Research Article
Nutritional Status of School Going Children (6-9 Years Old) In the Western Suburban Slums of Mumbai
Abhipsha Gupta* and Reema Mathur
Department of Food Science and Nutrition, SNDT Women’s University, Juhu Campus, Mumbai, Maharashtra India
*Corresponding author:Abhipsha Gupta, Department of Food Science and Nutrition, SNDT Women’s University, Juhu Campus, Mumbai, Maharashtra India. E-mail Id:abhipshagupta99@gmail.com
Article Information:Submission: 08/04/2026; Accepted: 21/04/2026; Published: 24/04/2026
Copyright: © 2026 Abhipsha Gupta, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Adequate nutrition during the early school years (6–9 years) is fundamental for supporting optimal growth, cognitive development and academic performance. Children living in urban slums are particularly vulnerable to nutritional deficiencies due to poverty, food insecurity and poor environmental conditions, which may adversely affect their overall health and learning potential. Considering the importance of nutrition for this age group, this study was undertaken to evaluate the nutritional status and dietary intake of school-going children residing in the western suburban slums of Mumbai.
Methods: A cross-sectional study was conducted in the western suburban slums of Mumbai with the aim to assess the malnutrition and dietary status of school going children of 6 to 9 years of age. Data was collected by visiting anganwadi centres to meet the participants or by visiting their houses. Demographic information was collected using a questionnaire and nutritional status was assessed through anthropometric measurements, dietary intake using 24 hour recall and food frequency and medical issues. Descriptive statistics was used and correlations estimated at p<0.05 level of significance.
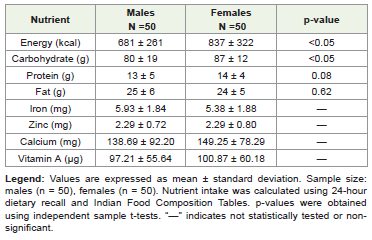
Results: According to BAZ (Body Mass Index for age- Z scores), 39% children were severely underweight and 14% underweight; 37% were stunted (HAZ- Height for Age Z scores) and 35% were thin (MUAC-Mid Upper Arm Circumference). The mean intake of energy for males was 681±261 kcal and 837±322 kcal for females, carbohydrate intake was 80±19 g and 87±12 g, protein intake was 13±5 g and 14±4 g and for fat, intakes was 25±6 g and 24±5 g for males and females respectively. These were all much lower than the EAR values. Iron and zinc intakes were similar in both sexes whereas calcium and vitamin A were only slightly higher in females. Significant differences were observed in the nutrient intakes of the children in the HAZ – Height-for-Age Z-score; MUAC – Mid-Upper Arm Circumference, and BMI –categories with the malnourished having a lower intake.
Conclusions: The school children in this study were malnourished and had nutrient intakes lower than the values recommended by ICMR for this age group.
Methods: A cross-sectional study was conducted in the western suburban slums of Mumbai with the aim to assess the malnutrition and dietary status of school going children of 6 to 9 years of age. Data was collected by visiting anganwadi centres to meet the participants or by visiting their houses. Demographic information was collected using a questionnaire and nutritional status was assessed through anthropometric measurements, dietary intake using 24 hour recall and food frequency and medical issues. Descriptive statistics was used and correlations estimated at p<0.05 level of significance.
Results: According to BAZ (Body Mass Index for age- Z scores), 39% children were severely underweight and 14% underweight; 37% were stunted (HAZ- Height for Age Z scores) and 35% were thin (MUAC-Mid Upper Arm Circumference). The mean intake of energy for males was 681±261 kcal and 837±322 kcal for females, carbohydrate intake was 80±19 g and 87±12 g, protein intake was 13±5 g and 14±4 g and for fat, intakes was 25±6 g and 24±5 g for males and females respectively. These were all much lower than the EAR values. Iron and zinc intakes were similar in both sexes whereas calcium and vitamin A were only slightly higher in females. Significant differences were observed in the nutrient intakes of the children in the HAZ – Height-for-Age Z-score; MUAC – Mid-Upper Arm Circumference, and BMI –categories with the malnourished having a lower intake.
Conclusions: The school children in this study were malnourished and had nutrient intakes lower than the values recommended by ICMR for this age group.
Keywords:School Children; Malnutrition;Dietary Intake; Anthropometry; Urban Slums; India
Introduction
School-age children represent the foundation of a nation’s future
health and productivity. Adequate nutrition during middle childhood
is essential for optimal physical growth, cognitive development and
academic performance. Nutritional deprivation during this critical
period can adversely affect learning ability, immunity and longterm
health outcomes. Globally, children face a “double burden of
malnutrition,” characterised by the coexistence of undernutrition
and emerging overweight, which has become a significant public
health concern in both developing and developed countries [1].
Childhood and early adolescence are marked by rapid growth and increased nutrient requirements. Inadequate dietary intake during this stage may lead to growth faltering, reduced school attendance and poor scholastic performance [2]. Despite the importance of this age group, school children aged 5-9 years are often underrepresented in national nutrition surveillance systems, which primarily focus on children under five years of age. Consequently, data on the nutritional status of primary school-age children, particularly those living in disadvantaged communities, remain limited.
Children residing in urban slums are especially vulnerable due to overcrowding, poor sanitation, unsafe drinking water, food insecurity and limited access to healthcare services. Such conditions predispose them to recurrent infections, inadequate dietary practices and increased risk of malnutrition [3]. Similar findings have been reported among school-age children living in disadvantaged urban settlements, where a high prevalence of undernutrition and growth deficits has been documented [4].
Studies from resource-limited communities have further demonstrated substantial levels of stunting, thinness and poor anthropometric indicators among school-going children, highlighting the persistent burden of nutritional inadequacy in this age group [5]. School health surveys conducted in Indian states have similarly documented substantial levels of undernutrition and growth faltering among primary school children, emphasizing the continuing burden of malnutrition beyond the under-five age group [6]. Although national surveys such as the National Family Health Survey document undernutrition among under-five children, evidence for school-age children in slum settings remains scarce.
In this context, the present study was undertaken with the objective to assess the nutritional status and dietary intake of schoolgoing children aged 6-9 years residing in a slum area of Mumbai. The study also examined selected socio-economic characteristics and the presence of common morbidities to better understand factors associated with malnutrition in this vulnerable population.
Childhood and early adolescence are marked by rapid growth and increased nutrient requirements. Inadequate dietary intake during this stage may lead to growth faltering, reduced school attendance and poor scholastic performance [2]. Despite the importance of this age group, school children aged 5-9 years are often underrepresented in national nutrition surveillance systems, which primarily focus on children under five years of age. Consequently, data on the nutritional status of primary school-age children, particularly those living in disadvantaged communities, remain limited.
Children residing in urban slums are especially vulnerable due to overcrowding, poor sanitation, unsafe drinking water, food insecurity and limited access to healthcare services. Such conditions predispose them to recurrent infections, inadequate dietary practices and increased risk of malnutrition [3]. Similar findings have been reported among school-age children living in disadvantaged urban settlements, where a high prevalence of undernutrition and growth deficits has been documented [4].
Studies from resource-limited communities have further demonstrated substantial levels of stunting, thinness and poor anthropometric indicators among school-going children, highlighting the persistent burden of nutritional inadequacy in this age group [5]. School health surveys conducted in Indian states have similarly documented substantial levels of undernutrition and growth faltering among primary school children, emphasizing the continuing burden of malnutrition beyond the under-five age group [6]. Although national surveys such as the National Family Health Survey document undernutrition among under-five children, evidence for school-age children in slum settings remains scarce.
In this context, the present study was undertaken with the objective to assess the nutritional status and dietary intake of schoolgoing children aged 6-9 years residing in a slum area of Mumbai. The study also examined selected socio-economic characteristics and the presence of common morbidities to better understand factors associated with malnutrition in this vulnerable population.
Materials and Methods
Study design and setting:
A community-based cross-sectional study was conducted in the
western suburban slums of Mumbai to assess the nutritional status
and dietary intake of school-going children aged 6-9 years.Ethical approval:
The study protocol was reviewed and approved by the Inter
System Biomedica Ethics Committee (ISBEC), Mumbai. Written
informed consent was obtained from parents or guardians prior to
enrolment.Participants:
Both male and female school-going children aged 6-9 years
residing in the selected slum areas were eligible for inclusion. Children
with intellectual disability, congenital abnormalities or known genetic
disorders were excluded to avoid confounding of growth assessment.
A total of 110 children were initially approached; however, complete
data were available for 100 participants, comprising 50 boys and 50
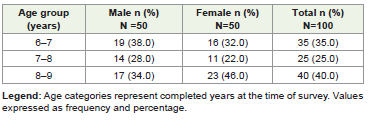
girls. The mean age of the study population was 7.17 ± 1.4 years.Data Collection:
Non-random purposive sampling was used. Slum was selected
based on convenience and all available children in the age-group were
approached in Anganwadi or by home visit. Five anganwadis were
covered. Sociodemographic details were collected from parents or
caregivers using a pretested structured questionnaire. Anthropometric
measurements including height, weight, body mass index (BMI),
mid-upper arm circumference (MUAC) and waist circumference
(WC) were recorded following standardized procedures based on
the NHANES 2007 anthropometry manual [7]. Height was measured
using a non-stretchable measuring tape with the child standing
erect without footwear, and weight was measured using a calibrated
weighing scale with light clothing. BMI was calculated as weight (kg)/
height (m²). Nutritional status was classified using Indian Academy
of Pediatrics (IAP) growth references and Khadilkar centile charts
for BMI-for-age (2007, 2015), MUAC-for-age (2021) and waist
circumference (2014) [8,9,10]. MUAC was measured on the left
arm using a non-elastic measuring tape and recorded to the nearest
0.1 cm, ensuring appropriate tension. Medical history and health related
information were also obtained, including past and present
illnesses, immunisation status, history of chronic conditions, age of
weaning, participation in supplementation or feeding programmes,
and utilisation of anganwadi services.Dietary assessment:
Dietary intake assessment was conducted using standardized
food frequency and 24-hour recall approaches consistent with
recommended dietary assessment methodologies for low-resource
settings [11]. Portion sizes were estimated using household measures,
and nutrient intake was computed using Indian food composition
tables following FAO dietary assessment guidelines. Nutrient intake
was computed using the Indian Food Composition Tables (IFCT,
2017). Intakes were compared with age-appropriate Estimated
Average Requirements [5].Statistical analysis:
Data were entered and analysed using SPSS software. Continuous
variables were expressed as mean ± standard deviation, and
categorical variables as frequency and percentage. Chi-square test,
independent t-test and analysis of variance (ANOVA) were applied
to assess differences between groups. A p-value <0.05 was considered
statistically significant.Results
A total of 100 children (50 boys and 50 girls) with a mean age
of 7.17 ± 1.40 years were included [Table 1]. Five children were not
enrolled in formal schooling, most attended government schools
(96.8%) or anganwadi centres (3.2%). The majority of respondents
were mothers (88%) and for rest, the fathers responded. Most
participants belonged to low-income families, with only 5% earning
more than Rs. 30,000/month and to joint-family households (73%);
16% lacked personal sanitation or water connections, and only onequarter
utilised ration support.
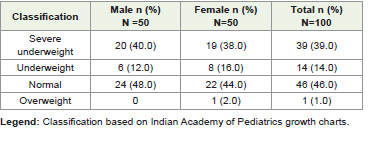
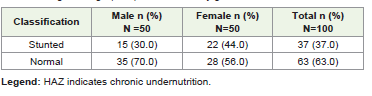
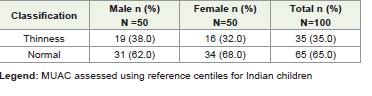
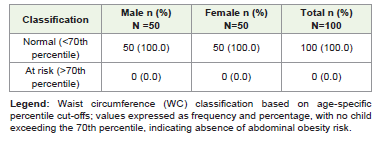
Mean anthropometric measurements showed that the overall mean weight was 15.9 ± 3.2 kg, with boys weighing more (16.5 ± 3.5 kg) than girls (15.2 ± 2.8 kg). The mean height was 112.23 ± 9.90 cm, with boys being taller (114.59 ± 10.31 cm) compared to girls (109.88 ± 8.97 cm). Mean BMI was comparable between sexes (boys: 12.50 ± 1.58 kg/m²; girls: 12.57 ± 1.53 kg/m²; overall: 12.53 ± 1.55 kg/m²). The overall meal waist circumference was 48.29 ± 5.95 cm, which was higher among boys (49.60 ± 5.03 cm) than girls (46.99 ± 6.55 cm). MUAC values were similar in both sexes (boys: 16.75 ± 1.88 cm; girls: 16.88 ± 1.64 cm; overall: 16.81 ± 1.76 cm). BMI-for-age classification showed 39% severe underweight and 14% underweight, with 46% normal and 1% overweight [Table 2]. Stunting was observed in 37% [Table 3], while thinness based on MUAC-for-age (<25th percentile cut-off) was present in 35% of children [Table 4]. None of the participants had waist circumference values above the 70th percentile, indicating absence of abdominal obesity and low risk of over-nutrition [Table 5]. Anaemia was the most prevalent morbidity, affecting 34% of the
Mean anthropometric measurements showed that the overall mean weight was 15.9 ± 3.2 kg, with boys weighing more (16.5 ± 3.5 kg) than girls (15.2 ± 2.8 kg). The mean height was 112.23 ± 9.90 cm, with boys being taller (114.59 ± 10.31 cm) compared to girls (109.88 ± 8.97 cm). Mean BMI was comparable between sexes (boys: 12.50 ± 1.58 kg/m²; girls: 12.57 ± 1.53 kg/m²; overall: 12.53 ± 1.55 kg/m²). The overall meal waist circumference was 48.29 ± 5.95 cm, which was higher among boys (49.60 ± 5.03 cm) than girls (46.99 ± 6.55 cm). MUAC values were similar in both sexes (boys: 16.75 ± 1.88 cm; girls: 16.88 ± 1.64 cm; overall: 16.81 ± 1.76 cm). BMI-for-age classification showed 39% severe underweight and 14% underweight, with 46% normal and 1% overweight [Table 2]. Stunting was observed in 37% [Table 3], while thinness based on MUAC-for-age (<25th percentile cut-off) was present in 35% of children [Table 4]. None of the participants had waist circumference values above the 70th percentile, indicating absence of abdominal obesity and low risk of over-nutrition [Table 5]. Anaemia was the most prevalent morbidity, affecting 34% of the
children, with a markedly higher prevalence among females (60%)
compared to males (8%). Dental caries were observed in 28% of
participants and were slightly more common among males (32%)
than females (24%). Ear, nose and throat problems were reported in
14% of children, with marginally higher occurrence among females
(16%) than males (12%). A few isolated conditions were also noted,
including skin diseases among three females and other illnesses
such as dengue in one male. Nearly half of the participants reported
the presence of chronic disorders, including chronic diarrhoea,
asthma, type I diabetes and cystic fibrosis, with no substantial gender
differences.
All children were fully immunised according to age-appropriate
schedules and were reportedly weaned at six months of age. None
of the participants were receiving nutritional supplementation
through government programmes; however, most attended school
or anganwadi feeding services. Dietary patterns were assessed using
a qualitative food frequency questionnaire along with a 24-hour
dietary recall. Meals were predominantly home-cooked and largely
non-vegetarian, with rice forming the staple cereal consumed daily
by most children. Pulses such as bengal gram, green gram and
lentils were generally consumed weekly or occasionally, while only
a few vegetables were eaten daily. Fruit intake was infrequent, and
regular consumption of milk and milk products was limited. Eggs and
chicken were typically consumed twice weekly, whereas meat and fish
intake was mostly weekly or occasional. Most children consumed
only two meals per day, reflecting low dietary diversity, and outside
or processed foods were consumed infrequently due to economic
constraints.
Energy, protein and carbohydrate intakes were comparatively
higher among females than males, while fat intake remained similar
between both sexes. Iron and zinc intakes were comparable, whereas
calcium and vitamin A intake was slightly higher among females
[Table 6]. Despite similar iron consumption, a greater prevalence
of anaemia was observed among girls, which may be attributed to
poor sanitation, recurrent infections such as diarrhoea, and overall
poor diet quality. Additionally, the high burden of underweight and
stunting may have contributed to this trend, consistent with findings
reported previously [3].
Comparison of nutrient intake with Estimated Average
Requirements (EAR) showed that none of the children met
the recommended dietary levels. Mean macronutrient intakes
generally ranged between approximately 50-80% of the EAR, while
micronutrient intakes were more inadequate, largely below 70% of
requirements. Stunted children demonstrated poorer intake, with
both macro- and micronutrients often falling below 50-60% of the
EAR. Although underweight children showed relatively higher
macronutrient intake approaching 70–80% of the EAR, this may
reflect the smaller sample size rather than true adequacy. Children
with normal MUAC-for-age had comparatively better intakes than
those with thinness, yet overall consumption across all anthropometric
categories remained insufficient to meet recommended requirements,
indicating widespread dietary inadequacy.
Lower macronutrient intake observed among children with thinness supports previous evidence that inadequate energy and protein consumption increases the risk of moderate and severe thinness in school-aged children [6]. Children with normal MUAC had significantly higher intakes of energy (p < 0.05) and carbohydrate (p < 0.05), whereas differences in protein (p = 0.08) and fat (p = 0.62) intake were not statistically significant. Similarly, micronutrient intakes including iron, zinc, calcium, and vitamin A showed no significant differences between groups. Comparable trends were observed for height-for-age (HAZ) and BMI-for-age (BAZ), where children with normal growth status consumed relatively greater macronutrients, while stunted and underweight children consistently demonstrated lower intakes. Overall, inadequate macronutrient consumption was associated with poorer anthropometric outcomes, reflecting both acute (MUAC) and chronic (HAZ and BAZ) undernutrition.
Lower macronutrient intake observed among children with thinness supports previous evidence that inadequate energy and protein consumption increases the risk of moderate and severe thinness in school-aged children [6]. Children with normal MUAC had significantly higher intakes of energy (p < 0.05) and carbohydrate (p < 0.05), whereas differences in protein (p = 0.08) and fat (p = 0.62) intake were not statistically significant. Similarly, micronutrient intakes including iron, zinc, calcium, and vitamin A showed no significant differences between groups. Comparable trends were observed for height-for-age (HAZ) and BMI-for-age (BAZ), where children with normal growth status consumed relatively greater macronutrients, while stunted and underweight children consistently demonstrated lower intakes. Overall, inadequate macronutrient consumption was associated with poorer anthropometric outcomes, reflecting both acute (MUAC) and chronic (HAZ and BAZ) undernutrition.
Discussion
The findings indicate a substantial burden of undernutrition
among school-age children living in urban slums. High levels of
underweight, stunting and thinness reflect both acute and chronic
nutritional deprivation. Despite ongoing school and anganwadi
feeding initiatives, dietary inadequacy remains common, suggesting
that existing support systems may be insufficient to meet total
nutritional requirements. Similar burdens of malnutrition among
urban slum school children have been documented in other Indian
settings [3].
Socio-economic and environmental constraints likely contribute
to poor nutritional outcomes. Limited income, high dependency
ratios, inadequate sanitation and restricted dietary diversity may
predispose children to recurrent infections and reduced nutrient
absorption. Comparable findings have been reported from Bangladesh
and other disadvantaged populations [12,13].
Dietary assessments showed consistently low intake of energy
and micronutrients, particularly calcium and vitamin A, with heavy
reliance on cereal-based diets. Such patterns are known to predispose
children to multiple nutritional deficiencies [14]. The positive
association between higher nutrient intake and better MUAC status
highlights the usefulness of MUAC-for-age assessment in detecting
undernutrition among school-age children [15]. Anaemia, especially
among girls, further suggests underlying micronutrient deficiencies
and infection-related factors, consistent with regional epidemiological
evidence [16]. Nutritional status during late childhood also influences
pubertal timing and body composition, with BMI variations known
to affect growth and maturation outcomes [17].
Comparable patterns of undernutrition among schoolage
children living in socio-economically disadvantaged slum
environments have also been reported in other South Asian settings
[18], indicating that this remains a broader regional public health
challenge. Strengthening school feeding programmes, improving
access to diverse foods, and integrating nutrition education with
sanitation and hygiene interventions may help address these gaps.
The cross-sectional design and reliance on single-day dietary recall
are limitations; however, the study provides important baseline data
for an under-researched age group in urban slums.
Overall, inadequate dietary intake combined with unfavourable
living conditions appears to be a key contributor to persistent
undernutrition, underscoring the need for targeted community and
school-based nutrition strategies.
Conclusion
The present study demonstrated a high burden of undernutrition
among school-going children aged 6-9 years residing in urban
slums of Mumbai. Anthropometric indicators revealed widespread
underweight, stunting and thinness, accompanied by inadequate
energy and micronutrient intake. Morbidity, particularly anaemia,
was common. Despite utilisation of anganwadi and school meal
programmes, dietary intake remained insufficient to meet ageappropriate
requirements. Children with better dietary adequacy
showed improved anthropometric status, indicating a close
association between nutrient intake and growth.
These findings highlight the need for strengthened school feeding initiatives, improved dietary diversity, and community-based nutrition interventions to address persistent undernutrition in this vulnerable population.
These findings highlight the need for strengthened school feeding initiatives, improved dietary diversity, and community-based nutrition interventions to address persistent undernutrition in this vulnerable population.
Acknowledgements
I extend my appreciation to the University department for
providing the necessary academic support and infrastructure to
conduct this research. I would like to thank Ms. Aparna Thorat
for helping in the statistical analysis. Special thanks are due to the
Anganwadi workers, particularly Ms. Nazma Shaikh, for their
cooperation and help in mobilizing the children and their parents.
Finally, I am deeply grateful to all the participating children and their
caregivers for their time, trust, and wholehearted participation in the
study.
References
Citation
Abhipsha Gupta, Reema Mathur. Nutritional Status of School Going Children (6-9 Years Old) In the Western Suburban Slums of Mumbai. Indian J Nutri. 2026;13(1): 339.