Case Report
Management of Atopic Dermatitis and Food Allergies in a Two-Year-Old Girl: A Case Report
Kour H1 and Kannan SS2*
1Department of Physiology, Jawaharlal Nehru Medical College Belagavi, Karnataka, India
2Department of Community Medicine, ESIC Medical College and Hospital, Chennai, Tamil Nadu, India
2Department of Community Medicine, ESIC Medical College and Hospital, Chennai, Tamil Nadu, India
*Corresponding author:Dr Suthanthira Kannan S, Department of Community Medicine, ESIC Medical College and Hospital, Chennai, Tamil Nadu, India. E-mail Id: gurudixitkannan@gmail.com
Article Information:Submission: 15/08/2025; Accepted: 30/08/2025; Published: 04/09/2025
Copyright: © 2025 Kour H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
A two-year-old girl with refractory atopic dermatitis and multiple food allergies presented with elevated serum IgE (605 IU/mL). A six-week multidisciplinary intervention incorporating allergen elimination and nutritionally adequate dietary alternatives led to marked clinical improvement and reduction in IgE to 150 IU/mL. Most allergens could be reintroduced except milk. This case demonstrates that structured nutritional therapy, guided by a multidisciplinary team, can effectively manage pediatric atopic dermatitis associated with food allergies.
Introduction
Atopic dermatitis (AD) is one of the most burdensome chronic
inflammatory skin diseases of early childhood, marked by intense
pruritus, sleep disruption, and recurrent eczematous flares. Globally
affecting up to 30% of children, AD poses a particularly significant
challenge in low- and middle-income countries like India, where
increasing urbanisation and lifestyle shifts have fuelled a rise in
atopic diseases. Approximately one-third of children with moderateto-
severe AD have co-existing food allergies, most commonly to
cow’s milk, egg, and soy in infancy, progressing to wheat, fish, and
tree nuts with age. [1,2] Diagnosis integrates clinical history, serum
IgE, skin prick testing, and confirmation via elimination diets or oral
food challenges. Targeted dietary avoidance remains a cornerstone
of management when food triggers are identified. This case report
highlights a successful multidisciplinary approach in a two-year-old
girl with AD and multiple food allergies, emphasising the role of
structured nutritional therapy in improving clinical outcomes in the
Indian context.
Case Presentation
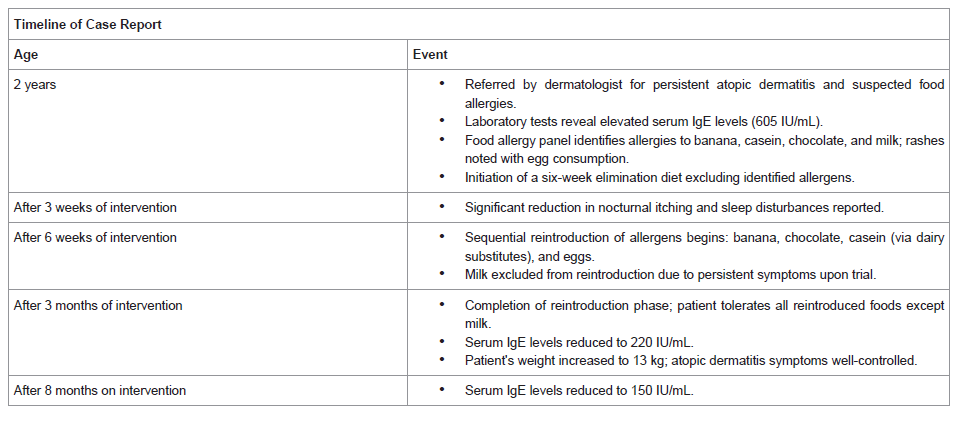
A two-year-old girl (weight: 9.2 kg) was referred by a
dermatologist for persistent atopic dermatitis characterised by severe
nocturnal pruritus and frequent crying episodes, often requiring her
parents to scratch her entire body for relief. Initial laboratory workup
showed markedly elevated serum total IgE (605 IU/mL). Given
the suspected food-related exacerbations, a food allergy panel was
performed, which revealed sensitivities to banana, casein, chocolate,
and milk. Although there was no history of milk intolerance in the
first year of life, parents reported the onset of rashes following milk
and egg consumption during the current presentation, supporting
the role of food allergens in symptom aggravation.
Management:
The dietary management of the patient was designed using
evidence-based guidelines for food allergy and atopic dermatitis:1. Elimination Phase: A six-week elimination diet was initiated
to exclude all identified allergens (banana, casein, chocolate,
milk, and eggs) from the patient’s diet. This phase was grounded
in recommendations from the European Academy of Allergy
and Clinical Immunology (EAACI), which advocate for allergen
elimination to reduce inflammatory responses.[3]
Nutritional adequacy was ensured using the following allergen free
substitutes:
• Soy milk – protein-rich and nutritionally balanced, widely
recommended for children with cow’s milk allergy (CMA).
• Oat milk – low-allergen and fibre-containing (β-glucan),
increasingly recognised as a well-tolerated option in
paediatric populations.[4]
• Ragi (finger millet) milk – naturally high in calcium, iron,
and essential amino acids, providing bone and micronutrient
support in plant-based diets.
• Homemade allergen-free meals – based on fresh fruits,
vegetables, and whole grains to ensure adequate vitamins,
minerals, and antioxidants while reducing exposure to
processed food allergens; parents were counselled on safe
preparation techniques.
2. Symptom Monitoring and Sleep Quality Assessment:
Weekly follow-ups were conducted to monitor improvements in
skin symptoms and sleep quality. Sleep quality was evaluated using
a modified Sleep Disturbance Scale for Children (SDSC), which has
been validated in pediatric populations. Scores indicated a significant
reduction in nocturnal itching and sleep disruption by the third week
of dietary intervention.[5]
The patient’s mother reported marked symptom relief,
corroborating findings in the existing literature on elimination diets
and their impact on AD-related sleep disturbances.
3. Reintroduction Phase: Starting in week seven, allergens
were reintroduced sequentially in controlled doses, following
protocols described by Sicherer and Sampson (2018) for graded
food reintroduction. Foods were reintroduced in order of increasing
allergenicity: banana, chocolate, casein (via dairy substitutes), and
eggs.[6]
Milk was excluded from reintroduction due to persistent symptoms upon trial, consistent with findings that CMA often persists longer than other food allergies in children.
Milk was excluded from reintroduction due to persistent symptoms upon trial, consistent with findings that CMA often persists longer than other food allergies in children.
4. Parental Education and Long-Term Dietary Strategies:
Parents were provided with evidence-based guidelines on avoiding
cross-contamination and recognizing early signs of allergic reactions.
Research from Burks et al. (2012) highlights the importance of
caregiver education in improving dietary adherence and outcomes.
[7]
A balanced diet plan was devised to ensure continued growth and nutritional adequacy while avoiding high-risk allergens.
Outcomes: By the end of the intervention, the child’s weight had increased to 13 kg. Her atopic dermatitis symptoms were well controlled, IgE levels reduced to 150 IU/mL, and she could tolerate most previously identified allergens except milk. These results align with studies demonstrating improved growth and symptom management through tailored elimination and reintroduction strategies.
A balanced diet plan was devised to ensure continued growth and nutritional adequacy while avoiding high-risk allergens.
Outcomes: By the end of the intervention, the child’s weight had increased to 13 kg. Her atopic dermatitis symptoms were well controlled, IgE levels reduced to 150 IU/mL, and she could tolerate most previously identified allergens except milk. These results align with studies demonstrating improved growth and symptom management through tailored elimination and reintroduction strategies.
Discussion
Atopic dermatitis (AD) with co-existing food allergies poses a
multifaceted challenge where inappropriate dietary restriction risks
malnutrition, while uncontrolled allergen exposure aggravates disease
severity. While this case demonstrates successful implementation
of a structured elimination and reintroduction diet, it is imperative
to recognise that elimination diets are not universally effective.
Several studies have reported failure rates ranging from 40% to
70%, particularly when empirical elimination (without confirmed
allergen testing) is employed.[9] In such instances, despite strict food
avoidance, patients continue to experience pruritus and eczematous
flares, likely due to non-dietary triggers (e.g., aeroallergens, infections,
stress, and climatic factors) or unavoidable cross-contamination.
Long-term restrictive diets may also inadvertently induce sensitisation
or increased reactivity upon re-exposure — a phenomenon described
in delayed tolerance acquisition, particularly with egg and peanut
allergens.
Additionally, elimination diets may negatively affect growth and
development if not accompanied by dietetic supervision. Reports of
growth faltering, micronutrient deficiencies (vitamin D, calcium,
iron), and reduced bone mineral density have been documented,
especially in children maintained on prolonged cow’s-milk- and eggfree
regimens without adequate substitutes. This case underscores
the importance of integrating nutrient-dense alternatives (soy, oat,
ragi milks) to maintain caloric and micronutrient sufficiency during
exclusion phases.
The strategic use of such substitutes allowed the patient to
achieve catch-up growth while maintaining allergen avoidance.
The psychosocial impact of AD is often under-recognised. Severe
nocturnal itching leads to sleep deprivation in both child and
parents, contributing to behavioural problems such as irritability,
attention deficits, and poor feeding. Parents frequently report
emotional exhaustion, guilt, and anxiety over dietary choices and
fear of inadvertent allergen exposure. Social constraints, including
avoidance of gatherings, playdates, or preschool interactions, can
impede normal childhood experiences. Furthermore, rigid meal
preparation requirements and concern over cross-contamination
create substantial caregiver stress, sometimes resulting in maladaptive
feeding practices or strained family dynamics. In this case, the
multidisciplinary team actively incorporated caregiver counselling
and practical education on allergen-free meal preparation to reduce
these psychosocial burdens. Therefore, Empowering caregivers
through dietary guidance, psychological support, and practical
strategies is therefore critical for sustaining long-term management
and enhancing overall quality of life.
Validated tools such as the Sleep Disturbance Scale for Children
(SDSC), Dermatology Life Quality Index (DLQI), and Parent-
Reported Quality of Life (PRQL) questionnaires can be used
longitudinally to capture these broader outcomes, allowing clinicians
to tailor interventions more holistically.
Ultimately, long-term management should aim for balance:
strict avoidance of confirmed allergenic foods during active disease
while avoiding unnecessary dietary restriction. Gradual controlled
re-exposure under supervision (tolerance induction approaches)
may facilitate immune modulation for certain allergens such as egg
and peanut. Empowering caregivers through education, access to
nutritionists, and psychological support is crucial to ensure adherence
and reduce distress. Continued research into biomarkers predicting
dietary response would enable more personalised dietary strategies,
thereby improving both clinical and quality-of-life outcomes in
children with AD and food allergies.
Conclusion
The successful resolution of symptoms in this patient
demonstrates the efficacy of personalized, evidence-based dietary
strategies in managing pediatric AD with associated food allergies.
Further studies are warranted to explore long-term outcomes and
refine approaches to gradual allergen reintroduction.
Acknowledgments
We thank the patient’s family for their cooperation and the
dermatologist for their ongoing involvement in the patient’s care.
References
Citation
Kour H, Kannan SS. Management of Atopic Dermatitis and Food Allergies in a Two-Year-Old Girl: A Case Report. Indian J Nutri. 2025;12(2): 324.