Research Article
Socio-Demographic Determinants of the Combined Iron-Folate Deficient intake among Mothers and Children’s Dietary Diversity: A Cross-Sectional Study
Sultana A¹*, Betsy A², Rastogi P¹, Choudhary S¹ and Sharma S¹
1Department of Maternal, Newborn and Child Health and Nutrition, MAMTA Health Institute for Mother and Child, New Delhi.
2Nutrition Sciences, ITC Foods Business Division, ITC Limited, Bengaluru
2Nutrition Sciences, ITC Foods Business Division, ITC Limited, Bengaluru
*Corresponding author:Ms. Afreen Sultana, Department of Maternal, Newborn and Child Health and Nutrition, MAMTA Health Institute for Mother and Child, B-5, Greater Kailash Enclave II, Delhi-110048. E-mail Id: afreen@mamtahimc.in
Article Information:Submission: 17/09/2025; Accepted: 10/10/2025; Published: 14/10/2025
Copyright: © 2025 Sultana A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Micronutrient-related malnutrition is a common public health problem in India, with most pregnant mothers consuming less than 50% of the recommended daily allowances of nutrients. Under-5 dietary diversity is equally poor, with 90% of them consuming less than 4 food groups a day. However,
there is a lack of research on the determinants of dual iron and folate deficiencies and under-5 dietary diversity among socially vulnerable populations. The study aimed to assess the prevalence of iron and folic acid deficiencies among pregnant, lactating, and non-pregnant, non-lactating (NPNL) women, the
dietary diversity score of children, and identify socio-demographic and anthropometric predictors associated with them.
Methods: It had a cross-sectional quantitative research study design. The study was conducted in the Valsad block of the Valsad district, Gujarat, India. We adopted a multi-stage random sampling to collect data using a semi-structured pre-validated questionnaire. We employed the logistic and Poisson regression techniques to find associations between predictors and the categorical outcome. The strength and the significance of the association were expressed as adjusted Odds Ratio (aOR) or Incident Rate Ratio (IRR) and 95% Confidence Interval (CI), and a p-value.
Results: A total of 1097 women were surveyed. The median (Interquartile Range, IQR) age of the women was 27 (25-30) years. The median (IQR) age of the child was 17 (32-45) months. Compared to the NPNL women, pregnant and lactating mothers had 1.29 higher odds of both iron and folate deficient intake (OR (95%CI); p-value: 1.289 (1.007, 1.570); <0.001). One kg increase in the weight of the child was associated with 2% increase in the dietary diversity score (IRR (95%CI); p-value: 1.003 (1.0007, 1.006); 0.01).
Conclusions: Women are deficient in most micronutrients, and pregnant women and lactating mothers are at a higher risk of dual iron-folate deficiencies.
Methods: It had a cross-sectional quantitative research study design. The study was conducted in the Valsad block of the Valsad district, Gujarat, India. We adopted a multi-stage random sampling to collect data using a semi-structured pre-validated questionnaire. We employed the logistic and Poisson regression techniques to find associations between predictors and the categorical outcome. The strength and the significance of the association were expressed as adjusted Odds Ratio (aOR) or Incident Rate Ratio (IRR) and 95% Confidence Interval (CI), and a p-value.
Results: A total of 1097 women were surveyed. The median (Interquartile Range, IQR) age of the women was 27 (25-30) years. The median (IQR) age of the child was 17 (32-45) months. Compared to the NPNL women, pregnant and lactating mothers had 1.29 higher odds of both iron and folate deficient intake (OR (95%CI); p-value: 1.289 (1.007, 1.570); <0.001). One kg increase in the weight of the child was associated with 2% increase in the dietary diversity score (IRR (95%CI); p-value: 1.003 (1.0007, 1.006); 0.01).
Conclusions: Women are deficient in most micronutrients, and pregnant women and lactating mothers are at a higher risk of dual iron-folate deficiencies.
Keywords:Food quality; diet; nutrients; anemia; diet diversity
Introduction
Micronutrient-related malnutrition [1] is an alarming public
health challenge globally, with India bearing a high burden,
disproportionately. As per the National Family Health Survey-5
(NFHS-5) report, more than 50% of both pregnant and non-pregnant
women were found to be anemic [2], and the status of anaemia among
pregnant women who consumed iron folic acid tablets for 100 days
and 180 days or more was 44% and 26%, respectively. There are
variations within the states and districts related to the prevalence of
anemia. For example, while the prevalence of anemia was between 62-
65% among women in Gujarat, it was more than 70% in the Valsad
district of Gujarat, across all age groups, including pregnant women
and children under 5 years of age [3].
The first 1,000 days of life, which is a period from conception till
over 2 years of life, are considered extremely crucial for development
[4]. Malnutrition of any form in this stage can cause irreversible brain
damage and delay physical growth and cognitive development [5].
Iron deficiency is the biggest contributor to anaemia in pregnancy,
which, when left untreated, causes long-term damage to maternal
and new-born health. Daily oral supplementation of a combination
of iron and folic acid (IFA) is the most cost-effective intervention to
reduce iron deficiency anaemia in pregnancy [6].
Both quantity and quality of dietary intake are crucial to address
for reducing malnutrition. Dietary diversity is an established
qualitative measure reflecting household access to a variety of foods.
Being short and easy to obtain, it acts as a proxy tool to measure
the micronutrient adequacy [7]. Higher dietary diversity leads to
improved nutritional outcomes of children. Children in the rural
areas and high-focus regions are at a higher risk of dietary diversity
failure [8]. Furthermore, dietary diversity failure is associated with
low fruit, vegetable, and protein-rich food consumption [9].
Children’s dietary diversity is quite low in India, especially in
rural areas [10]. Nearly 90% of under-5 children consume less than
4 food groups a day. The inadequate dietary diversity significantly
increases the risk of stunting, wasting, and underweight among
under-5 children [11]. There is empirical evidence that a high dietary
diversity is associated with micronutrient adequacy in infants and
children under 5 years old [12]. Likewise, most pregnant mothers
have less than 50% of the recommended dietary intakes of iron (98%)
and folate (89%) [13].
There are multiple efforts taken by the government to address
micronutrient deficiencies, such as POSHAN Abhiyaan, Integrated
Child Development Services (ICDS), Mid-Day Meal (MDM) scheme,
Food fortification (+F), etc. [14]. However, to tackle the issue of
anemia holistically, there is still a need to understand the specific
gaps in the dietary practices of women of reproductive age to assess
the predictors of IFA and other micronutrient deficiencies. Dietary
diversity is a validated proxy indicator of micronutrient adequacy
among different age groups, including infants, children, and women
[15].
Identifying the need to address these gaps, a cross-sectional exploratory study was conducted in the Valsad district of Gujarat across 51 villages. The study aimed to assess the prevalence of IFA deficiencies among pregnant, lactating, and non-pregnant, nonlactating (NPNL) women, the dietary diversity score of children, and identify socio-demographic and anthropometric predictors associated with these deficiencies and dietary diversity scores, respectively. The project aimed at assessing the predictors of combined iron-folatedeficient intake, with the predictors of deficient intake of either or none.
Identifying the need to address these gaps, a cross-sectional exploratory study was conducted in the Valsad district of Gujarat across 51 villages. The study aimed to assess the prevalence of IFA deficiencies among pregnant, lactating, and non-pregnant, nonlactating (NPNL) women, the dietary diversity score of children, and identify socio-demographic and anthropometric predictors associated with these deficiencies and dietary diversity scores, respectively. The project aimed at assessing the predictors of combined iron-folatedeficient intake, with the predictors of deficient intake of either or none.
Methods
Study design:
A cross-sectional design was adopted, and quantitative research
was conducted.Study settings:
The study was conducted in the Valsad block of the Valsad district,
Gujarat. There are 85 villages in the Valsad block of the Valsad district
of Gujarat. The mean population of the villages is 2620. We conducted
the survey in 41 villages of the Valsad block.Study Population:
It included under-5 children and their mothers and pregnant
women (irrespective of gender, caste, color, and religion).Inclusion criteria:
• Under-5 children (6-59 months) residing in the areas for at
least the past 6 months and planning to reside in the same
area for 6 months• Mothers of under-5 children residing in the areas for at least the past 6 months and planning to reside in the same area for 6 months (their in-laws’ side)
• Pregnant women residing in the areas for at least the past 6 months and planning to reside in the same area for 6 months or 1 year
Exclusion criteria:
All those who did not provide consent or assent (for adolescent
mothers), had suffered a major illness in the past 6-12 months, or had
any physical deformity or genetic abnormality.Sample size:
The sample size was 768 (~800) under-5 children and 300
pregnant women.Sampling:
We adopted a multi-stage random sampling. We recruited
children from 1000 eligible households spread across 51 villages.
Fifty-one villages having more than 250 households were selected
randomly from the Valsad block, and approximately 50 households
were selected per village, for a total of approximately 250 households.
We started from the center of the village, and after having selected
the first house, we went in the clockwise direction (right side), and
each qualifying household was interviewed till the desired sample
size was achieved, i.e., 50 children under-5 and their mothers. One
of the youngest under-5 children and his/her mother were selected
per household. In the case of a boy and a girl of the same age, the girl
was selected due to the evidence of their increased susceptibility to
malnutrition. In the case of twins, we randomly selected one. If we
could not meet our number, we moved to the adjacent village.Study tools:
• The semi-structured pre-validated questionnaire [16]
consisted of questions on the socio-demographic profile of
the study participants, i.e., age, sex, educational status, size
of the family, type of the family, monthly family income, and
occupational status. We also asked about the presence of
ration cards in the households, such as the below the poverty
line (BPL) card, Antayodya Anna Yojna (AAY) card, etc. [17].• The questionnaire for children included an assessment of the nutritional status of children: weight (measured to the nearest 100g on the weighing scale), height (measured to the nearest 1mm), mid-upper arm circumference (by a tape to the nearest 0.1cm), and 24-hour dietary recall.
• The questionnaire for mothers included questions on
anthropometric measurements (weight, height, Mid-Upper
Arm Circumference (MUAC), and dietary practices, and the
last 24-hour recall. Training of the field team was conducted
on the developed questionnaire.
• The dietary diversity score was assessed using the following 8 food groups, including 1) grains, white roots and tubers, and plantains, 2) pulses (beans, peas, and lentils), nuts and seeds, 3) dairy, 4) meat, poultry, and fish, 5) eggs, 6) dark green leafy vegetables, 7) other vitamin A-rich fruits and vegetables, and 8) other vegetables, and other fruits. The score ranges from 0 to 8, expressed as an average score for the population, with a higher score indicating inclusion of more food groups in the diet.
• We assessed the dietary intake of ten micronutrients among mothers, including iron, calcium, vitamin D (Ergocalciferol), vitamin C, vitamin A, vitamin E, zinc, and folic acid. A 24-hour dietary recall was performed to generate the dietary diversity score, which included the assessment of 8 food groups and intake of micronutrients, including IFA. The dietary intake of micronutrients less than the recommended dietary allowance (RDA) was categorised as insufficient intake according to the ICMR 2024 criteria [18]. Additionally, the dietary diversity scores among children aged 6–59 months were also examined to explore their relationship with anthropometry indicators and socio-demographic factors.
• The dietary diversity score was assessed using the following 8 food groups, including 1) grains, white roots and tubers, and plantains, 2) pulses (beans, peas, and lentils), nuts and seeds, 3) dairy, 4) meat, poultry, and fish, 5) eggs, 6) dark green leafy vegetables, 7) other vitamin A-rich fruits and vegetables, and 8) other vegetables, and other fruits. The score ranges from 0 to 8, expressed as an average score for the population, with a higher score indicating inclusion of more food groups in the diet.
• We assessed the dietary intake of ten micronutrients among mothers, including iron, calcium, vitamin D (Ergocalciferol), vitamin C, vitamin A, vitamin E, zinc, and folic acid. A 24-hour dietary recall was performed to generate the dietary diversity score, which included the assessment of 8 food groups and intake of micronutrients, including IFA. The dietary intake of micronutrients less than the recommended dietary allowance (RDA) was categorised as insufficient intake according to the ICMR 2024 criteria [18]. Additionally, the dietary diversity scores among children aged 6–59 months were also examined to explore their relationship with anthropometry indicators and socio-demographic factors.
Ethical considerations:
The ethical approval was obtained from SIGMA-Institutional
Ethical Review Board (10095/IRB/22-23).Statistics:
The categorical data were described as frequencies and percentages,
and the numerical data were described as mean (Standard Deviation)
or median (Interquartile Range, IQR). We created two new variables
by combining iron and folate deficiencies. Thereby, one variable had
two categories, including ‘either or none’ iron and folate deficiencies
and ‘both’ iron and folate deficiencies. Likewise, the other variable
included three categories: ‘either, none, or both’ iron and folate
deficiencies.We employed the logistic regression technique to find associations between predictors and the categorical outcomes. The strength and the significance of the association were expressed as adjusted Odds Ratio (aOR) and 95% Confidence Interval (CI), and a p-value. We used the Poisson regression technique to explore associations between predictors of the infant dietary diversity. The strength of the relationship was expressed as Incident Rate Ratio (IRR) and 95% CI. We did not use the occupation of the mother in the dietary diversity model of children, as there was not much variation in the dataset, since 92% of mothers were housewives. All the analyses were performed in STATA version 14.0. A p-value <0.05 was considered a statistically significant value.
Results
The data were collected in the Valsad block of the Valsad district
of Gujarat. We collected data from 51 villages. A total of 1097 women
were surveyed. Out of 1097, 586 were pregnant and lactating women,
and 511 were non-pregnant and non-lactating women. The median
(IQR) age of the women was 27 (25-30) years. Out of 1097 women,
276 had no children, 765 had one child between 6 and 59 months, and
56 had two children between 6 and 59 months. Out of 821 children,
405 were boys and 416 were girls.
The median (IQR) age of the child was 17 (32-45) months. The median age of the eldest child was 37 (47-54) months. Out of 56 eldest children, 25 were boys and 31 were girls. The median (IQR) weight and height of the children were 11 (9-13) kg and 87 (75-95) cm, respectively. Similarly, the median (IQR) MUAC of the children was 14.5 (13.5-15) cm. The median (IQR) dietary diversity score among children was 5 (4-8). Nearly 21% of children had less than 50% of the maximum dietary diversity (<4 food groups per day out of 8).
Out of 1097 mothers, 133 were either illiterate or educated between 1st and 8th standard, 799 were educated between 9th and 12th standard, and the remaining 165 were educated up to graduation or above. Out of 1097, 1008 were housewives and 89 were working mothers. Out of 1097, 174 were living in a nuclear family, while 923 were living in a joint or extended family. The median (IQR) weight and height of the mothers were 52.7 (45.1, 60.8) kg and 152 (149, 154.5) cm, respectively. Out of 1097, 610 were above the poverty line, 459 had BPL or AAY cards, and the remaining 28 had no cards. The median (IQR) size of the family was 5 (4-6). The median (IQR) monthly family income was 15k (10k-25k).
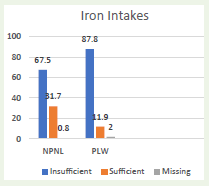
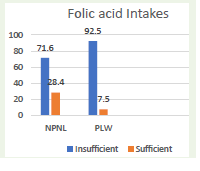
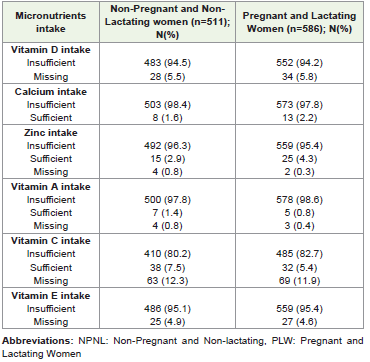
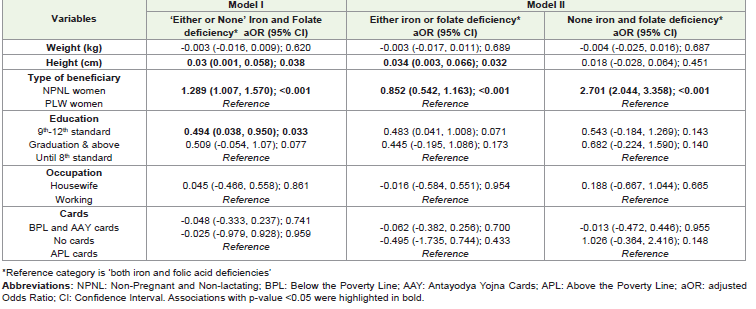
All women had insufficient vitamin D and E intake [Table 1]. Around 67% of NPNL and 88% of the pregnant and lactating women had deficient iron intake [Figure 1]. Likewise, 71% of the NPNL women and 92% of pregnant and lactating women had deficient folate intake [Figure 2]. The pregnancy has emerged as a major predictor of insufficient intake [Table 2]. Compared to the NPNL women, pregnant and lactating mothers had 1.29 higher odds of ‘both iron and folate’ deficient intake (OR (95%CI); p-value: 1.289 (1.007, 1.570); <0.001). Similarly, taller and educated women had a higher probability of ‘either or none’ iron-folate deficient intake than their counterparts.
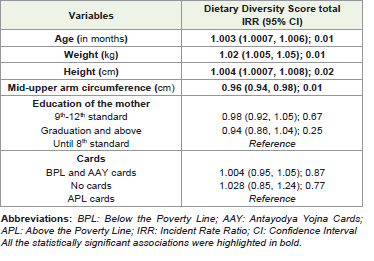
A positive association between weight and height of the child was noted with their dietary diversity scores [Table 3]. One kg increase in
The median (IQR) age of the child was 17 (32-45) months. The median age of the eldest child was 37 (47-54) months. Out of 56 eldest children, 25 were boys and 31 were girls. The median (IQR) weight and height of the children were 11 (9-13) kg and 87 (75-95) cm, respectively. Similarly, the median (IQR) MUAC of the children was 14.5 (13.5-15) cm. The median (IQR) dietary diversity score among children was 5 (4-8). Nearly 21% of children had less than 50% of the maximum dietary diversity (<4 food groups per day out of 8).
Out of 1097 mothers, 133 were either illiterate or educated between 1st and 8th standard, 799 were educated between 9th and 12th standard, and the remaining 165 were educated up to graduation or above. Out of 1097, 1008 were housewives and 89 were working mothers. Out of 1097, 174 were living in a nuclear family, while 923 were living in a joint or extended family. The median (IQR) weight and height of the mothers were 52.7 (45.1, 60.8) kg and 152 (149, 154.5) cm, respectively. Out of 1097, 610 were above the poverty line, 459 had BPL or AAY cards, and the remaining 28 had no cards. The median (IQR) size of the family was 5 (4-6). The median (IQR) monthly family income was 15k (10k-25k).
All women had insufficient vitamin D and E intake [Table 1]. Around 67% of NPNL and 88% of the pregnant and lactating women had deficient iron intake [Figure 1]. Likewise, 71% of the NPNL women and 92% of pregnant and lactating women had deficient folate intake [Figure 2]. The pregnancy has emerged as a major predictor of insufficient intake [Table 2]. Compared to the NPNL women, pregnant and lactating mothers had 1.29 higher odds of ‘both iron and folate’ deficient intake (OR (95%CI); p-value: 1.289 (1.007, 1.570); <0.001). Similarly, taller and educated women had a higher probability of ‘either or none’ iron-folate deficient intake than their counterparts.
A positive association between weight and height of the child was noted with their dietary diversity scores [Table 3]. One kg increase in
the weight of the child was associated with 2% increase in the dietary
diversity score (IRR (95%CI); p-value: 1.003 (1.0007, 1.006); 0.01).
Discussion
The present study revealed a high prevalence of micronutrient
deficiencies among women in the Valsad district of Gujarat, which
is consistent with the national-level data highlighting widespread
iron deficiency anemia and micronutrient inadequacies among
women of reproductive age in India. Notably, 87.8% of pregnant and
lactating women were iron-deficient, and 92.5% had insufficient folic
acid intake, compared to 67.5% and 71.6% among NPNL women,
respectively. Non-compliance in IFA intake among pregnant women
was indicated in a study by Choudhuri, et al. 2022, where, nearly half
of the pregnant women had non-compliant intake of IFA, and major
reasons included forgetfulness and fear of side effects [19]. These
findings emphasize the persistent gap between increased nutritional
requirements during pregnancy and actual intake.
Due to the increased requirements of IFA, pregnant women are
at a high risk of IFA deficiency [20]. This analysis provided a similar
conclusion, as it identified pregnancy status as a significant predictor
of combined IFA deficiency, indicating that pregnant and lactating
women were more likely to suffer from dual deficiencies compared to
NPNL women, underscoring the urgent need to strengthen maternal
nutrition programs, including access to supplements, nutrition
counselling, and food-based interventions.
Height was significantly associated with reduced odds of dual
deficiency when compared to being deficient in just one, which
may reflect long-term nutritional status rather than short-term
intake. There was no significant association between height and
being completely free from IFA deficiency. Education level showed
a protective trend against deficiencies, especially among women
educated up to 9th–12th standard, although associations were
marginally significant. This finding suggests that even though it
may not eliminate the risk, but a higher level of education reduces
the chances of having dual deficiency. This result aligns with a study
by Sandri et al. 2024, which concludes that education level is of
fundamental importance for health, particularly for nutritional habits
[21].
Predictors of dietary diversity scores among children aged
6-59 months were identified using Poisson regression analysis.
Anthropometric factors such as age, weight, and height were
positively associated with dietary diversity, suggesting that older and
better-nourished children tend to consume food from more groups,
indicating improved dietary quality. Similar findings have been
concluded by Khura B et al. 2024, where Minimum Dietary Diversity
(MDD) had a positive association with underweight in children aged
6 to 23 months. Their results showed that children with adequate
MDD had 9% less likelihood of being underweight than those with
inadequate MDD [22]. However, a negative association was observed
between MUAC and dietary diversity, suggesting that some children
are consuming a high-calorie diet, which is not balanced and diverse.
Maternal education and household economic status, as measured by
ration card ownership, were not significantly associated with child
dietary diversity in this population. These findings highlight the
importance of looking beyond household poverty to understand
dietary quality in young children and suggest that nutrition
interventions may need to focus on improving both the quantity and
quality of foods offered.
Overall, the observations highlight the need for targeted nutritional
interventions addressing specific vulnerabilities of pregnant and
lactating women owing to higher nutritional needs and increased
risks of dual deficiencies. The interventions can be strategized as a
holistic approach that includes improving the quality of maternal
diets through food-based approaches, education interventions on
the importance of IFA supplementation, and promoting diversified
complementary feeding practices for young children. Such efforts are
essential to mitigate the burden of micronutrient deficiencies among
vulnerable populations, such as pregnant, lactating women, and
children under 5 years of age.
The results of the present study should be interpreted in view of
certain limitations. The study was done in a small geographical area
(Valsad block), and the findings may not be generalized to other
geographies. The 24h recall had its own limitations of recall bias.
Though efforts were made to minimize the error by deeply probing
the intakes. We did not obtain other antenatal, postnatal, and infant
indicators that could have been adjusted in the regression models due
to lack of resources and time. However, the study has its strengths.
We analysed the dual IFA deficient intake and assessed its predictors
based on a relatively adequate sample of 1097 women. We used
the standard and pre-validated tools for obtaining data from the
participants. The data were collected by the local investigators who
could speak the local dialect.
Conclusions
Inadequate intake of most micronutrients is widely prevalent
among mothers, irrespective of their pregnancy status. However,
pregnancy exaggerates the deficiencies due to the increased demand,
leading to a vicious cycle of malnutrition across generations. Under-5
dietary diversity failure is common and one-fifth of the children
consume less than 4 food groups per day. Within the household,
mother and the child may have different nutritional intakes and
statuses. Hence, family-centric approach is required while assessing
the nutritional intakes of the key vulnerable populations.
References
Citation
Sultana A, Betsy A, Rastogi P, Choudhary S, Sharma S. Socio-Demographic Determinants of the Combined Iron-Folate Deficient intake among Mothers and Children’s Dietary Diversity: A Cross-Sectional Study. Indian J Nutri. 2025;12(2): 327.