Research Article
High Fat, High Sugar and High Salt Food Consumption among Adolescent Girls Residing in Mumbai City
Mishra Sonu1*, Subhadra M2 and Neha S3,4
1Department of Foods, Nutrition and Dietetics, College of Home Science, Nirmala Niketan, Affiliated to University of Mumbai, Maharashtra, India.
2Department of Foods, Nutrition and Dietetics,College of Home Science, Nirmala Niketan, Affiliated to University of Mumbai, Maharashtra, India.
3Department of Foods, Nutrition and Dietetics, Hirabai Cowasji Jehangir Medical Research Institute, Pune, Maharashtra, India.
4Department of Foods, Nutrition and Dietetics, School of Health Sciences, Savitribai Phule Pune University, Pune, Maharashtra, India.
2Department of Foods, Nutrition and Dietetics,College of Home Science, Nirmala Niketan, Affiliated to University of Mumbai, Maharashtra, India.
3Department of Foods, Nutrition and Dietetics, Hirabai Cowasji Jehangir Medical Research Institute, Pune, Maharashtra, India.
4Department of Foods, Nutrition and Dietetics, School of Health Sciences, Savitribai Phule Pune University, Pune, Maharashtra, India.
*Corresponding author:Mishra Sonu, Department of Foods, Nutrition and Dietetics, College of Home Science, Nirmala Niketan, Affiliated to University of Mumbai, Maharashtra, India. E-mail Id: sonu01m@gmail.com
Article Information: Submission: 24/07/2025; Accepted: 12/08/2025; Published: 15/08/2025
Copyright: ©2025 Sonu M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: The frequent consumption of high-fat, salt, and sugar (HFSS) foods among youngsters leads to a higher risk of overweight, obesity, and nutrient deficiencies, thereby raising concerns about the future risk of noncommunicable diseases (NCDs). The study aimed to assess the consumption pattern of HFSS food intake among adolescent girls in Mumbai and examine the influence of socioeconomic status on these habits.
Methods: A cross-sectional study was conducted among 1,035 adolescent girls aged 13–18 years who were selected through random and purposive sampling from four zones of Mumbai (North, South, East, and West). Participants were categorized as per their socioeconomic status (as per the Kuppuswamy scale). Data on HFSS food consumption were collected using a structured food frequency questionnaire and analysed using SPSS version 25.0.
Results: The findings revealed a high prevalence of HFSS food consumption among adolescent girls. Daily intake was most common for sugar as an ingredient in various recipes (55.8%), tea with sugar (48.1%), cream biscuits (39.2%), sweet biscuits (32.3%), and chocolates (31.8%). Weekly consumption was notable for chaat (47.4%), instant noodles (43.5%), vada pav/samosa (42.8%), and sugary beverages. Bakery items and processed foods like wafers and cheese were consumed predominantly on a weekly or monthly basis. Socioeconomic status significantly influenced HFSS food intake, with higher consumption observed among girls from higher socioeconomic backgrounds (p<0.05)
Conclusion: This study highlights socioeconomic disparities in the widespread and frequent intake of HFSS foods among adolescent girls in Mumbai, underscoring an urgent need for targeted nutrition education and intervention programs to foster healthier eating behaviours and reduce the immediate as well as future risk of NCDs in this vulnerable population.
Methods: A cross-sectional study was conducted among 1,035 adolescent girls aged 13–18 years who were selected through random and purposive sampling from four zones of Mumbai (North, South, East, and West). Participants were categorized as per their socioeconomic status (as per the Kuppuswamy scale). Data on HFSS food consumption were collected using a structured food frequency questionnaire and analysed using SPSS version 25.0.
Results: The findings revealed a high prevalence of HFSS food consumption among adolescent girls. Daily intake was most common for sugar as an ingredient in various recipes (55.8%), tea with sugar (48.1%), cream biscuits (39.2%), sweet biscuits (32.3%), and chocolates (31.8%). Weekly consumption was notable for chaat (47.4%), instant noodles (43.5%), vada pav/samosa (42.8%), and sugary beverages. Bakery items and processed foods like wafers and cheese were consumed predominantly on a weekly or monthly basis. Socioeconomic status significantly influenced HFSS food intake, with higher consumption observed among girls from higher socioeconomic backgrounds (p<0.05)
Conclusion: This study highlights socioeconomic disparities in the widespread and frequent intake of HFSS foods among adolescent girls in Mumbai, underscoring an urgent need for targeted nutrition education and intervention programs to foster healthier eating behaviours and reduce the immediate as well as future risk of NCDs in this vulnerable population.
Keywords:Adolescents; HFSS (High Fat, Salt, And Sugar); Socioeconomic Status
Introduction
The World Health Organization (WHO) defines adolescence as
the period from 10-19 years. This period is recognized as a crucial
transitional phase of growth and development from childhood to
adulthood, which requires good nutrition and a healthy lifestyle [1].
Adopting healthy eating patterns, that is, regular consumption of a
variety of whole grains and nutrient-rich cereals (pearl millet, finger
millet, etc.), legumes, seasonal fruits and vegetables, meat, milk, and
eggs, is essential to support the final growth spurt during adolescence
[2].
Medina et al. (2020) defined eating habits as “conscious, collective
and repetitive behaviors which lead people to select, consume, and use
certain foods or diets, in response to social and cultural influences”
[3]. The consumption of poor-quality diets is one of the biggest
contributors to the global burden of non-communicable diseases
(NCDs). Amongst all age groups, the age group of adolescents has
been consistently identified as a model displaying the consumption
of a poor-quality diet, characterised by the low consumption of fruits
and vegetables, whole grains, lean meat, and low-fat dairy, and the
high intake of confectionery, high-sugar beverages, processed meats,
refined grains, and ready-to-eat meals [4].
High-fat, salt, and sugar (HFSS) foods are those prepared with
excessive amounts of cooking oil/fats, sugar, or salt. The Food Safety
and Standards Authority of India (FSSAI) defines HFSS foods as
processed food products that contain high levels of saturated fat,
total sugar, or sodium. The declared nutritional values of these
ingredients exceed the recommended limits of energy (kcal) from
total sugar (<10% of total energy), energy from saturated fat (<10%
of total energy), and sodium (<1 mg/1 kcal).The daily consumption
of >15% of energy from visible ghee/oil/butter, salt intake of >5g/
day, and >25g/day of sugar (for 2000 kcal/day) is considered high.
High-fat foods include all deep-fried foods and foods prepared with
high quantities of oil/fat, such as French fries, samosa, kachoris, puris,
desserts, biscuits, cookies, cakes, and parathas. Processed foods/prepackaged
foods like chips, biscuits, namkeen, papad, and pickles are
examples of high-salt foods. Commercially prepared jams, sauces, icecreams,
etc. can be considered examples of high-sugar foods. HFSS
foods are considered unhealthy as they lack essential amino acids,
fatty acids, and micronutrients and their excessive consumption
increases the risk of noncommunicable diseases [5].
One of the main concerns regarding the consumption of
HFSS foods during early life is the increasing prevalence of
childhood overweight and obesity, which can lead to a range of
health complications later in adulthood. However, due to the ease
of availability, variety, appealing taste, attractive and persistent
advertisements, and peer pressure, the intake of these foods continues
to rise, particularly among children and adolescents. Additionally, the
lack of awareness about the health risks associated with HFSS foods,
combined with strong taste preferences and social influences, further
contributes to unhealthy eating patterns [6,7].
Thus, the aim of the present study was to study the HFSS food
consumption patterns among adolescent girls residing in Mumbai
city.
Materials and methods
Study Population:
The present study was conducted on adolescent girls (aged 13–
18 years) residing in Mumbai City belonging to low (LSES), middle
(MSES), and high (HSES) socioeconomic statuses.Sample size and sampling technique:
The study population (N=1035) was primarily selected using
random sampling followed by purposive sampling. One ward from
each of the four zones of Mumbai City (North, South, West and East)
was selected randomly. From each ward, adolescent girls aged 13–18
years belonging to three different socio-economic strata (low, middle,
and high-income groups as per Kuppuswamy scale, 2019) were
included in the study.Ethics approval:
The research proposal was approved by the Institutional Ethical
Committee (IEC) of Dr. BMN College of Home Science. The
proposal has been registered with the Clinical Trials Registry - India
CTRI/2021/07/034563. After obtaining assent from the participants,
a duly signed informed consent was obtained from the parents of
participants as the participants were minors.Data Collection:
Data on HFSS food consumption were collected using a food
frequency questionnaire (FFQ). The questionnaire had two parts.
Part A included questions on demographic details of the participants
(gender, age, family type, monthly income, education, and occupation
of parents). The modified Kuppuswamy Scale was used to determine
the socio-economic status of study participants. Part B included
questions on the frequency and quantity of HFSS foods consumed
by the participants. A list of 25 food items classified into high-fat,
high-salt and high-sugar foods was included in the FFQ. The FFQ
was explained to the participants, and they were asked to select one
frequency for the consumption of each food. The frequency of HFSS
foods intake in this study is categorized as follows: less than 25%
(low), 25–50% (moderately high), and more than 50% (high).Data Analysis:
Data collected were statistically analysed using SPSS software for
Windows (version 25, 2017, IBM Corporation, Armonk, New York,
United State). The frequencies of intake of food items are presented
as percentages. The frequency of consumption of food was coded as:
Never = 1, Monthly = 2, Weekly = 3 and Daily = 4. The frequency
intake between the three SES were compared using the Kruskal–Wallis
H test with Bonferroni correction to adjust for multiple comparisons.
The data for frequency consumption for the three groups is presented
as Mean± SD, with a higher mean indicating more frequent intake. A
p-value <0.05 after Bonferroni correction was considered statistically
significant.Results
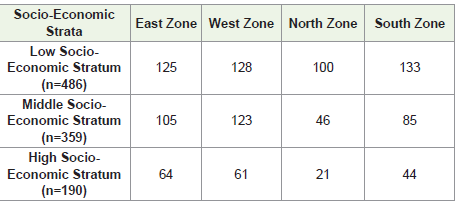
The study was conducted among 1,035 adolescent girls aged 13–18
years residing in Mumbai city. The sample comprised 486 girls from
LSES, 359 from MSES, and 190 from HSES backgrounds, ensuring
representation across all geographic, age, and socioeconomic groups
[Table 1].
Daily consumption of HFSS foods:
The foods for which the frequency of daily intake was assessed
among adolescent girls were categorized as high-sugar foods, highfat-
high-salt foods, and high-fat–high-sugar foods. The highest daily
consumption was observed for items in the high-sugar foods category,
with 55.8% reporting daily use of sugar (as an ingredient in various
recipes), followed by 48.1% consuming tea typically sweetened with
sugar. In the high-fat-high-salt category, toasts/bread/pav (25.4%)
and savoury biscuits (24.4%) were most commonly consumed on a
daily basis. Among high-fat-high-sugar foods, cream biscuits (39.2%),
sweet biscuits (32.3%), and chocolate (31.8%) showed moderately
high intake. [Table 2]Weekly consumption of HFSS foods:
The patterns observed highlighted the popularity of savory and
snack foods rich in fats and salt. Chaat (47.4%), instant noodles
(43.5%), and vadapav/samosa (42.8%) were frequently consumed on
a weekly basis. In addition, a moderately high weekly intake was also
observed for chocolate (40.4%) and cream biscuits (39.2%) followed
by sugary beverages like non-aerated beverages (35.6%), aerated soft
drinks (32%), coffee/cold coffee (30.2%), fruit juices/sweetened lime
juice (29.6%), and fruit milkshakes/smoothies/falooda (28.6%) [Table 2]Monthly consumption of HFSS foods:
The consumption of packaged processed foods such as wafers/
French fries (46.6%), fruit milkshakes/smoothies (40.1%), and chaat
(39.3%) were the highest. Several high-fat-high-salt foods, including
cheese (36.1%), khari (26.8%), and farsan (27.4%), as well as high sugar
beverages like fruit juices (31.4%) and aerated soft drinks
(31.3%), also showed high monthly intakes [Table 2].To summarise, high-sugar foods including the added sugar
recipes and tea, health drinks, and coffee/cold coffee were integrated
into the daily routines of adolescent girls, whereas high-fat-highsugar
foods (cream biscuits, sweet biscuits, chocolate) are also
consumed frequently. Some of the high-fat-high-salt foods such as
toasts/bread/pav and savoury biscuits are commonly eaten daily, but
some other foods in the same category i.e. vadapav/samosa, instant
noodles, chaat were typically consumed weekly or monthly.

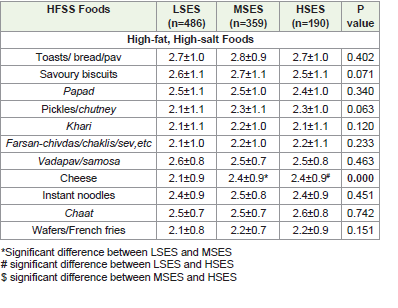
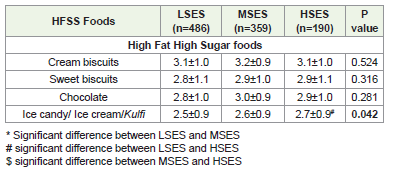
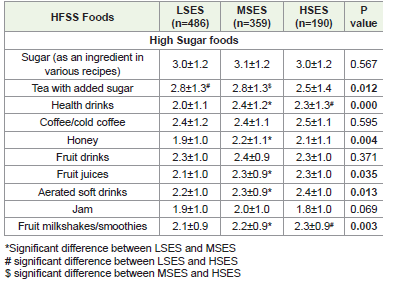
Consumption patterns of HFSS foods as per the Socioeconomic Status:
[Table 3-5] Pesent the socioeconomic disparities in the mean
frequency of intake of HFSS foods. A significant difference was found
in the intake of cheese (high-fat-high-salt food), ice cream (highfat-
high-sugar foods), honey, health drinks, tea, fruit juices, fruit
milkshakes, aerated soft drinks, and fruit drinks (high sugar foods)
across SES groups (p<0.05).The frequency of cheese consumption was higher in adolescents
in both MSES and HSES groups compared to that in the LSES group
(p<0.05), with a similar trend observed for health drinks and fruit
milkshakes. In contrast, tea consumption was higher among the
LSES and MSES groups than that in the HSES group (p<0.05). Fruit
juices and aerated soft drinks were more frequently consumed by
adolescents in the MSES group compared to those in the LSES group
(p<0.05).
Discussion
The present study provides a comprehensive assessment of HFSS
food consumption patterns among 1,035 adolescent girls in Mumbai,
highlighting the frequency and types of HFSS foods consumed, as
well as the influence of socioeconomic status (SES) on these dietary
habits.
Daily Consumption Patterns:
The high daily sugar and sweet product consumption is
particularly concerning, as the excessive intake of added sugars is
a well-established risk factor for obesity and NCDs. Our findings
are consistent with those of a study conducted in Mumbai in 2022,
which also reported sugar as the most frequently consumed HFSS
item among adolescents daily, with early adolescents consuming
sugar more often than late adolescents [8]. These findings are also
consistent with those of Wadakappanavar et al. (2019), who also
reported notably high snack consumption rates among both urban
(85%) and rural (90%) children. Their study also highlighted that
benne biscuits-made primarily from maida, ghee, and sugar—were
the most frequently consumed snack, with a daily intake observed
in 80.71% of children [9]. Similarly, Poornima B et al, (2024) studied
frequency of HFSS food consumption among girls aged 11-16 years
(n=129) and reported that 20% of the girls consumed fried and salty
foods such as chips on a daily basis, 70% of the girls were consuming
biscuits, cookies and chocolates daily. It was concluded that there was
a significantly (p<0.05) higher consumption of bakery products, ice
cream, packaged fruit juices and chips among all girls [10]Weekly and Monthly Consumption Patterns:
Approximately 30% of the participants preferred to consume
high-salt and fat-rich savoury snacks such as chaat, instant noodles,
and vada pav/samosa, as well as high- sugar and fat-rich foods,
including ice cream and chocolates, every week. Sugary beverages,
including fruit drinks and aerated soft drinks, also showed a
moderately high weekly consumption. High-fat foods like wafers/
French fries and cheese were consumed predominantly on a monthly
basis. These patterns showed similar findings from other Indian cities,
such as Guwahati and Jaipur, where frequent fast food and snack
consumption among adolescents was attributed to convenience,
taste preferences, and lifestyle factors [11,12]. Some other factors
responsible for adopting HFSS food among adolescent identified by
Maitri P (2021) were nuclear family, skipping breakfast, time, taste
and attractiveness of these foods, emotional eating, lack of nutritional
knowledge, and role of advertising [13].Socioeconomic Differences:
A significant finding of this study is the influence of SES on HFSS
food consumption. Girls from higher SES backgrounds reported
greater intakes of cheese, flavoured milk, fruit milkshakes, and soft
drinks (p<0.05), whereas tea consumption was higher among those
from LSES and MSES groups (p<0.05). These results align with
the findings of Gupta et al. (2018) in rural Himachal Pradesh, who
reported the highest junk food consumption among children from
high SES, which could be attributed to increased affordability and
access [14].The contribution of ultra processed foods to the total macronutrient
intake of adolescents from two different socioeconomic status (SES)
groups—middle-income and low-income families—in Delhi showed
that adolescents in the middle-income group derive a significantly
greater proportion—and greater absolute amounts—of their daily
energy, carbohydrates, fat, and protein from ultra-processed foods
when compared to those from the low-income group [15].
The widespread consumption of HFSS foods can be attributed to
several factors, including easy availability, aggressive marketing, peer
influence, and changing family dynamics. Arya and Dubey (2023)
highlighted the role of food delivery apps, small family sizes, and the
prevalence of working mothers in promoting fast food intake among
Indian adolescents [16].
In a study by Tawheed A et al. (2017) involving 51 respondents,
31.9% were aware of the high sugar content in fast foods, 68.8%
recognized the high salt content, 74% knew about the high saturated
fat content, and 51.5% were aware of their high cholesterol
levels stressing on the fact, that in spite of having awareness, the
consumption of these foods are still high in adolescents [17]
Shete and Wagh (2018) reported a positive association between
junk food intake and higher body mass index among adolescents,
indicating that poor dietary habits during adolescence are linked to
higher risks of overweight, obesity, and nutrient deficiencies, which
can persist into adulthood and elevate the risk of NCDs [18].
Conclusion
This study demonstrates a concerning widespread and frequent
intake of high-fat, high-sugar, and high-salt foods by more than 30%
of the adolescent girls residing in Mumbai. Socioeconomic status
significantly influenced these dietary habits, with a higher percentage
of participants from HSES groups showing greater consumptions of
certain HFSS foods. These findings underscore an urgent need for
targeted nutrition education and intervention programs to promote
healthier eating behaviors among adolescent girls.
Acknowledgment
Authors would like to thank all the participants of the study for
their cooperation, and contribution of valuable data for the research
project.
References
Citation
Sonu M, Subhadra M, Neha S. High Fat, High Sugar and High Salt Food Consumption among Adolescent Girls Residing in Mumbai City. Indian J Nutri. 2025;12(2): 321.