Research Article
Nutritional Assessment of Geriatric Cancer Patients with Esophagus and Head and Neck Cancer (HNC)
Priyanka Srivastava*, Barna Ganguly, Nitiraj Shete Nirav A Asarawala and Bharat M. Gajjar
Department of Medical Oncology, Rayos Comprehensive Cancer Care, Anand, Gujarat, India.
*Corresponding author:Dr Priyanka Srivastava, Department of Medical Oncology, Rayos Comprehensive Cancer Care, Anand, Gujarat, India. E-mail Id: priyankasrivastavadr@gmail.com
Article Information:Submission: 01/02/2026; Accepted: 18/02/2026; Published: 20/02/2026
Copyright: ©2026 Srivastava P. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:The oesophageal and HNC patients suffer from dysphagia and frequently present with undernourishment. The treatment related toxicities are higher and survival outcomes are poorer in undernourished patients. The geriatric cancer patients (age ≥ 65 years) encounter a unique
challenge of age-related undernourishment, which further gets aggravated due to disease biology. There are very few studies from western Indian population to evaluated baseline malnourishment in geriatric cancer patients and its association with treatment outcome.
Objectives: To assess baseline nutritional status and its association with demographic, clinic-pathological and treatment outcome parameters in geriatric cancer patients undergoing chemotherapy treatment.
Materials and Methods:This observational study was conducted at M.S. Patel Cancer Center, Shreekrishna Hospital, Bhaikaka Univeristy, Karamsad, Gujarat, India. The Geriatric cancer patients diagnosed with HNN and esophageal cancer, being treated with curative intent chemotherapy were enrolled in the study from April 2021 to March 2023. Total 89 patients were included in this study. Baseline clinic-pathological data including geriatric assessment was noted. Based on body mass index (BMI) patients were dichotomized in to BMI < 18.5 i.e. undernourished and ≥18.5. An assessment of treatment outcomes including survival as per nutrition status was done.
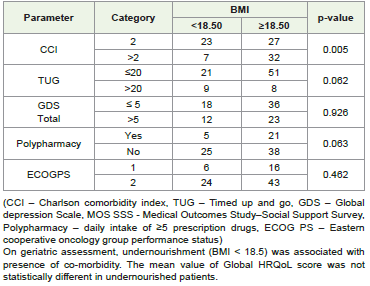
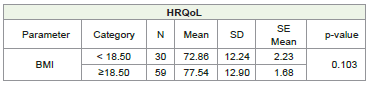
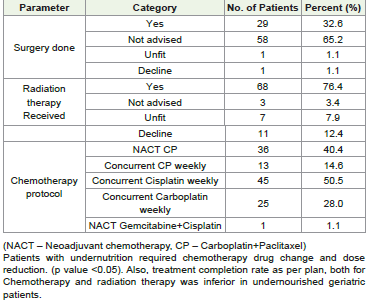
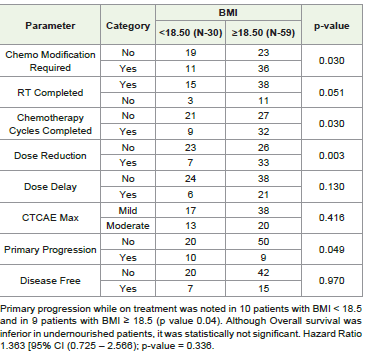
Results:Out of total 89 patients, 78.7% were males, 95.5% patients were from middle and lower SES, 84.26% patients had HNC and 15.74% esophageal cancer. Patients with metastatic disease were not included in this study. At baseline presentation, as per BMI 33.7% patients were malnourished. On geriatric assessment, malnourishment (BMI < 18.5) was associated with presence of co-morbidity (p value <0.05). Patients with malnutrition required chemotherapy protocol modification and dose reduction (p value <0.05). Treatment completion rate for Chemotherapy and radiation therapy was inferior in malnourished geriatric patients. Primary progression while on treatment was noted in 10 patients with BMI < 18.5 and in 9 patients with BMI ≥ 18.5 (p value - 0.04). Although HR QOL global mean score and Overall survival were inferior in malnourished patients, it was statistically not significant.
Conclusion:A significant proportion of geriatric cancer patients with esophagus and HNC suffer from malnourishment. It adversely affects treatment completion rate and progression free survival in this group of patients. A timely nutritional assessment and dietary interventions should be an integral part of geriatric cancer patient management.
Objectives: To assess baseline nutritional status and its association with demographic, clinic-pathological and treatment outcome parameters in geriatric cancer patients undergoing chemotherapy treatment.
Materials and Methods:This observational study was conducted at M.S. Patel Cancer Center, Shreekrishna Hospital, Bhaikaka Univeristy, Karamsad, Gujarat, India. The Geriatric cancer patients diagnosed with HNN and esophageal cancer, being treated with curative intent chemotherapy were enrolled in the study from April 2021 to March 2023. Total 89 patients were included in this study. Baseline clinic-pathological data including geriatric assessment was noted. Based on body mass index (BMI) patients were dichotomized in to BMI < 18.5 i.e. undernourished and ≥18.5. An assessment of treatment outcomes including survival as per nutrition status was done.
Results:Out of total 89 patients, 78.7% were males, 95.5% patients were from middle and lower SES, 84.26% patients had HNC and 15.74% esophageal cancer. Patients with metastatic disease were not included in this study. At baseline presentation, as per BMI 33.7% patients were malnourished. On geriatric assessment, malnourishment (BMI < 18.5) was associated with presence of co-morbidity (p value <0.05). Patients with malnutrition required chemotherapy protocol modification and dose reduction (p value <0.05). Treatment completion rate for Chemotherapy and radiation therapy was inferior in malnourished geriatric patients. Primary progression while on treatment was noted in 10 patients with BMI < 18.5 and in 9 patients with BMI ≥ 18.5 (p value - 0.04). Although HR QOL global mean score and Overall survival were inferior in malnourished patients, it was statistically not significant.
Conclusion:A significant proportion of geriatric cancer patients with esophagus and HNC suffer from malnourishment. It adversely affects treatment completion rate and progression free survival in this group of patients. A timely nutritional assessment and dietary interventions should be an integral part of geriatric cancer patient management.
Keywords:Geriatric; Cancer; Malnutrition; BMI; Chemotherapy; Adverse Drug Reaction
Introduction
Malnourishment has been described as a “deficiency, excess or
imbalance of a wide range of nutrients, resulting in a measurable
adverse effect on body composition, function and clinical outcome.”
[1] Malnutrition in cancer patients occurs due to disease biology
and treatment side effect, which can be described as anorexia and
cachexia. Cancer cachexia manifests as a significant reduction in
adult body weight, accompanied by changes in body composition
and disturbances in the balance of the biological system. It causes
progressive dysfunction, systemic inflammatory response, negative
protein-energy balance, and involuntary loss of lean body mass, with
or without a decline in adipose tissue. [2] Cachexia is considered
as a major contributor to morbidity, to impaired QOL, increase in
healthcare costs and accounts for 20% of all cancer-related deaths.
[3] Patients with HNC and oesophageal cancer are at greatest risk of
cachexia and malnutrition due to direct involvement of anatomical
structure involved in food deglutition. [4] In HNC patients mechanical
swallowing/chewing difficulties (dysphagia/odynophagia), pain, taste
alterations and xerostomia also attribute to low oral intake and weight
loss before and during treatment. [5]
In Geriatric age group patients (age ≥65 years), physiological
sarcopenia i.e. muscle wasting and weakness can further worsen
the deficits associated with cancer cachexia. Malnutrition is an
important part of multifactorial geriatric syndrome, yet it is often
under-recognised. Other than advanced age and cancer stage,
frailty, dementia, major depression, functional impairment, and
physical performance are important risk factors for malnourishment.
[16] Several screening and assessment tools are used for nutritional
assessment in geriatric cancer patients including the BMI, Mini
Nutrition Assessment (MNA), the Malnutrition Universal Screening
Tool (MUST), and the Patient-Generated Subjective Global
Assessment (PG-SGA).[7] The International Society for Geriatric
Oncology (SIOG) has recommended “the inclusion of nutritional
assessment before the start of active cancer treatment for older adults,
after taking consideration of the deleterious impact of malnutrition on
older adults with cancer.”[8] There are very few studies of nutritional
assessment and its impact of treatment outcome in geriatric cancer
patients from Western Indian population.
This study was conducted to analyses the prevalence of
malnutrition in our geriatric cancer patient population with HNC
and oesophageal Cancer, and its association with baseline geriatric
assessment parameters and treatment outcomes.
Methodology
This study was a part of a PhD study dealing with the chemotherapy
ADRs in Geriatric cancer patients treated with curative intent. This
prospective, observational study, was conducted at M.S.Patel Cancer
Centre, Bhaikaka University, Karamsad, Gujarat. Study was approved
by IEC – April 2021. Patients were enrolled from April 2021 till
March 2023. The study was conducted according to ethical guidelines
established by the Declaration of Helsinki, Good Clinical Practice
Guidelines, and the Indian Council of Medical Research guidelines.
Since this not an interventional clinical trial, it was not registered
with the Clinical Trials Registry India. Written informed consent
was taken from all the participants before enrolment in the study.
Baseline assessment included Age, Gender, socio-economic strata
(SES) (Modified Kuppuswamy socioeconomic scale), presenting
symptom and its duration, Eastern Cooperative Oncology Group
Performance status (ECOG PS), Geriatric assessment, Clinical
examination, Investigations (Laboratory and Radiological). Details of
final diagnosis, planned surgery, radiation therapy and chemotherapy
were noted. Any change in chemotherapy dosing, schedule, and
protocol selection in view of assessment at baseline were recorded.
Adverse drug reactions (ADRs) assessment was done using Common
Terminology Criteria for Adverse Events version 5.0 (CTCAE v5.0).
Follow-up was planned up to one year post chemotherapy. The
overall survival (OS) was calculated from the date of diagnosis until
the time of death or last follow-up, while the Relapse-free survival
(RFS) was calculated from the time of diagnosis until recurrence,
primary progression, or death.
Statistical analysis: All quantitative variables are expressed in
terms of Mean ± SD subject to variable follows normal distribution
or Median (IQR) if variable is non-normal. All qualitative variables
are expressed in terms of frequency and percentage. Chi-square test
is used to test association between categorical outcomes. Appropriate
independent sample t-tests and ANOVA are used to test significance
of quantitative study variables with assumption outcome variable
having two categories and more than two categories respectively. All
above analysis was done using Excel and IBM SPSS version 25.0. The
p-value less than 0.05 considered to be significant. To identify factors
influencing binary outcome variable we applied logistic regression
and Odds ratio (95% CI) and p-value is reported.
Results
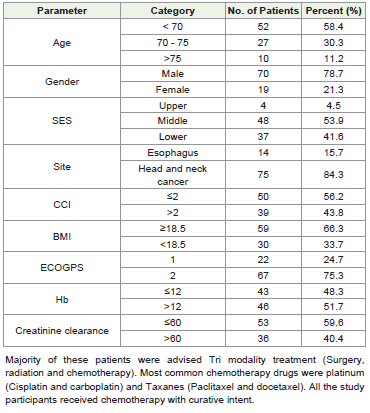
Out of total 89 patients, 78.7% were males and majority of
these patients were from middle and lower SES (95.5%). Seventyfive
patients had HNC and 14 patients had oesophagus primary.
Metastatic disease patients were excluded from the study. Additional
comorbidities were present in 43.8% patients. Twenty five percent
patients had ECOG PS 1 and 75 % had ECOG PS 2. The formula for
calculation of BMI as follows, BMI = weight (kg)/height2 (m). A BMI
of < 18.5 is considered under nourished.[9]
Discussion
Malnutrition in geriatric population and specially with

esophageal and HNC cancer patients is multifactorial, some of which
are correctable with timely diagnosis and intervention. The present
study highlights the need of comprehensive geriatric assessment
including nutrition in patients with HNN and oesophageal cancer.
In this group of patient’s malnutrition is multifactorial and adversely
affects treatment outcome. Timely identification of malnourishment
and early intervention is the key to prevent poor outcomes from
chemotherapy and the disease itself. BMI is an easy nutritional
assessment tool, that includes height and weight of patient. Globally
BMI < 18.5 is considered as undernourished. [1] As per BMI scale
33.7% of the patients were undernourished in this study.
The MNA was originally developed to identify patients 65 years
or older at risk of malnutrition irrespective of a specific disease.
Both versions, the short-form and long-form, are recommended
for screening of nutritional status of older patients. In MNA short
form screening maximum score is 14. Scores ≥12 indicate satisfactory
nutritional status, with no further requirement. A screening score ≤ 11
suggests risk for malnutrition.[11] In a study conducted by Rubenstein
et al, the MNA short form had 97.9% sensitivity, 100% specificity and
98.7% diagnostic accuracy for predicting undernutrition.[12] The
MNA takes recent weight loss, loss of appetite, mobility, and neuropsychological
parameters in to account as well unlike BMI which
is a one-time assessment. Many studies have evaluated MNA and
other nutritional assessment tools and highlighted need for more
comprehensive assessment including serum albumin, hemoglobulin
and skeletal muscle mass as an appropriate tool. [13,14]. In an Indian
study conducted by Noronha et al revealed that 75% of patients had
abnormal MNA scores. [15]
Malnutrition has been associated with cognitive decline and frailty. A systemic review of 6 longitudinal studies evaluating risk factors for malnutrition in the older population highlights significance of cognitive decline (OR: 1.844; P = 0.001), dementia (OR: 2.139; P = 0.001). [3] In our study, comprehensive geriatric assessment suggests that undernourishment was associated with higher CCI.
Malnutrition has been associated with cognitive decline and frailty. A systemic review of 6 longitudinal studies evaluating risk factors for malnutrition in the older population highlights significance of cognitive decline (OR: 1.844; P = 0.001), dementia (OR: 2.139; P = 0.001). [3] In our study, comprehensive geriatric assessment suggests that undernourishment was associated with higher CCI.
In a systematic review of nutrition as potential prognostic
factor for health and treatment outcomes in patients with cancer,
23 out of 56 studies merged patients with malnutrition and at risk
of malnutrition as MNA scores, and reported 27.0–85.0% being at
least at risk. In a chemotherapy prediction model validated by Hurria
et al mini-nutritional assessment was an important predictor of
grade 3 and 4 nonhematologic toxicity. [4] In our study also study
malnutrition predicted mortality/survival, cancer progression,
treatment maintenance and (health-related) quality of life and did not
predict adverse treatment outcomes and functional status/ decline
in patients with cancer. In our patient population more patients
with undernutrition required chemotherapy drug change and dose
reduction. ( p value<0.05). Primary progression while on treatment
was noted in 10 patients with BMI < 18.5 and in 9 patients with BMI
≥ 18.5 (p value 0.04). In older age patients’ cancer cachexia is a key
predictor of mortality. [5] In our study although Overall survival was
inferior in undernourished patients, it was statistically not significant.
There are few limitations of our study. It was conducted at a single centre, only esophageal and HNC patients were included in this study. Metastatic disease patients were excluded. Most of the patients were from middle and lower socioeconomic status. These factors may affect nutrition status and treatment outcome. it will be difficult to extrapolate the result in patients form upper SES who have better access to supportive health care and to patients diagnosed with other sites of malignancy. This is an observational study so impact of dietary intervention could not be commented upon.
There are few limitations of our study. It was conducted at a single centre, only esophageal and HNC patients were included in this study. Metastatic disease patients were excluded. Most of the patients were from middle and lower socioeconomic status. These factors may affect nutrition status and treatment outcome. it will be difficult to extrapolate the result in patients form upper SES who have better access to supportive health care and to patients diagnosed with other sites of malignancy. This is an observational study so impact of dietary intervention could not be commented upon.
Conclusion
Our study highlights the high prevalence of malnutrition in this
group of patient population. Malnutrition is associated with frailty,
poor PS, cognition, and functional decline. It adversely affects clinical
outcome in cancer patients. Incorporating CGA in every geriatric
oncology patient and early dietary intervention are unmet need of
hour.
References
Citation
Srivastava P. Nutritional Assessment of Geriatric Cancer Patients with Esophagus and Head and Neck Cancer (HNC). Indian J Nutri. 2026;13(1): 337.