disparities. When analyzed by village, the chart reveals varying anaemia burdens, with some villages like Makhnipahar and Gadpahari showing a higher absolute number of anaemic individuals. This layered visual enables clear identification of both high-burden groups and better-performing pockets, helping policymakers and field teams prioritize villages and design targeted interventions for anaemia control within the Mal Pahariya community
Anaemia, particularly iron-deficiency anaemia, is one of India’s most pressing public health challenges, disproportionately affecting women, children, and marginalized groups. According to NFHS- 5 (2020–21), over 65% of women and 67.5% of children under five in Jharkhand are anaemic. While national programs like Anaemia Mukt Bharat aim to reduce anaemia, communities such as the Particularly Vulnerable Tribal Groups (PVTGs) often remain outside the reach of structured health services. A significant lack of localized evidence exists for these populations, limiting the design of effective, community-tailored interventions (Sharma et al., 2020; Singh and Roy, 2021) [4,5]. However, the significantly high anaemia prevalence in males also signals broader dietary deficiencies and chronic undernutrition in the community — an issue often overlooked in anaemia-related health programming.
These findings underscore the need for gender-inclusive anaemia control strategies, especially for PVTG communities like the Mal Pahariya, where structural marginalization exacerbates health inequalities for both sexes.
A greater proportion of females are anaemia compared to males; highlights gender-based nutritional disparities. When analyzed by village, the chart reveals varying anaemia burdens, with some villages like Makhnipahar and Gadpahari showing a higher absolute number of anaemic individuals. This layered visual enables clear identification of both high-burden groups and better-performing pockets, helping policymakers and field teams prioritize villages and design targeted interventions for anaemia control within the Mal Pahariya community
Discussion
With an overall anaemia prevalence of 82%, the data not only
surpasses state (Jharkhand: ~65%) and national (India: ~57%)
averages reported in NFHS-5 (2020–21), but also confirms the gravity
of iron-deficiency anaemia among Particularly Vulnerable Tribal
Groups (PVTGs). The disproportionate burden on women, 90.1%
of whom were found to be anaemic, significantly exceeds global
estimates, where WHO (2023) reported 30.7% of women aged 15-
49 years and 35.5% of pregnant women as anaemic. This striking
disparity reinforces previous scholarship that links anaemia with
gender-based nutritional inequality, reproductive health burdens, and
limited access to antenatal care and dietary supplements. (Sharma et
al., 2020; ICMR-NIN, 2018) [4,6].
The substantial anaemia prevalence among men (67.0%) is
particularly striking, as anaemia in adult males is often underreported
and underdiagnosed. This suggests a more systemic nutritional
deprivation that affects the entire community, regardless of gender, and
raises concerns around chronic food insecurity, low dietary diversity,
and insufficient protein and iron intake. This finding challenges
the conventional narrative that primarily associates anaemia with
women and children and points toward a broader ecological issue
of malnutrition within PVTG households. These localised deficits
resonate with global patterns, where an estimated 4 billion people
consume diets lacking adequate levels of key micronutrients such as
iron (65%) and folate (54%) (Global Micronutrient Report, 2024). The
Mal Pahariya prevalence therefore reflects not only a communityspecific
crisis but also contributes to the wider discourse on the global
nutrition gap.
“As one woman from Jhapri village shared during the camp, ‘We eat what we grow. Most days it’s rice and salt, and pulses or vegetables only when the monsoon comes. I often feel dizzy while working in the fields, but I thought it was just tiredness.’ Her account reflects the chronic dietary insufficiencies that dominate everyday life and likely contribute to the striking 90.1% anaemia prevalence among women in this study.” Similarly, a young man from Gadapahari remarked, ‘I go out for work most days, but I feel weak very often. Even if I eat more rice, it doesn’t give strength.’ Such lived experiences highlight that anaemia is not only a women’s health issue, but a systemic nutritional crisis affecting the entire community.”
The present findings reveal that the mean Haemoglobin levels among both males (12.3 g/dL) and females (10.5 g/dL) are below the WHO-defined cut-off values for normal Haemoglobin concentration. According to WHO, Haemoglobin levels <13.0 g/dL in men and <12.0 g/dL in non-pregnant women (or <11.0 g/dL in pregnant women) are indicative of anaemia. This clearly establishes that anaemia is prevalent in both genders within the study population, with women showing a comparatively greater deficit.
“As one woman from Jhapri village shared during the camp, ‘We eat what we grow. Most days it’s rice and salt, and pulses or vegetables only when the monsoon comes. I often feel dizzy while working in the fields, but I thought it was just tiredness.’ Her account reflects the chronic dietary insufficiencies that dominate everyday life and likely contribute to the striking 90.1% anaemia prevalence among women in this study.” Similarly, a young man from Gadapahari remarked, ‘I go out for work most days, but I feel weak very often. Even if I eat more rice, it doesn’t give strength.’ Such lived experiences highlight that anaemia is not only a women’s health issue, but a systemic nutritional crisis affecting the entire community.”
The present findings reveal that the mean Haemoglobin levels among both males (12.3 g/dL) and females (10.5 g/dL) are below the WHO-defined cut-off values for normal Haemoglobin concentration. According to WHO, Haemoglobin levels <13.0 g/dL in men and <12.0 g/dL in non-pregnant women (or <11.0 g/dL in pregnant women) are indicative of anaemia. This clearly establishes that anaemia is prevalent in both genders within the study population, with women showing a comparatively greater deficit.
When compared with WHO standards for the public health
significance of anaemia, the mean values from this study strongly
suggest that anaemia constitutes a severe public health problem in this
population. This calls for urgent interventions, including improved
dietary practices, supplementation programs, deworming initiatives,
and awareness campaigns aimed at addressing the underlying causes.
Geographical analysis revealed that anaemia prevalence is not
isolated to specific villages but consistently high across all eight
surveyed locations, ranging from 75% to 91.8%. The highest burden
was observed in Gadapahari (91.8%), followed by Keradoli (87.5%)
and Jhapri (83.9%). This uniformity across locations underscores
the systemic nature of the problem, likely exacerbated by shared
socio-economic disadvantages, poor healthcare infrastructure, and
geographic inaccessibility. Despite national-level programs such
as Anaemia Mukt Bharat and tribal health interventions, the nearabsence
of preventive or curative engagement in these villages points
to a failure in last-mile service delivery for PVTGs.
The gender distribution of participants, heavily skewed towards
women (65.1%), also sheds light on community health dynamics.
Women’s higher participation may indicate both their increased
vulnerability and their greater engagement with health initiatives.
However, this also raises questions about male invisibility in healthseeking
behavior, particularly in tribal contexts where male migration
is common and health education campaigns often overlook adult
men.
The use of venous blood sampling analyzed through certified
laboratory techniques ensures robust clinical accuracy, surpassing
the reliability of field-based tools like HemoCue. This methodological
rigor enhances the credibility of findings and highlights the value
of high-quality diagnostic practices, especially in under-researched
populations. However, the absence of qualitative data such as
dietary recall, morbidity history, or socio-cultural barriers limits the
study’s ability to contextualize findings within lived experiences of
participants.
Nonetheless, the results provide critical baseline data and a
clear call to action for public health authorities, local governance
structures, and development practitioners working with PVTGs in
Jharkhand. This local call to action resonates with global advocacy
momentum. The renewed focus at the Nutrition for Growth Summit
2025 explicitly called for bold political and financial commitments to
accelerate anaemia reduction. Positioning the Mal Pahariya evidence
within this policy dialogue highlights how local baseline data can
strengthen national anaemia control programmes and align India’s
commitments with global nutrition targets.
Conclusion
This study highlights the urgent and widespread public health
challenge of anaemia within the Mal Pahariya community, a Particularly
Vulnerable Tribal Group residing in remote villages of Pakur district.
With 82% of the sampled population identified as anaemic, this points
to chronic undernutrition—especially among women (90.1%) and
men (67%) — the findings signal a crisis that demands immediate,
targeted, and culturally appropriate interventions. Such widespread
anaemia reflects not only gender-based nutritional disparities but
also systemic dietary gaps. Globally, over 4 billion people consume
inadequate iron (65%), folate (54%), and other micronutrients, with
women disproportionately affected in iron, iodine, and vitamin B12
(Global Micronutrient Report, 2024).
Despite decades of national anaemia control programs, communities like the Mal Pahariya remain largely excluded from structured health services due to geographic isolation, systemic neglect, and social marginalization. The uniformly high anaemia prevalence across villages confirms that the issue is not anecdotal or isolated, but deeply embedded in the daily realities of these populations.
Despite decades of national anaemia control programs, communities like the Mal Pahariya remain largely excluded from structured health services due to geographic isolation, systemic neglect, and social marginalization. The uniformly high anaemia prevalence across villages confirms that the issue is not anecdotal or isolated, but deeply embedded in the daily realities of these populations.
The study serves as a wake-up call for policymakers, indicating
the need for:
Tailored community nutrition programs should include dietary diversification, promotion of traditional ironrich foods, and culturally rooted behaviour change communication.
Strengthened outreach by frontline health workers, specifically trained to address the needs of PVTGs;
Gender-inclusive interventions that target not just adolescent girls and pregnant women, but also adult men and boys who remain invisible in current anaemia discourse;
Decentralized data systems that capture health indicators from marginalized communities, enabling real-time monitoring and responsive governance.
In closing, this research provides foundational evidence for inclusive health planning and underscores the ethical imperative of reaching India’s most vulnerable citizens with the care and attention they deserve. The findings resonate with the global urgency to address anaemia, as reflected in the renewed advocacy at the Nutrition for Growth Summit 2025, which called for bold financial and policy commitments.
Tailored community nutrition programs should include dietary diversification, promotion of traditional ironrich foods, and culturally rooted behaviour change communication.
Strengthened outreach by frontline health workers, specifically trained to address the needs of PVTGs;
Gender-inclusive interventions that target not just adolescent girls and pregnant women, but also adult men and boys who remain invisible in current anaemia discourse;
Decentralized data systems that capture health indicators from marginalized communities, enabling real-time monitoring and responsive governance.
In closing, this research provides foundational evidence for inclusive health planning and underscores the ethical imperative of reaching India’s most vulnerable citizens with the care and attention they deserve. The findings resonate with the global urgency to address anaemia, as reflected in the renewed advocacy at the Nutrition for Growth Summit 2025, which called for bold financial and policy commitments.
Acknowledgement
First and foremost, we extend our deepest gratitude to the Mal
Pahariya community of Littipara and Karmatarn panchayats for
their trust, cooperation, and willingness to participate in this study.
Their openness and engagement made this research meaningful.
We sincerely acknowledge the efforts of our field team, who worked
tirelessly to mobilize participants and secure community consensus
through Gram Sabha meetings, ensuring ethical and respectful data
collection.
We are thankful to Sarva Seva Samity Sanstha (4S India) for
entrusting us with this opportunity and supporting grassroots health
research. We extend our heartfelt regards to Mr. Shwetank Mishra,
whose encouragement and guidance were instrumental at every step
of this journey, and to the Paul Hamlyn Foundation (PHF) team for
their meaningful and sustained support. We also thank Mr. Mihir
Sahana, ED of 4S India, for providing us an opportunity to work
with the ultra-poor community at Santhal Parganas and Mr. Kumar
Gaurav, Dy. Director, for his thoughtful guidance throughout the
process.
References
Citation
Chakraborty D, Kar SC, Sengupta M. Anaemia in Marginalized Communities: Evidence from the Mal Pahariya PVTG in Littipara Block, Jharkhand. Indian J Nutri. 2026;13(1): 342.