Research Article
Gender Differences in Dietary Practices among People with Type 2 Diabetes. A Study from South India
Janakiraman UM, Kumpatla S and Viswanathan V*
Department of Diabetes Research Centre M.V. Hospital, West Madha Church Street, Royapuram, Chennai, Tamil Nadu, India
*Corresponding author:Dr. Vijay Viswanathan, Department of Diabetes Research Centre M.V. Hospital, West Madha Church Street, Royapuram, Chennai, Tamilnadu, India. E-mail Id: drvijay@mvdiabetes.com
Article Information:Submission: 05/01/2026; Accepted: 27/01/2026; Published: 30/01/2026
Copyright: © 2026 Janakiraman UM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:Evidence on food intake among people with diabetes in India is limited. Aim was to assess gender differences in the dietary practices, food frequency, calorie distribution and nutrient composition among people with type2 diabetes(T2DM).
Methods: A total of 454 participants were included and their sociodemographic, anthropometric, biochemical, 24hours dietary-recall were recorded. Food frequency of different food items and nutrient composition such as total calorie, Carbohydrate, Protein and Fat were calculated. Recommended Dietary Allowance (RDA) for Indian population was used.
Results: The total calorie intake was higher in males (1410kcals) than females (1303kcals). Consumption of carbohydrate(gms) (M: F 220 vs 201) (P<0.001), Protein(gms) (M: F 49 vs 46) (p=0.006) was significantly higher in males than females. The fat consumption was similar in both genders. The percentage of carbohydrate intake was higher (M: F 63.7 vs 63.2%) and protein intake (M: F 13.9 vs 14%) was lesser in both genders as compared to RDA of Indian population. Green leafy vegetables and consumption of other vegetables was also lesser.
Conclusion:The level of protein, green leafy vegetables and other vegetables consumption was lesser than recommendations among people with T2DM. Intensive diet counselling should be focused on recommendation of protein rich foods to meet the requirements.
Methods: A total of 454 participants were included and their sociodemographic, anthropometric, biochemical, 24hours dietary-recall were recorded. Food frequency of different food items and nutrient composition such as total calorie, Carbohydrate, Protein and Fat were calculated. Recommended Dietary Allowance (RDA) for Indian population was used.
Results: The total calorie intake was higher in males (1410kcals) than females (1303kcals). Consumption of carbohydrate(gms) (M: F 220 vs 201) (P<0.001), Protein(gms) (M: F 49 vs 46) (p=0.006) was significantly higher in males than females. The fat consumption was similar in both genders. The percentage of carbohydrate intake was higher (M: F 63.7 vs 63.2%) and protein intake (M: F 13.9 vs 14%) was lesser in both genders as compared to RDA of Indian population. Green leafy vegetables and consumption of other vegetables was also lesser.
Conclusion:The level of protein, green leafy vegetables and other vegetables consumption was lesser than recommendations among people with T2DM. Intensive diet counselling should be focused on recommendation of protein rich foods to meet the requirements.
Keywords:Food Frequency, 24hrs Dietary Recall, Calorie Distribution, Nutrient Composition
Abbreviations
Recommended Dietary Allowance (RDA); Type2 Diabetes Mellitus (T2DM)
Introduction
Around 537 million adults are living with diabetes worldwide
and this number is predicted to rise to 643million by 2030 and
783million by 2045 [1]. According to ICMR INDIAB study, the
prevalence of diabetes and prediabetes in India is reported as
101million and 136 million respectively [2]. Diet plays a major
role in type 2 diabetes(T2DM) coupled with physical activity(PA).
Dietary guidance helps in prevention of T2DM and also helps in initial management of the condition prior to pharmological treatment [3-6]. It involves the avoidance of rapidly absorbed simple carbohydrates, a reduction in fat intake, an increase in high fiber (HF) foods and a balanced distribution of complex carbohydrates [3,5-9]. HF diet have been shown to control hyperglycaemia, modifying meal frequency and size altered nutrient uptake afford better glycemic control(GC) [8]. GC can also be achieved by calorie restriction and weight reduction [10].
Dietary guidance helps in prevention of T2DM and also helps in initial management of the condition prior to pharmological treatment [3-6]. It involves the avoidance of rapidly absorbed simple carbohydrates, a reduction in fat intake, an increase in high fiber (HF) foods and a balanced distribution of complex carbohydrates [3,5-9]. HF diet have been shown to control hyperglycaemia, modifying meal frequency and size altered nutrient uptake afford better glycemic control(GC) [8]. GC can also be achieved by calorie restriction and weight reduction [10].
Healthy dietary practice can improve various factors which
include obesity, insulin release, hypertension. Absence of healthy
dietary practice is crucial declining factor in attaining GC in
T2DM. Individuals with diabetes are generally not aware of its
value in assuring better GC [11,12]. Diet related self-care practices,
individual preferences, availability of food substitute at affordable
level, knowledge about ideal diet and PA plays an important
role in self-care dietary practice [13]. A greater knowledge of
the dietary practices among people with T2DM is important
for healthcare professionals for better treatment outcomes. A
systematic review of studies modelling dietary pattern of general
population in India was reported in 2016. A large variations in
dietary pattern was evident in the above review but the literature
available on dietary practices followed by people with T2DM
is limited in Indian context [14]. Hence, the study was aimed
to assess the gender differences in the dietary practices, food
frequency, calorie distribution and nutrient composition among
people with T2DM.
Materials and Methods
This cross-sectional study was conducted among people with
T2DM, between Nov2020-Oct2022 attending a tertiary care
centre in Chennai, South India. A total of 454 participants
(Male: Female 289:165) were included and participants who are
following ketogenic diet, paleo diet and restricted diet and people
with gestational diabetes, type 1 diabetes, chronic illness were
excluded.
Sociodemographic details such as education, occupation, family
income, location, marital status, habits, medication details, PA
were recorded. Standardized protocols were used to collect the
anthropometric measurements such as weight measured in light
clothing without shoes. BMI was calculated as kg/m2.
Blood pressure(BP), clinical and biochemical measurements were
also recorded. Glycated haemoglobin(HbA1c) was estimated
by immunoturbidimetric method using fully automated Roche
c311 analyzer. Presence of co-morbid conditions and diabetic
complications were recorded. The Study protocol was approved
by the institution’s ethical committee (Ref IEC/N-003/11/2020).
Informed consent was obtained from all the participants.
24hours dietary recall was taken to evaluate their dietary habits and nutrient composition such as total calories, Carbohydrate(CHO), Protein and Fat% were calculated. Food frequency of different food items, consumption of different types of oils was identified and whether the participants consumed these items daily, alternative days, twice a week, once a week, rarely or never was recorded. The Recommended Dietary Allowance (RDA) and Indian Food Composition Table (IFCT) for Indian population was used for reference [15,16]. Details on PA, timing of consumption of food, meal schedule and composition were recorded.
24hours dietary recall was taken to evaluate their dietary habits and nutrient composition such as total calories, Carbohydrate(CHO), Protein and Fat% were calculated. Food frequency of different food items, consumption of different types of oils was identified and whether the participants consumed these items daily, alternative days, twice a week, once a week, rarely or never was recorded. The Recommended Dietary Allowance (RDA) and Indian Food Composition Table (IFCT) for Indian population was used for reference [15,16]. Details on PA, timing of consumption of food, meal schedule and composition were recorded.
Statistical analysis:
The normality of the data was checked and median values
are reported for continuous variables which showed skewed
distribution. Number and percentages are reported for categorical
variables. Mann-Whitney U and chi-square tests were used to
see the statistical significance in clinical profile and dietary
intake among male and female participants. A p-value of <0.05
was considered as statistically significant. Statistical analysis was
performed using IBM SPSS version 28.0.Results
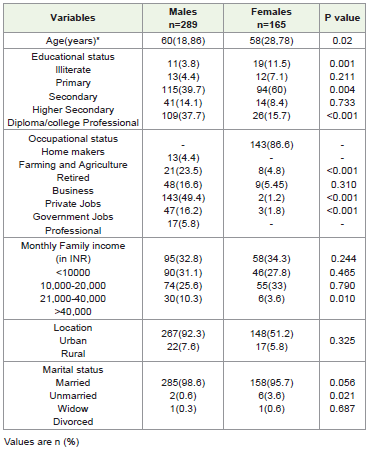
[Table 1] shows the socio demographic details of the study
participants. The median age was 60 and 58years respectively
in males and females. Majority of them were males (64%) and
females were 36%. Around 93.4% of males and females were
educated and only 6.6% were found to be illiterates. Majority
of the female participants(86.6%) were homemakers. Most of
the males (49.4%) were involved in private jobs by occupation.
Family income showed that 25.6% of males and 33% females
were earning monthly income of 20000-40000INR. Around 92.3%
of males and 51.2% of females were living in a urban location
whereas 7.6% of males and 5.8% of females were from rural
areas. [Table 1].
[Table 2] shows the anthropometric, blood pressure, clinical
and biochemical details of the study participants. Median weight
of male participants(70) was significantly higher than female
participants(66)(P=0.004). BMI was significantly higher in females
than males(P=0.001). Nearly 75% of females were overweight and
obese which was higher compared to males (68%). The median
duration of diabetes was similar in both gender. BP and GC
was also similar between males and females. Medication profile
shows that, 47% of the males and 42.4% of the females were
on oral hypoglycaemic agents (OHAs) respectively. 46.7% of the
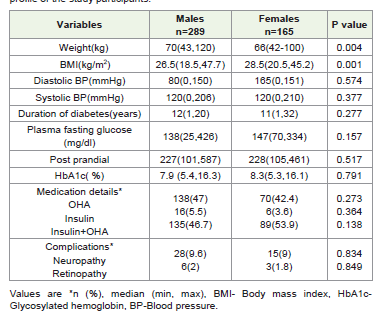
males and 53.9% of the females were on combination of insulin
and OHAs. Out of all, 9.6% and 2% of the males and 9% and
1.8% of the females were having diabetic complications such as
neuropathy and retinopathy respectively. [Table 2]
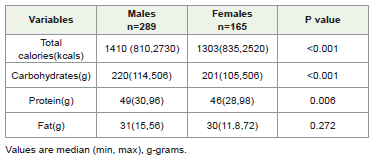
Table 3] shows the genderwise comparison of diet intake among the participants. The total calorie intake was significantly higher in males (1410kcals) as compared to females (1303kcals) (p<0.001). The consumption of complex carbohydrates(gms) (M:F;220:201) (p<0.001), protein (gms) (M:F;49:46) (P=0.006) was significantly higher in males than females. The fat consumption was similar in both the gender (M: F; 31:30gms) (P=0.272). [Table 3]
Table 3] shows the genderwise comparison of diet intake among the participants. The total calorie intake was significantly higher in males (1410kcals) as compared to females (1303kcals) (p<0.001). The consumption of complex carbohydrates(gms) (M:F;220:201) (p<0.001), protein (gms) (M:F;49:46) (P=0.006) was significantly higher in males than females. The fat consumption was similar in both the gender (M: F; 31:30gms) (P=0.272). [Table 3]
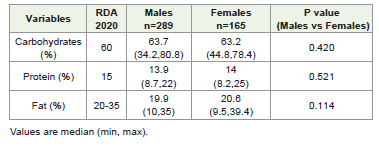
[Table 4] shows the comparison of gender wise macronutrient
distribution with recommended dietary allowances (RDA 2020)
among the study participants. The percentage of carbohydrate
intake was 63.7% in males and 63.2% in females. As per the RDA
recommendation it should be 60% but the percentage of the
carbohydrate intake was higher in both males and females (M:
F:63.7:63.2%). The percentage of protein intake was 13.9% in males
and 14% in females. RDA recommends 15%, however the protein
intake was lesser in both genders. The percentage of fat was 19.9%
in males and 20.6% in females. There was no difference found in the
percentage of fat consumption. [Table 4]
[Table 5] shows the lifestyle and dietary habits of the study
participants. Dietary habits showed that majority of the participants
were non-vegetarians (males-87.5%, females-90%). Most of the
males(62.6%) and females(56.3%) were doing regular exercise as
advised whereas 37.3% of the males and 43.6% of the female
participants were physically inactive. It was noticed that 68% of the
male participants do not consume food at regular timing whereas
83% of female participants were taking food at regular timing
which was statistically significant (P<0.001). A minor proportion
of participants (2.4%) only skip meals in both gender. Around
88.2% of the males and 75.7% of the females follow appropriate
meal schedule which was statistically significant (P=0.005). Among
all the participants, 85.8% of the males and 86.6% of the females
were taking adequate meal composition [Table 5].
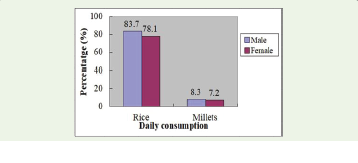
[Figure 1]-shows the gender-wise comparison of cereal intake
among the study participants. Assessment of food frequency
showed that, majority of males (83.7%) and females (78%) consume
rice daily while only few of them (8.3 vs.7.2%) consumes millets.
[Figure 2]-shows that, majority of the male participants were taking
milk daily than females (91.6 vs.80%;P=0.003). A majority of the
male participants were consuming pulses everyday than females
(67.8 vs.60%;P<0.001). Only 15.2% of males and 16.9% of females
were observed to consume green leafy vegetables everyday. 41% of
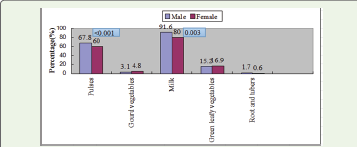
the male and 33.9% of the female participants were consuming
nuts daily. Majority of them were consuming sunflower oil (M: F 58.8
vs.53.3%) than any other source of oils in both the gender. The nonvegetarian
food consumption especially chicken without skin or fish
was consumed either once a week or twice a week. Daily egg white
consumption among the males was 17.9% whereas it was 19.3% in
females. Around 11.7% of males and 12.1% of females consumes
simple sugars every day.
Discussion
The present study highlights the gender differences of dietary
practices followed by people with T2DM. The majority of the
participants were educated and duration of diabetes was similar
in both gender. Half of the participants were on combination
therapy of OHA and insulin. The total calorie consumption was
higher in males than females. The carbohydrate and protein
intake was higher in males as compared to females but the fat
intake was similar in both the gender.
The dietary recommendations by ICMR, NIN [15] allow (55-60%)carbohydrate, (15%) protein and (20-35%)fat to keep diabetes under good control. Our study findings revealed that percentage of carbohydrate intake was higher in both males and females (M:F 63.7:63.2%) and protein intake was lesser in both gender(M:F 13.9:14%). The consumption of recommended level of good quality protein was only 5% among rural and 18% in urban region. Similarly, the consumption of carbohydrate percentage by individuals with T2DM was higher and the protein percentage was lesser in the study. In general, it was reported that proportion of population consuming more than recommended intake of cereals was 97.1% in rural and 68.8% in urban region [15].
The dietary recommendations by ICMR, NIN [15] allow (55-60%)carbohydrate, (15%) protein and (20-35%)fat to keep diabetes under good control. Our study findings revealed that percentage of carbohydrate intake was higher in both males and females (M:F 63.7:63.2%) and protein intake was lesser in both gender(M:F 13.9:14%). The consumption of recommended level of good quality protein was only 5% among rural and 18% in urban region. Similarly, the consumption of carbohydrate percentage by individuals with T2DM was higher and the protein percentage was lesser in the study. In general, it was reported that proportion of population consuming more than recommended intake of cereals was 97.1% in rural and 68.8% in urban region [15].
body size. Hypertension, diabetes and cholesterol levels were
found to be significantly related to dietary patterns [17]
. In our study, nearly 75% of females were overweight and obese as
compared to 68% of males. The median BMI was significantly
higher in females than males. Contrary to our finding, there was
no difference in the mean WHR and BMI of male and female
respondents in a study conducted in Madhya pradesh, India [18].
Another finding of the present study revealed that around
83.7% of males and 78% of females consume rice daily while only
few of them (male-8.3%,female-7.2%) consume millets. Similarly,
a India multicenter screening including a large sample size proved
that, consumption of rice is more across India as compared with
millets. The report also showed that staple food has significant
effect on blood glucose levels and anthropometric measurements
[19]. The present study revealed that daily consumption of pulses
among the male was 67.8% and among females it was 60% but
the quantity to be taken as per the RDA recommendation was
(pulses-90g/day) so that the protein needs will be met as per the
requirement. Similarly, shrivastav etal [20] reported that majority
of respondents consume pulses every day.
Lodha etal [18] reported that intake of green leafy vegetables was less. Our study also showed that only 15.2% of males and 16.9% of females consume green leafy vegetables every day which seems to be very less when compared with RDA [15]. As per ICMR NIN [15] guidelines, a person should include 350g of vegetables per day or to consume 3-5 serving of vegetables but in our study there was less consumption of vegetables on daily basis among both the gender.
Lodha etal [18] reported that intake of green leafy vegetables was less. Our study also showed that only 15.2% of males and 16.9% of females consume green leafy vegetables every day which seems to be very less when compared with RDA [15]. As per ICMR NIN [15] guidelines, a person should include 350g of vegetables per day or to consume 3-5 serving of vegetables but in our study there was less consumption of vegetables on daily basis among both the gender.
Overall, 91.6% of males and 80% of females consume milk
every day in our study. Similar to our finding lodha etal [18]
also revealed that majority of respondents consumed milk every day.
NIN guidelines recommend usage of different varieties of cooking
oils to obtain a variety of phytonutrients [15]
but the present study revealed that majority of them consume sunflower oil than
any other source of oil.
The lodha etal [18] revealed that 27 participants used sugars daily whereas in our study 34 male and 20 female participants consume sugars every day. In general, a varied diet with HF fruits, vegetables, pulses and nuts was associated with better health outcomes. Inspite of imparting education on dietary practices and dietary recommendation at every follow-up visit to the clinic, there was an imbalance in their nutrient intake in our participants. Only 32% of our male participants reported that they consume food at regular timing whereas 83% of female participants consume food on time. The level of PA was lesser in females than males (56.3% vs.62.6%), only 2.4% of them skip meals in both gender. Majority of them follow appropriate meal schedule (males-88.2%,females-75%) and meal composition (males-85.8% ,females-86.6%).
The lodha etal [18] revealed that 27 participants used sugars daily whereas in our study 34 male and 20 female participants consume sugars every day. In general, a varied diet with HF fruits, vegetables, pulses and nuts was associated with better health outcomes. Inspite of imparting education on dietary practices and dietary recommendation at every follow-up visit to the clinic, there was an imbalance in their nutrient intake in our participants. Only 32% of our male participants reported that they consume food at regular timing whereas 83% of female participants consume food on time. The level of PA was lesser in females than males (56.3% vs.62.6%), only 2.4% of them skip meals in both gender. Majority of them follow appropriate meal schedule (males-88.2%,females-75%) and meal composition (males-85.8% ,females-86.6%).
Limitation:
In this study, only 24hour diet recall was used to assess the
dietary pattern and proximate principles of calorie, carbohydrate
protein and fat was calculated, but not fiber, vitamins and
minerals intake which has to be focused in future studies. This
study was conducted in a tertiary care centre, thus we cannot
generalize the findings.Conclusion
The level of protein consumption was lesser than required
amount among people with T2DM as per recommended
dietary allowance. Green leafy vegetables and other vegetables
consumption was lesser among the participants. Intensive diet
counselling should be focused on the amount of green leafy
vegetables and other vegetables to be taken per day and protein
rich foods to meet the requirements.
Acknowledgments
We thank Dr. Arutselvi.D for her help in designing the study
and Renuga, Sharon, Prabha, Nandhini, Thanuja dietitians for
their help in data collection for this study.
References
Citation
Janakiraman UM, Kumpatla S, Viswanathan V. Gender Differences in Dietary Practices among People with Type 2 Diabetes. A Study from South India. Indian J Nutri. 2026;13(1): 335.