Research Article
Determinants of Initiation of Breastfeeding: A Cross-Sectional Study
Gohiya P1* and Sonkar R2
1Department of Pediatrics, GMC, Bhopal, Madhya Pradesh, India
2Department of Pediatrics, PGMO District Hospital Raisen, Madhya Pradesh, India
2Department of Pediatrics, PGMO District Hospital Raisen, Madhya Pradesh, India
*Corresponding author:Dr Poorva. Gohiya, Department of Pediatrics, GMC, Bhopal, Madhya Pradesh, India. E-mail Id: gohiyapoorva@gmail.com
Article Information:Submission: 09/07/2025; Accepted: 12/08/2025; Published: 15/08/2025
Copyright: © 2025 Gohiya P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Breastfeeding is essential for the well-being of infants as well as mothers, providing numerous health benefits and promoting bonding. [1]However, improper breastfeeding practices contribute to neonatal mortality, accounting for significant proportion of child deaths under five. This study aims to investigate factors associated with initiation of breastfeeding.
Methods: This hospital-based cross-sectional study was conducted over a period of one year, involving 500 mothers-neonate dyads, admitted in the postnatal ward. Socioeconomic and maternal factors, including maternal stress, were assessed using the Perceived Stress Scale (PSS) and the Edinburgh Postnatal Depression Scale (EPDS) [2]. Early initiation of breastfeeding was defined as breastfeeding starting within one hour of birth.
Results: Majority of mothers (71.8%) were aged 18-25 years and resided in urban areas (66.6%). Most mothers (88.2%) were housewives. Maternal stress assessment revealed that 73% had low stress, and 82.6% did not report any depression. Maternal age, parity, delivery mode, pregnancy complications, and pain interfering with breastfeeding were associated with delayed initiation of breastfeeding. On multivariate analysis, cesarean section (LSCS) and pain (various reasons) were the two main factors which contributed to delayed initiation of breastfeeding.
Conclusion: Understanding these factors can aid in promoting early breastfeeding initiation and addressing challenges faced by mothers. Improving breastfeeding practices is crucial to reduce neonatal and child mortality, enhance maternal and infant health, and strengthen the mother-infant bond. Health interventions and support programs should target the identified factors to foster optimal breastfeeding practices and improve maternal and neonatal outcomes.
Methods: This hospital-based cross-sectional study was conducted over a period of one year, involving 500 mothers-neonate dyads, admitted in the postnatal ward. Socioeconomic and maternal factors, including maternal stress, were assessed using the Perceived Stress Scale (PSS) and the Edinburgh Postnatal Depression Scale (EPDS) [2]. Early initiation of breastfeeding was defined as breastfeeding starting within one hour of birth.
Results: Majority of mothers (71.8%) were aged 18-25 years and resided in urban areas (66.6%). Most mothers (88.2%) were housewives. Maternal stress assessment revealed that 73% had low stress, and 82.6% did not report any depression. Maternal age, parity, delivery mode, pregnancy complications, and pain interfering with breastfeeding were associated with delayed initiation of breastfeeding. On multivariate analysis, cesarean section (LSCS) and pain (various reasons) were the two main factors which contributed to delayed initiation of breastfeeding.
Conclusion: Understanding these factors can aid in promoting early breastfeeding initiation and addressing challenges faced by mothers. Improving breastfeeding practices is crucial to reduce neonatal and child mortality, enhance maternal and infant health, and strengthen the mother-infant bond. Health interventions and support programs should target the identified factors to foster optimal breastfeeding practices and improve maternal and neonatal outcomes.
Keywords:Breastfeeding; Cross-Sectional Study; Neonatal Mortality; Maternal Stress; Pain
Introduction
Breastfeeding is crucial, offering numerous benefits to both
mothers and infants. It enhances bonding and provides essential
growth factors, immune factors, hormones, and bioactive
components. Mothers benefit from reduced risks of breast cancer,
ovarian cancer, and type 2 diabetes [3]. For infants, breastfeeding
lowers the chances of pneumonia, diarrhea, childhood obesity, atopic
diseases, juvenile diabetes, and sudden infant death syndrome, while
promoting neurodevelopmental growth [4].
Improper breastfeeding practices and pre-lacteal feed contribute
to neonatal mortality, responsible for around 40% of deaths among
children under five [5]. Understanding factors related to early
breastfeeding initiation is vital for promoting optimal breastfeeding.
Several factors influence early breastfeeding, including
socioeconomic factors (area of residence, region, paternal education,
and income) and maternal factors (age at marriage, antenatal care,
birth preferences, physical abuse risk, multiparity, breast issues,
medication, attachment, positioning, and stress) [6].
Early initiation, starting breastfeeding within one hour after
birth, is a critical intervention to prevent neonatal and child deaths,
endorsed by the American Association of Pediatrics (AAP) [7].
Benefits of early initiation are manifold. It increases colostrum
intake, providing infection-fighting antibodies and nutrients.
Skin-to-skin contact regulates neonates’ temperature and triggers
oxytocin release, reducing postpartum complications for mothers.
It strengthens the mother-newborn bond, facilitating successful
exclusive breastfeeding for six months. Moreover, it enhances
maternal immunity, delays subsequent pregnancies, and lowers
insulin needs for diabetic mothers [1-6].
This study aims to analyze various neonatal and maternal
factors that affect breastfeeding initiation. Specifically, maternal
stress, recognized as a significant factor impacting initiation and
continuation of breastfeeding, is objectively assessed using two
scales: the Edinburgh Postnatal Depression Scale and the Perceived
Stress Scale. By investigating these factors, we seek to gain insights
into promoting optimal breastfeeding practices and addressing the
challenges faced by mothers in initiating breastfeeding early.
Materials and methods
Study Design
Hospital-based cross-sectional study
Study Period
One year
Sample Size
The total sample size was calculated using the formula = 4pq/ d2, assuming a prevalence of initiation of breastfeeding to be 50%, a confidence interval of 95%, and an error of 5%. The calculated sample size was N=500.
Hospital-based cross-sectional study
Study Period
One year
Sample Size
The total sample size was calculated using the formula = 4pq/ d2, assuming a prevalence of initiation of breastfeeding to be 50%, a confidence interval of 95%, and an error of 5%. The calculated sample size was N=500.
Consent:
Written and informed consent were obtained from mothers
admitted to the postnatal ward. Information was provided in a
language that the mothers could understand, as the consent form and
patient information sheet were bilingual.Inclusion Criteria
All mothers-infant dyad admitted to the postnatal ward with their babies
Exclusion Criteria
a) Mothers admitted to the obstetric ICU
b) Mothers whose babies were referred to neonatal intensive care. Study tool
Pretested semi-structured proforma.
Methodology
Permission to conduct the study was obtained by institutional ethical
committee. Data collection was done using semi-structured proforma. All interviews were conducted by face-to-face by the investigator who collected data on maternal and neonatal demographic variables and clinical findings of the study participants. It also included information on maternal stress using Perceived stress scale (PSS) and Edinburgh postnatal depression scale.
All mothers-infant dyad admitted to the postnatal ward with their babies
Exclusion Criteria
a) Mothers admitted to the obstetric ICU
b) Mothers whose babies were referred to neonatal intensive care. Study tool
Pretested semi-structured proforma.
Methodology
Permission to conduct the study was obtained by institutional ethical
committee. Data collection was done using semi-structured proforma. All interviews were conducted by face-to-face by the investigator who collected data on maternal and neonatal demographic variables and clinical findings of the study participants. It also included information on maternal stress using Perceived stress scale (PSS) and Edinburgh postnatal depression scale.
Stress scales:
1) Perceived Stress ScaleThe perceived stress scale is most widely used psychological instrument for measuring the perception of stress. It is a self-reported questionnaire that was designed to measure “the degree to which individuals appraise situations in their lives as stressful” 10-item scale (PSS-10) , with 4 positive items and 6 negative items rated on a 5-point Likert scale. Scoring – PSS scores are obtained by reversing responses (e.g., 0 = 4, 1 = 3, 2 = 2, 3 = 1 & 4 = 0) to the four positively stated items (items 4, 5, 7, & 8) and then summing across all scale items. Stress level are classified as to the points on likert scale as- Low stress (0-13), Moderate stress (14-26) and High perceived stress (27- 40)
2) Edinburgh Postnatal Depression Scale:
The Edinburgh Postnatal Depression Scale (EPDS) is one of the
most widely used screening instruments for assessing symptoms of
perinatal depression and anxiety. This is a 10-item scale with each
item scored from 0 to 3. Maximum score: 30 Possible Depression: 10
or greater Always look at item 10 (suicidal thoughts). The mother
was screened for possible PPD using the 10-item well-validated
Edinburgh PPD Scale (EPDS) in hindi language(2) with responses varying from 0 to 3 for each item. The cutoff point to screen the PPD is decided as score more than 10.5 based on a study done by Desai et al. to validate the EPDS in Gujarat language with a specificity of 98% and sensitivity 100% It assesses emotional experiences over the past seven days using ten Likert-scale items. Scoring is as: Depression not likely (<8), Depression possible (9-11), Fairly high possibility of depression (12-13) and Probable depression (14 and higher)
Ethical Clearance:
The study was initiated after obtaining permission from the
institutional ethical committee (letter number: 478/MC/IEC/2020).Statistical analysis:
The collected data were transformed into variables, coded and
entered in Microsoft Excel. Data were analyzed and statistically
evaluated using SPSS-PC-25 version. Quantitative data was expressed
in mean ± standard deviation and depends on normality distribution
difference between two comparable groups were tested by student’s
t-test (unpaired) or Mann Whitney ‘U’ test. Qualitative data were
expressed in percentage and statistical differences between the
proportions were tested by chi square test or Fisher’s exact test. All
the factors which were found to be significant in univariate analysis
were included in the multiple logistic regression model and adjusted
odds ratio along with 95% CI was calculated for delayed initiation of
breastfeeding.Results
Maternal and neonatal parameters:
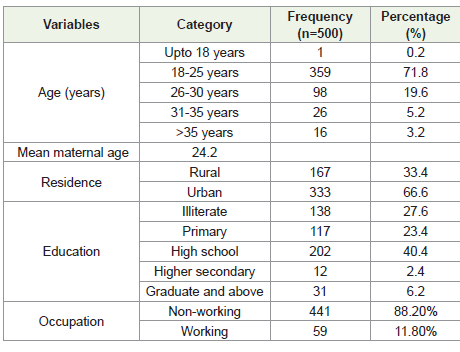
[Table 1] represents sociodemographic profile of mothers of
neonates admitted in postnatal ward. Out of 500 mothers, 71.8%
mothers belonged to age range of 18 to 25 years. In the study,
maximum mothers were resident of urban area (66.6%) and majority
of them (40.4%) were educated up to high school. In our study
88.2% of mothers were housewives and 11.8% females were working
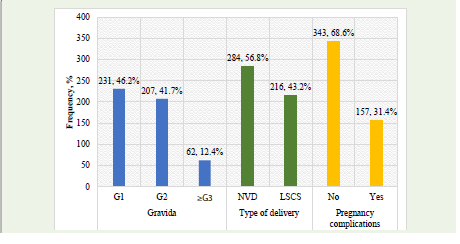
mothers. Obstetric profile of mothers has been displayed in Figure
1. Majority of mothers were primigravida (46.2%). Mode of delivery
was vaginal and LSCS in 56.8% and 43.2% cases respectively. The
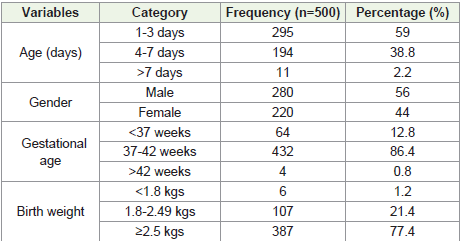
study revealed 68.6% of mothers had pregnancy complications.Neonatal demographic parameters have been displayed in
table 2.59% of neonates aged between less than 24-72 hours. Male
predominance was observed which accounted to 56% and majority
of neonates were full term i.e 432 (86.4%) Birthweight of 77.4% of
neonates was more than 2.5 kg whereas 21.4% neonates had birth
weight ranged between 1.8 to 2.49 kgs.
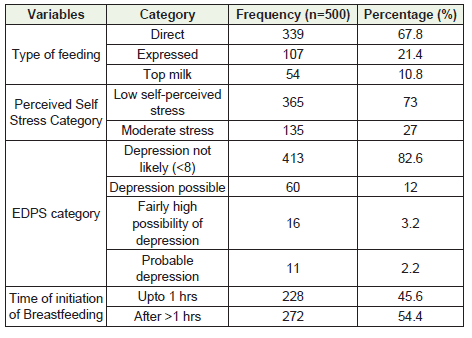
73% of mothers had low self-perceived stress. When considering EPDS score, out of 500 mothers 82.6% did not report any depression while 12% mothers had possible depression. Early initiation of breastfeeding was observed in 45.6% of mothers.
73% of mothers had low self-perceived stress. When considering EPDS score, out of 500 mothers 82.6% did not report any depression while 12% mothers had possible depression. Early initiation of breastfeeding was observed in 45.6% of mothers.
Univariate analysis:
[Table 4] presents the relationship between various parameters
and the initiation of breastfeeding. In terms of neonatal parameters,
46.1% of male neonates and 45% of female neonates had early
initiation of breastfeeding. Additionally, 44.2% of low birth weight
(LBW) neonates and 44.9% of preterm neonates had early initiation
of breastfeeding. However, difference in none of these neonatal
parameters showed a statistically significant association with the
initiation of breastfeeding.Regarding maternal factors, 39.5% of mothers residing in
rural areas-initiated breastfeeding within one hour, while 48.6%
of mothers living in urban areas did the same. This difference was
also not found to be statistically significant (p>0.05). Among literate
mothers, 50.7% initiated breastfeeding within one hour, whereas
43.6% of illiterate mothers did the same, and this difference was not
statistically significant (p>0.05). Furthermore, 46.7% of non-working
mothers had early initiation of breastfeeding, whereas only 36.7% of
working mothers-initiated breastfeeding within one hour. Again, this
difference was not statistically significant.
The mean maternal age for early initiation of breastfeeding
was 23.48±4.11, while for delayed initiation, it was 24.80±4.80.
This difference of maternal age and initiation time was found to be
statistically significant (p<0.01).
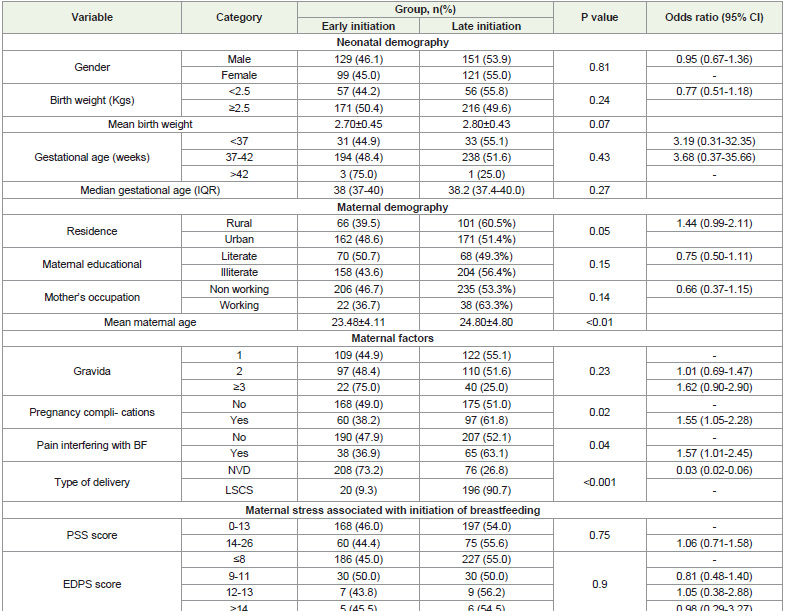
The preceding data examines maternal factors linked to the
initiation of breastfeeding. Among primiparous women, delayed
initiation was observed in 55.1%, while among multiparous women,
the rate was 25% (p>0.05). In women with pregnancy complications,
63.1% experienced delayed initiation, whereas in women without
pregnancy complications, the rate was 52.1%. This association was
found to be statistically significant with a p-value of 0.02, suggesting
that pregnancy complications may impact breastfeeding initiation.
Furthermore, for women experiencing pain, initiation was
delayed in 63.1% of neonates. This association was also found to be
statistically significant, with a p-value of 0.04, suggesting that pain
during breastfeeding influences the timing of initiation. Moreover,
among women with vaginal delivery, 26.8% experienced delayed
initiation, while a significantly higher proportion of 90.7% of women
who underwent LSCS experienced delayed initiation. This difference
was found to be statistically significant (p<0.001).
In regard with association of maternal stress. Among mothers
with low perceived stress, delayed initiation was observed in 54% of
cases, while among mothers with moderate stress, the rate was 55.6%
(p>0.05). Additionally, mothers without depression had a delayed
initiation rate of 54%, whereas mothers with probable depression had
a slightly higher rate of 54.5%.
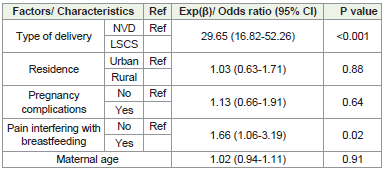
Multivariate logistic regression analysis:
[Table 5] presents Multivariate logistic regression analysis of
independent factors for delayed initiation of breastfeeding. All the
factors which were found to be significant in univariate analysis were
included in the multiple logistic regression model. After adjusting
for other factors, the independent predictors for delayed initiation
of breastfeeding were LSCS delivery [AOR = 29.65 (95% CI: 16.82,
52.26)], and pain interfering with breastfeeding [AOR = 1.66 (95%
CI: 1.06, 3.19)].Discussion
Breastfeeding after one hour of birth increases the risk of
infant mortality, according to a systematic review[8]. Many
factors, including mode of delivery, mother’s parity, maternal
stress, insufficient milk supply, and maternal illness, are negatively
associated with successful breastfeeding, resulting in delays in early
breastfeeding initiation (within the first hour of birth) and reduced
duration of exclusive breastfeeding for infants. Breastfeeding should
be started as soon as possible, preferably within one hour, according
to WHO recommendations.[9]
Analysis of a large cohort of almost 100,000 newborns from three
large trials conducted in India, Ghana and Tanzania had shown that
in comparison to infants who started breastfeeding during the first
hour of life, the risk of neonatal death was 41 percent and 79 percent
greater in infants who started breastfeeding between 2-23 hours and
24-96 hours after delivery, respectively. [8].
In our study the early initiation of breastfeeding was practiced
in 45.6% of newborns. Gupta et al.and Sharma et al [10,11] reported
breast feeding within one hour in 40%, and 38.6% of newborns
respectively. This rate is less than 50% and it clearly indicates that
majority of newborns are not fed timely even after the institutional
deliveries in India are almost 95% [5]
Neonatal factors affecting initiation of breastfeeding:
In present study the. mean gestational age of neonates was (38.2
+1.780) weeks. 44.9% of preterm infants were breastfed within one
hour of birth, whereas breastfeeding was started early in 48.4% and
75% of full-term and post-term newborns, respectively. The findings
were contrary with observations of Ayton et al and Meckonen et
al who concluded that late preterm and term neonates had lower
rates of early initiation of breastfeeding [12,13]. In our study, 46.1%
of mothers with male newborns-initiated breast feeding within
one hour, which was comparable to other studies [14]. Though the
differences in initiation of breast feeding as per gestational age and
gender are not statistically significant.In our study, 44.2% of low-birth-weight neonates were breastfed early. These findings were similar to other studies where no association between birthweight and initiation of breastfeeding was established.
Maternal factors affecting initiation of breastfeeding:
The study showed 50.7% of literate mothers and 43.6% of illiterate
mothers started breastfeeding within an hour. The association
between maternal literacy and breastfeeding initiation was not
statistically significant. This observation is significant as rural women
are usually illiterate but they can be motivated to breast feed early
by observing peers in institutional deliveries, thus this could be one
more benefit of institutional deliveries.39.5% of mothers residing
in rural areas whereas 48.6% of those from urban areas-initiated
breastfeeding within one hour. This observation is similar with the
study conducted by Khanal et al. and may reflect better exposure to
appropriate breastfeeding practices among urban mothers [15].In current study, mothers with complications during pregnancy
had a lower rate of early breastfeeding initiation (38.4%). Antepartum
hemorrhage, postpartum hemorrhage, and eclampsia were among
the illnesses that required intensive care treatment, leading to delayed
initiation of breastfeeding. Complications during pregnancy were
significantly associated with late initiation of breastfeeding. Working
mothers (36.7%) in our study had a slightly lower rate of early
breastfeeding initiation compared to non-working women (46.7%),
as observed in other studies as well [16,17]. In our study mothers
who experienced pain interfering with breastfeeding (36.9%) also
had delayed initiation, with mastitis, breast engorgement, and pain
due to LSCS being the main contributing factors. This vicious cycle
of pain leading to delayed initiation was found to be significant. As
per our findings, delivery by cesarean section (LSCS) was associated
with delayed initiation of breastfeeding. Various meta-analysis has
also concluded that LSCS deliveries are linked to lower odds of timely
breastfeeding initiation compared to vaginal birth [18,19,20].
Breastfeeding provides potential protection against postpartum
depression. However, early cessation of breastfeeding and severe
breastfeeding discomfort or pain are associated with postpartum
depression. Breastfeeding may have an antidepressant effect and
contribute to a better regulation of diurnal basal cortisol secretion
[21]. In our study, maternal stress was measured using the Perceived
Stress Scale, with 73% of mothers experiencing low stress and 27%
experiencing moderate stress. While all mothers experienced some
level of stress during delivery, the relationship between maternal
stress and initiation of breastfeeding was not found to be statistically
significant. The initiation of breastfeeding showed no relation with
depression as only 2.2% of mothers were probably depressed as per
scoring in the study. This result was consistent with the study of
Amipara et al and other similar studies [22,23]. The relation between
stress and delayed initiation of breastfeeding is not well established
though early initiation of breast feeding can decrease stress in
lactating mothers at the same time the constant worry that baby is
not getting enough milk can be a reason of stress [24].
Conclusion
Our study revealed significant association between the mode of
delivery and pain experienced during delivery with delayed initiation
of breastfeeding. However, maternal stress was not significantly
associated with delayed initiation of breastfeeding. Based on these
results, we strongly recommend that all mothers are counselled about
the importance of early breastfeeding initiation during their antenatal
car visits. Additionally, it is crucial to identify women who may be at
a higher risk of not starting breastfeeding on time and provide them
with additional lactation support
To promote early breastfeeding initiation, a best practice is
to have all newborns placed on their mother’s breast shortly after
delivery in the labor room, (skin to skin contact) with assistance
from healthcare professionals. This approach will help initiate
breastfeeding as promptly as possible, enhancing the likelihood of
successful breastfeeding and its associated health benefits for both
mother and baby.
The conclusions drawn from this study are subject to certain
limitations that need to be considered. Firstly, the findings may not
be applicable to the general population as the study was conducted
in a hospital setting, which may not fully represent the broader
demographic diversity. Secondly, since this study was designed as a
one-time observational study, we did not assess the impact of early
initiation on total duration of breastfeeding.
Ethical clearance:
The approval was obtained from the Institutional Ethical
Committee of the Gandhi Medical College, Bhopal (letter number:
478/MC/IEC/2020).References
Citation
Gohiya P, Sonkar R. Determinants of Initiation of Breastfeeding: A Cross-Sectional Study. Indian J Nutri. 2025;12(2): 322.