Research Article
Impact of Oral Nutrition Supplement on Indian Older Adults with Chronic Kidney Disease (ION-CKD): Pilot Study
Aritra Khan1, Nikhil Kelkar2, Suman Kumar Biswas3, Samia Anam4, Chandan Bandyopadhyay5, Indrajit Majumder6, Anindya Maitra7* and Arnab Chatterjee8*
1Chief Dietitian, HOD (Clinical Dietetics), Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India.
2BDS, Clinical Nutrition Excellence Academy, Mumbai, India
3Assistant Clinical Dietitian, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
4Assistant Clinical Dietitian, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
5Associate Professor, Department of Economics, Asansol Girls’ College, Asansol, India
6Founder Secretary & Hony. Research Project Coordinator, Diabetes Awareness & You (DAY). India
7Consultant Physician & Nephrologist, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
8Assistant Professor, Department of Food & Nutrition, Asansol Girls’ College, Asansol, India
2BDS, Clinical Nutrition Excellence Academy, Mumbai, India
3Assistant Clinical Dietitian, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
4Assistant Clinical Dietitian, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
5Associate Professor, Department of Economics, Asansol Girls’ College, Asansol, India
6Founder Secretary & Hony. Research Project Coordinator, Diabetes Awareness & You (DAY). India
7Consultant Physician & Nephrologist, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India
8Assistant Professor, Department of Food & Nutrition, Asansol Girls’ College, Asansol, India
*Corresponding author:Dr. Anindya Maitra, Consultant Physician & Nephrologist, Samaritan Medical Surgical & Critical Care, Elgin Road, Kolkata, India. E-mail Id: anindya.maitra1@gmail.com
Dr Arnab Chatterjee, Assistant Professor, Department of Food & Nutrition, Asansol Girls’ College, Asansol, India E-mail id: arnabchatterjeenin@gmail.com
Dr Arnab Chatterjee, Assistant Professor, Department of Food & Nutrition, Asansol Girls’ College, Asansol, India E-mail id: arnabchatterjeenin@gmail.com
Article Information:Submission: 13/01/2026; Accepted: 19/02/2026; Published: 23/02/2026
Copyright: © 2026 Khan A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Older adults represent a substantial portion of the population in India. Chronic kidney disease (CKD) is one of the major noncommunicable diseases in India. Older adults are one of the most vulnerable groups that suffer from CKD. The prognosis of the CKD often worsens with chronic protein-energy wasting (PEW). Thus, to address the imbalances of the amino acid and suboptimal intake of nutrients in older adults, the impact of oral nutritional supplements (ONS) was assessed in the study.
Methods and Materials: A total of 41 samples were selected based on the inclusion and exclusion criteria. Several nutritional, biochemical, haematological, and renovascular parameters were assessed during the initiation and at the end of 30 days of the study.
Results: The results revealed that calorie and protein intake have improved in the participants who received the ONS. The positive impacts were also observed in the biochemical, haematological, and renovascular parameters.
Conclusion: It can be concluded that a controlled intervention under the guidance of a clinical dietitian can be useful in the management of CKD, especially for older adults.
Methods and Materials: A total of 41 samples were selected based on the inclusion and exclusion criteria. Several nutritional, biochemical, haematological, and renovascular parameters were assessed during the initiation and at the end of 30 days of the study.
Results: The results revealed that calorie and protein intake have improved in the participants who received the ONS. The positive impacts were also observed in the biochemical, haematological, and renovascular parameters.
Conclusion: It can be concluded that a controlled intervention under the guidance of a clinical dietitian can be useful in the management of CKD, especially for older adults.
Keywords:Chronic Kidney Disease; Oral Nutrition Supplement; Older Adults, Protein Energy Wasting, India
Introduction
In India, the population of older adults will be 324 million by
2050. One in every seven Indians will be older adults[1]. Thus, the
health and nutritional intervention strategies must be developed
now onwards to serve the population with utmost care and priority.
Apart from diabetes and hypertension, chronic kidney disease (CKD)
is one of the major concerns for older adults[2]. The estimated
glomerular filtration rate (eGFR) remains <60 mL/minute/1.73 m2
for three months or long that indicates the initiation of the disease[3].
Interestingly, the CKD is asymptomatic in the early-moderate
stage; more than fifty percent of the population is diagnosed when
the eGFR is <15 mL/minute/1.73m2. Older adults are one of the
vulnerable populations with a higher prevalence rate of CKD. As
the age grows, dysbiosis and disintegration of the epithelial layer are
common[2,4]. Thus, the population suffers from malnutrition. As the
kidney is also responsible for various metabolic regulations, loss of
functionality of renal cells enhances the chance of malnourishment
of the tissues. Overall, the synchronized impact of disintegration,
dysbiosis, and malnutrition will largely impact the food intake
capacity of the individual. Chronic anorexia will further enhance
the risk of morbidity and mortality, especially for older adults
with diabetes and hypertension[4]. In this context, the objectives
of the present study are to assess the impact of renal oral nutrition
supplements on the nutritional status of the individual. Furthermore,
the study will examine the changes in biochemical, haematological,
and renovascular variables of the older adults with CKD who received
ONS for a period of thirty days.
Methods and Materials
Study population:
Participants in the study were recruited from the Samaritan
Hospital in Kolkata, West Bengal, India, from November 2022
to December 2022. The selection criteria for the study were as
follows: the age between 55 and 95 years, diagnosed with CKD;
absence of infection; diagnosed as PEW according to the criteria
introduced by the International Society of Renal Nutrition and
Metabolism[5]; written informed consent and ability to understand
the study protocol. The exclusion criteria were any of the following:
the individual was not willing to provide informed consent and
comply with the protocol procedures, had a history of dialysis
noncompliance, malabsorption syndromes, chronic inflammatory
diseases of unknown origin, malignancy, nephrotic syndrome, or
chronic liver disease, the presence of recurrent acute illnesses, body
weight <40 kg, or if they were pregnant or lactating females. Patients
were also disqualified if they had recently undergone surgery or were
using any other dietary supplements. The study was carried out in
accordance with the ethical principles outlined in the latest version
of the Declaration of Helsinki and the applicable guidelines for good
clinical practice. Ethical approval for this study was obtained from the
institutional ethics committee.Nutritional Intervention:
The eligible participants were included in the study. The baseline
data, anthropometric measurements, and laboratory parameters were
assessed in both the pre- and post-intervention phases. Patients were
advised to take an oral nutritional supplement in addition to their
regular diet during the study period. The oral nutritional supplement
was scientifically designed with 100% HBV Whey Protein, sucrose
free, and an energy-dense formula, low potassium and phosphorus
levels. Patients were instructed to consume six scoops of oral
nutritional supplement powder thrice a day for 30 days, where one
serving (63g) was reconstituted in 100 mL of plain water. Disease
Specific Renal Nutritional Supplement (PentaSure Renal) (Hexagon
Nutrition Ltd) was used as an oral nutritional supplement. A clinical
dietician provided dietary counselling during the entire study period.Evaluation of nutritional status:
The body mass index (BMI) was estimated using the following
equation: BMI = body weight/height². Clinical dieticians involved
in the study used the 24-hour recall method to analyse the dietary
protein intake (DPI) and dietary energy intake (DEI). Further
values were obtained from the Indian Council of Medical Research recommended
Indian Food Composition Table databases. Body
weight was measured by using a standardized weighing scale.Laboratory parameters:
Blood samples from participants were collected at the beginning
and at the end of the study period. Serum creatinine (Cr), blood
glucose (Glu), haemoglobin (Hb), serum albumin (Alb), blood urea
nitrogen (BUN), serum phosphorus (P), and serum potassium (K),
using standard laboratory testing procedures. Even the White Blood
Cells (WBC), Red Blood Cells (RBC), and platelets were counted
using the standard procedure. Blood pressure was measured for all
the participants using the sphygmomanometer, and the standard
protocol was followed during measurement.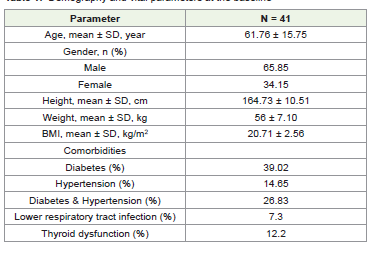
Statistical analyses:
Continuous data are summarized as arithmetic means with
standard deviation (SD). Changes from baseline to day 30 were
computed for all continuous variables and presented as mean change
with 95% confidence intervals (CI). Since all continuous data were
normally distributed, a paired sample t-test was used to compare the
baseline with day 30 (end of study) values for continuous variables.
Categorical and nominal data are presented as numbers with
percentages. All testing was done using two-sided tests at α 0.05 (95%
confidence level). Statistical analysis was performed using GraphPad
Prism 8.0 software.Results
Baseline Characteristics of Participants:
A total of 50 eligible patients were included in the study, but
only 41 completed it. Therefore, the results were analysed for these
41 patients. There were 27 (65.85%) men and 14 (34.15%) women
with a mean age of 61.76 ± 15.75 years. The demography and vital
parameters of the study participants at baseline are presented in
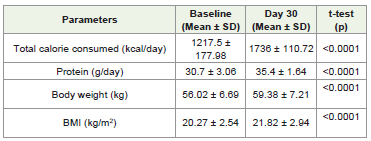
(Table 3.1)Changes in nutritional status:
The study also found that patients’ nutritional status improved
over the study period, with increased caloric and protein intake.
The mean caloric intake increased from 1217.5 ± 178.98 kcal/day
at baseline to 1736 ± 110.72 kcal/day at the end of the study while
administrating the ONS for the entire study period. Similarly, the
mean protein intake increased from 30.7 ± 3.06 g/day at baseline to
35.4 ± 1.64 g/day after the incorporation of ONS.Changes in biochemical status:
Several biochemical variables were measured for both the pre- and
post-intervention phases with ONS. The results showed that serum
albumin, blood urea nitrogen, creatinine, fasting, and postprandial
levels of glucose were significantly changed compared to the baseline
data. This significant improvement suggests enhanced nutritional
status and potentially better clinical outcomes. [Figure 1].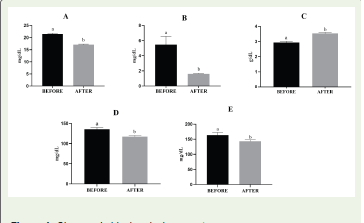
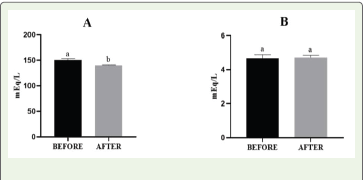
Changes in fluid and electrolyte balances:
The experimental results showed that electrolyte balance was
restored for patients who received the ONS. The sodium output was
significantly reduced; however, the potassium level did not show any
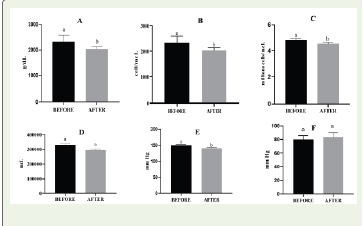
significant change. Even, the urine output level remained unchanged.Changes in hematological and renovascular parameters:
The study revealed that hemoglobin level was significantly
enhanced after the incorporation of ONS with the regular diet of
the participants. The higher WBC count is one of the inflammatory
markers. The ONS administration proved to be effective in reducing
the WBC of the participants. The erythropoiesis process is largely
affected by the decrease in renal function; however, the inclusion of
ONS in the regular diet of the participants significantly improved
the RBC count of the individuals. Excessive platelet count reflects a
higher inflammatory state of the physiological system. The targeted
ONS intervention showed a significant reduction in the platelet count
of the participants. Even the renovascular parameters, like the systolic
blood pressure, showed a remarkable decrease once the participants
started using the ONS on a regular basis.Discussion
International Society for Renal Nutrition and Metabolism
(ISRNM) advocates that the morbidity and mortality rate of CKD
increases due to protein-energy wasting (PEW) syndrome [6]. Thus,
the alteration in body composition will have a detrimental impact on
several metabolic processes [7]. The suboptimal intake of calories and
protein reduces insulin sensitivity, causing poor appetite; hence, the
ONS is essential to maintain the body’s homeostasis, especially for
older adults. In this study, we examined the impact of CKD on the
body weight and BMI level of the individuals. Several studies reported
that PEW-driven catabolism induces weight loss, and chronic
undernutrition is common in CKD. Thus, the changes in BMI are
inevitable. Prior meta-analyses showed that the impact of ONS is
effective along with a low-protein diet. Although the previously
available studies showed that the ONS targets mineral metabolism
pathways to counter the nutritional imbalances. However, the present
study showed that the incorporation of an ONS helps to replenish the
protein requirement of the participants along with the routine diet
and restricts the progression of CKD. Thus, body weight and BMI of
the participants were improved when compared to the baseline data.
The gradual decline of the glomerular filtration rate is associated with decreased appetite. This phenomenon greatly impacts the patient outcome. The regulation of food intake is controlled by multiple factors in non-dialyzed CKD patients. Several studies suggested that a cascade of reactions triggers anorexia in CKD patients, which is associated with increased secretion of proinflammatory cytokines and alteration of amino acid balance [8]. These conditions increased the tryptophan level across the blood-brain barrier. Thus, a hyper serotoninergic condition is one of the threats for CKD patients. The present study used the ONS, and the absorption of protein improved for the participants. Thus, the imbalance of the amino acid was corrected, which further enhanced the overall appetite of the participants. The results showed that the participants’ increased intake of protein and calories compared to their baseline data.
The gradual decline of the glomerular filtration rate is associated with decreased appetite. This phenomenon greatly impacts the patient outcome. The regulation of food intake is controlled by multiple factors in non-dialyzed CKD patients. Several studies suggested that a cascade of reactions triggers anorexia in CKD patients, which is associated with increased secretion of proinflammatory cytokines and alteration of amino acid balance [8]. These conditions increased the tryptophan level across the blood-brain barrier. Thus, a hyper serotoninergic condition is one of the threats for CKD patients. The present study used the ONS, and the absorption of protein improved for the participants. Thus, the imbalance of the amino acid was corrected, which further enhanced the overall appetite of the participants. The results showed that the participants’ increased intake of protein and calories compared to their baseline data.
The reabsorption of urea increases with the decrease rate of
urine flow. The primary sources of urea are dietary protein and the
turnover of tissue protein. BUN level reflects the nitrogen component
present in serum urea [9]. Amino acid imbalances and several other
external factors induce the dissociation of urea into cyanate, which
is further converted to isocyanate. Isocyanate has a higher affinity
towards the nucleophilic groups, like primary amines. Thus, the
isocyanate production causes the post-translational modification of
amino acids and proteins, causing several biochemical alterations,
known as carbamylation [10]. Therefore, uncontrolled urea can harm
various tissues, like vascular walls, pancreatic β-cells, and intestinal
epithelium. A study conducted in 2019 by Seki et al. on 459 Japanese
CKD patients showed that the BUN level is a crucial marker for
assessing the renal outcomes [11]. The dietary supply of protein is
essential to counter the adverse effects of amino acid imbalances.
The present study showed that a regulated administration of ONS
(PentaSure Renal) can address the ill impact of carbamylation on
tissues by reducing the BUN level of the participants.
As we discussed earlier, the PEW is a serious threat to the CKD patients. Thus, CKD patients suffer from fatigue, muscle wasting, and impaired cognition with the advancement of the disease. The essential nutrient that can counter this adversity is creatinine. As animal protein is a major source of dietary protein, the consumption of animal protein is often restricted for CKD patients [12]. Thus, patients are solely reliant on the endogenous creatine to combat the declining rate of muscle mass. But the initial step of endogenous protein synthesis depends on the renal cell masses. The enzyme arginine: glycine amidinotransferase (AGAT) secreted in the kidney converts arginine and glycine into guanidinoacetate. In the liver, the enzyme guanidinoacetate N-methyltransferase (GAMT) is involved in the methylation process to convert the guanidinoacetate to creatine [13]. Thus, the balanced intake of protein is essential, while the consumption of animal protein is restricted for CKD patients. Thus, ONS (PentaSure Renal) served the purpose in this study, and the results showed that the creatinine level of the participants reduced after the intervention.
As we discussed earlier, the PEW is a serious threat to the CKD patients. Thus, CKD patients suffer from fatigue, muscle wasting, and impaired cognition with the advancement of the disease. The essential nutrient that can counter this adversity is creatinine. As animal protein is a major source of dietary protein, the consumption of animal protein is often restricted for CKD patients [12]. Thus, patients are solely reliant on the endogenous creatine to combat the declining rate of muscle mass. But the initial step of endogenous protein synthesis depends on the renal cell masses. The enzyme arginine: glycine amidinotransferase (AGAT) secreted in the kidney converts arginine and glycine into guanidinoacetate. In the liver, the enzyme guanidinoacetate N-methyltransferase (GAMT) is involved in the methylation process to convert the guanidinoacetate to creatine [13]. Thus, the balanced intake of protein is essential, while the consumption of animal protein is restricted for CKD patients. Thus, ONS (PentaSure Renal) served the purpose in this study, and the results showed that the creatinine level of the participants reduced after the intervention.
Several studies have demonstrated that lower serum albumin is
an indicator of the prognosis of CKD [14]. However, there is no direct
relationship that has been established between these two clinical
conditions. Low serum albumin may be a cause of dysfunction of liver
dysfunction and chronic inflammation in CKD patients [15]. Thus,
malnutrition needs to be corrected to challenge the inflammation. A
study conducted by Lange et.al. in 2018 showed that inflammation
needs to be corrected, especially for elderly CKD patients, and
correction of serum albumin level could serve as one of the markers
to evaluate the impact of intervention on the CKD patients [16]. Our
study showed that when the group was administered the ONS, the
serum albumin level improved and complied with the previously
available findings.
The quality and quantity of protein in the Indian diet are major
concerns. Even the patients of CKD are anorexic due to the PEW.
Along with the essential micronutrients, it is recommended that
patients with CKD have a 0.6-0.8g/kg body weight of protein per day
and 1-1.2g/kg of protein per day for non-dialysis and dialysis patients,
respectively [17]. Studies suggested that to supply the essential protein
and calories the clinicians largely rely on the ONS. But the glycaemic
load of the ONS is one of the major bottlenecks for CKD patients
[8]. In the present study, the ONS showed a significant reduction of
fasting and postprandial blood glucose levels of the participants after
consumption of the product for thirty days under the supervision of
the clinicians.
Several studies reported that CKD often compromises the electrolyte regulation of individuals. Electrolyte dysregulations can be life-threatening. Hyperkalemia, dysnatremia, and dysmagnesemia are the three common electrolyte disturbances seen in CKD. Once the serum K+ concentration is >5.3 mEq/L, the condition is termed hyperkalemia. The distal part of the nephron, based upon the physiological needs, secretes and reabsorbs K+. Aldosterone regulates, and the basolateral Na+ / K+-ATPase mediates the tight regulation of apical Na+-Cl – cotransporter, renal outer medullary K+ (ROMK) channel, epithelial sodium channel (ENaC), and BK channels, allowing the distal nephron to control the extrusion of K+. A retrospective study conducted with 2,40000 sample size showed that the CKD patients are prone to hyperkalemia compared to the non-CKD patients [18].
Several studies reported that CKD often compromises the electrolyte regulation of individuals. Electrolyte dysregulations can be life-threatening. Hyperkalemia, dysnatremia, and dysmagnesemia are the three common electrolyte disturbances seen in CKD. Once the serum K+ concentration is >5.3 mEq/L, the condition is termed hyperkalemia. The distal part of the nephron, based upon the physiological needs, secretes and reabsorbs K+. Aldosterone regulates, and the basolateral Na+ / K+-ATPase mediates the tight regulation of apical Na+-Cl – cotransporter, renal outer medullary K+ (ROMK) channel, epithelial sodium channel (ENaC), and BK channels, allowing the distal nephron to control the extrusion of K+. A retrospective study conducted with 2,40000 sample size showed that the CKD patients are prone to hyperkalemia compared to the non-CKD patients [18].
Even serum Na+ concentration is affected by the reduced
functionality of the nephrons. Na+ is also a primary determinant
of the serum osmolality and water balance. The changes in serum
osmolality regulate the influx and efflux of fluid in the cells. The
supraoptic and paraventricular nuclei of the hypothalamus produce
Arginine vasopressin (AVP). Once the serum osmolality increases
and intravascular volume decreases, the AVP is released from the
posterior pituitary. The basolateral membrane of collecting ducts
contains V2 receptors, which bind with AVP. Thus, the conjugation
activates the production of adenylyl cyclase-mediated cAMP and
PKA signalling. Increased production of cAMP and phosphorylation
induce apical membrane insertion of aquaporin 2 channels. Thus,
the presence of the tubulomedullary osmotic gradient enhances free
water absorption. A cohort study with a large sample size showed that
CKD patients are prone to dysnatremia, which further causes fluid
imbalances [19]. Our study showed that the administration of ONS is
effective in regulating the electrolyte balance for participants.
Anaemia is most common among CKD patients. However, haemoglobin level cannot be considered as a prominent marker to check the state of iron availability of CKD patients. Several metaanalyses showed that there is a nonlinear and negative relationship between CKD and the progression of CKD. But a study conducted by Pan et al suggested that a reduced haemoglobin level of 8.6 g/dL or less may suggest a renal endpoint risk. The present study showed that consumption of ONS is effective in improving the haemoglobin level of individuals [20].
Fan et al reported that an increase in WBC count is positively correlated with the advancement of CKD. WBC count is one of the inflammatory markers [21]. Thus, various studies reported that if the correct ONS is introduced at the right time in the management of CKD, the chances of renal failure can be prevented. The present study also showed that the WBC count substantially reduced once the ONS was administered to the participants.
As we discussed earlier the anaemia is common among CKD patients. The studies reported that, though the plasma ferritin remains normal for CKD patients, the plasma iron and transferrin concentrations decrease compared to a non-CKD person. The reduced plasma iron and transferrin concentrations signify the increased level of inflammation in CKD patients. Thus, the overall erythropoiesis process is altered, and RBC death is prominent with reduced GFR. Several studies reported that the rate of reduction of inflammation could improve RBC count of the individual with CKD. The present study also reported the same [22].
The kidney plays a major role in maintaining the body’s homeostasis. Whereas the platelets are responsible for patrolling the blood circulation with a stable disk shape [23]. The platelets are extremely reactive to the biological changes in the vessel wall. Any form of infection or injury can affect the activation or aggregation of platelets in the biological system. The kidney has a large network of arterioles and glomerular capillaries. Hence, the studies reported that any progressive impairment of the kidney leads to a reduction of antiplatelet mediators [24]. Thus, the enhanced number of platelets is usual for a CKD patient. But the present study reported that a reduction in platelet count showed that the ONS (Penta Sure Renal) might help in the reduction of inflammation and support the CKD patients.
Studies suggested that 60-90% of CKD patients suffer from hypertension. Several mechanisms are associated with the elevated level of blood pressure (BP) in CKD, including the increased activity of RAAS. The activation of RAAS causes narrowing of peritubular capillaries downstream of sclerosed glomeruli [25]. The reduction of blood flow increases the secretion of renin, which further triggers the circulating angiotensin II levels. Therefore, the blood pressure of the CKD patients increased due to systemic vascular resistance and a direct vasoconstrictor effect. This condition is termed renovascular disease, where the narrowing of renal arteries increases the overall blood pressure [26]. Even the chronic inflammation due to the PEW in CKD patients leads to a reduction of functional nephrons, which further increases the load on the existing nephron and causes the narrowing of the arteries. Thus, this vicious cycle needs nutritional intervention. Our study showed that the ONS administration helped in the supply of the protein requirement of the participants, and the reduction of blood pressure of the participants.
Anaemia is most common among CKD patients. However, haemoglobin level cannot be considered as a prominent marker to check the state of iron availability of CKD patients. Several metaanalyses showed that there is a nonlinear and negative relationship between CKD and the progression of CKD. But a study conducted by Pan et al suggested that a reduced haemoglobin level of 8.6 g/dL or less may suggest a renal endpoint risk. The present study showed that consumption of ONS is effective in improving the haemoglobin level of individuals [20].
Fan et al reported that an increase in WBC count is positively correlated with the advancement of CKD. WBC count is one of the inflammatory markers [21]. Thus, various studies reported that if the correct ONS is introduced at the right time in the management of CKD, the chances of renal failure can be prevented. The present study also showed that the WBC count substantially reduced once the ONS was administered to the participants.
As we discussed earlier the anaemia is common among CKD patients. The studies reported that, though the plasma ferritin remains normal for CKD patients, the plasma iron and transferrin concentrations decrease compared to a non-CKD person. The reduced plasma iron and transferrin concentrations signify the increased level of inflammation in CKD patients. Thus, the overall erythropoiesis process is altered, and RBC death is prominent with reduced GFR. Several studies reported that the rate of reduction of inflammation could improve RBC count of the individual with CKD. The present study also reported the same [22].
The kidney plays a major role in maintaining the body’s homeostasis. Whereas the platelets are responsible for patrolling the blood circulation with a stable disk shape [23]. The platelets are extremely reactive to the biological changes in the vessel wall. Any form of infection or injury can affect the activation or aggregation of platelets in the biological system. The kidney has a large network of arterioles and glomerular capillaries. Hence, the studies reported that any progressive impairment of the kidney leads to a reduction of antiplatelet mediators [24]. Thus, the enhanced number of platelets is usual for a CKD patient. But the present study reported that a reduction in platelet count showed that the ONS (Penta Sure Renal) might help in the reduction of inflammation and support the CKD patients.
Studies suggested that 60-90% of CKD patients suffer from hypertension. Several mechanisms are associated with the elevated level of blood pressure (BP) in CKD, including the increased activity of RAAS. The activation of RAAS causes narrowing of peritubular capillaries downstream of sclerosed glomeruli [25]. The reduction of blood flow increases the secretion of renin, which further triggers the circulating angiotensin II levels. Therefore, the blood pressure of the CKD patients increased due to systemic vascular resistance and a direct vasoconstrictor effect. This condition is termed renovascular disease, where the narrowing of renal arteries increases the overall blood pressure [26]. Even the chronic inflammation due to the PEW in CKD patients leads to a reduction of functional nephrons, which further increases the load on the existing nephron and causes the narrowing of the arteries. Thus, this vicious cycle needs nutritional intervention. Our study showed that the ONS administration helped in the supply of the protein requirement of the participants, and the reduction of blood pressure of the participants.
Conclusion
The extensive study on the impact of ONS in older adults with
CKD showed that the individuals’ protein energy wasting is a major
underlying cause of mortality and morbidity of patients with CKD.
Thus, to provide adequate macro and micro nutrients to stop the
malnutrition, data support the efficacy of the ONS. The ONS has
been proven to be effective in the prevention of advancement of
CKD by improving the nutritional, biochemical, haematological,
and renovascular parameters. However, the present study has several
limitations, but the assessment of the initial trends will be helpful to
design a strong and robust methodological framework to identify the
impact of ONS on older adults with CKD.
Funding Statement:
No funding was received. Oral nutritional supplements were
procured independently through the hospital pharmacy as part of
routine care. The manufacturer had no role in study design, data
collection, analysis, interpretation, manuscript writing, or publication
decision.Conflict of Interest:
The authors declare no financial or personal conflicts. Dr. Nikhil
Kelkar’s affiliation was fully disclosed; he had no role in patient care,
recruitment, data collection, analysis, or interpretation.Authors Contribution:
The corresponding authors provided manuscript oversight and
handled journal correspondence. Clinical care and data collection
were performed at Medical Surgical & Critical Care by Dr. Aritra
Khan and the clinical team, including Suman Kumar Biswas and
Samia Anam. Chandan Bandyopadhyay and Indrajit Majumder were
involved in the data analyses and project monitoring accordingly.Acknowledgement
The research was supported by Samaritan Medical Surgical &
Critical Care, Dr. S.K. Mitra, Medical Superintendent
Declaration of Competing Interest:
The authors declare that they have no known competing financial
interests or personal relationships that could have appeared to
influence the work reported in this paper.Ethical Approval:
This study was approved by the Institutional Ethics
Committee, Samaritan Clinic Pvt Ltd, Elgin Road, Kolkata,
U85110WB11984PTC037486References
Citation
Khan A, Kelkar N, Biswas SK, Anam S, Bandyopadhyay C, et al. Impact of Oral Nutrition Supplement on Indian Older Adults with Chronic Kidney Disease (ION-CKD): Pilot Study. Indian J Nutri. 2026;13(1): 338.