Research Article
Nutritional Status and Health Outcomes Among Traffic Police in Belagavi, India: A Cross-Sectional Study
Pirjade S1 and Kour H2*
1Department of Nutrition and Dietetics, J.N Medical College, Belagavi, Karnataka, India.
2Department of Physiology, J.N Medical College Belagavi, Karnataka, India.
2Department of Physiology, J.N Medical College Belagavi, Karnataka, India.
*Corresponding author:Dr. Harpreet Kour, Department of Physiology, J.N Medical College Belagavi, KLE Academy of Higher Education and Research, Belagavi, Karnataka, India E-mail id: harpreetkour.kour@gmail.com
Article Information:Submission: 23/06/2025; Accepted: 02/08/2025; Published: 06/08/2025
Copyright: © 2025 Pirjade S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Traffic police personnel are subjected to multiple occupational stressors including prolonged standing, air pollution, and irregular schedules, which may predispose them to poor nutritional and health outcomes.
Methods: A cross-sectional study was conducted among 70 traffic police personnel aged 40 to 60 years in Belagavi, Karnataka. Data on nutritional status were obtained through anthropometric assessments, three-day 24-hour dietary recall, and a food frequency questionnaire (FFQ). Health outcomes were assessed using the Work Ability Index (WAI), International Physical Activity Questionnaire (IPAQ), Perceived Stress Scale (PSS), and Pittsburgh Sleep Quality Index (PSQI). Descriptive statistics, Pearson correlation, and Chi-square tests were employed for analysis. P value less than 0.05 was considered as significant.
Results: The mean age of participants was 47.57 ± 6.12 years. The mean BMI was 26.25 ± 3.31 kg/m², with 62.8% of participants classified as overweight or obese. Dietary intake exceeded recommended daily allowances for energy and macronutrients, while only 8.6% had good dietary diversity. Low physical activity was reported by 80% of participants, 67.1% experienced moderate stress, and 41.4% had poor sleep quality. Work ability scores were poor in 91.4% of cases. Significant associations were found between BMI and both work ability (p = 0.04) and sleep quality (p = 0.02).
Conclusion: Traffic police personnel in Belagavi exhibit a high burden of modifiable health risks related to nutrition, physical inactivity, and occupational strain. Multi-component health interventions targeting diet, physical activity, and recovery behaviors are urgently needed to improve health outcomes and occupational sustainability in this workforce.
Methods: A cross-sectional study was conducted among 70 traffic police personnel aged 40 to 60 years in Belagavi, Karnataka. Data on nutritional status were obtained through anthropometric assessments, three-day 24-hour dietary recall, and a food frequency questionnaire (FFQ). Health outcomes were assessed using the Work Ability Index (WAI), International Physical Activity Questionnaire (IPAQ), Perceived Stress Scale (PSS), and Pittsburgh Sleep Quality Index (PSQI). Descriptive statistics, Pearson correlation, and Chi-square tests were employed for analysis. P value less than 0.05 was considered as significant.
Results: The mean age of participants was 47.57 ± 6.12 years. The mean BMI was 26.25 ± 3.31 kg/m², with 62.8% of participants classified as overweight or obese. Dietary intake exceeded recommended daily allowances for energy and macronutrients, while only 8.6% had good dietary diversity. Low physical activity was reported by 80% of participants, 67.1% experienced moderate stress, and 41.4% had poor sleep quality. Work ability scores were poor in 91.4% of cases. Significant associations were found between BMI and both work ability (p = 0.04) and sleep quality (p = 0.02).
Conclusion: Traffic police personnel in Belagavi exhibit a high burden of modifiable health risks related to nutrition, physical inactivity, and occupational strain. Multi-component health interventions targeting diet, physical activity, and recovery behaviors are urgently needed to improve health outcomes and occupational sustainability in this workforce.
Keywords:Nutritional Status; Occupational Health; Traffic Police; Body Mass Index (BMI); Physical Activity; Sleep Quality; Work Ability Index; Perceived Stress; Dietary Diversity; India
Introduction
Occupational health is a critical dimension of workforce
sustainability, particularly in high stress, high-exposure professions
such as traffic policing. Traffic police personnel, while integral to
urban traffic regulation and public safety, operate under strenuous
conditions marked by prolonged standing hours, irregular shifts, and
chronic exposure to air pollution, thermal extremes, vehicular noise,
and ultraviolet radiation [1]. These environmental and occupational
hazards are compounded by physical fatigue and psychological stress,
creating a unique risk profile that distinguishes traffic police from
other public sector workers.
The physiological burden imposed by this work environment is
reflected in growing evidence of elevated rates of non-communicable
diseases (NCDs), including obesity, hypertension, type 2 diabetes
mellitus, and musculoskeletal disorders, among law enforcement
personnel globally [2]. Despite the physically mobile nature of their
duties, traffic police often exhibit sedentary behaviour patterns outside
working hours and face challenges in maintaining healthy dietary and
lifestyle practices. Irregular meal timing, limited dietary diversity,
and excessive caloric intake often a consequence of occupational time
constraints and poor nutritional awareness are well-documented
contributors to metabolic dysregulation in shift-based occupations
[3].
Furthermore, stress-related disorders and impaired sleep quality
are increasingly recognized as prevalent among police forces, with
empirical data linking chronic stress exposure to reduced work
performance, increased absenteeism, and accelerated biological aging
[4,5]. These concerns are magnified in developing countries, where
occupational health surveillance systems are limited and preventive
interventions for high-risk occupational groups remain inadequately
implemented.
Despite these risks, there is a paucity of comprehensive data
on the nutritional status and health outcomes of traffic police in
India. Most existing studies either generalize findings from broader
law enforcement populations or focus narrowly on select health
parameters without integrating dietary and lifestyle assessments.
This gap is particularly pronounced in tier-2 cities such as Belagavi,
Karnataka, where urbanization and vehicular density continue to
increase, intensifying occupational exposures for traffic personnel
In this context, the present study was designed to evaluate the
nutritional status and health outcomes of traffic police personnel aged
40 to 60 years in Belagavi city. Using a combination of anthropometric
assessments, dietary intake evaluation, and standardized tools for
measuring physical activity, sleep quality, stress levels, and work
ability, this study aims to generate evidence to inform occupational
health interventions tailored to this vulnerable population.
Methodology
This was a community-based, cross-sectional study conducted
among traffic police personnel in Belagavi City, Karnataka, India,
between October 2024 and March 2025. The objective was to assess
the nutritional status and health outcomes including work ability,
stress, sleep quality, and physical activity among traffic police officers
aged 40–60 years.
The target population included uniformed traffic police officers
employed by the Belagavi Police Department. Participants were
eligible if they (i) were aged 40 to 60 years, (ii) were actively engaged
in traffic control duties for a minimum of one year, and (iii) provided
informed written consent. Individuals were excluded if they had been
recently transferred out of traffic duty, were on extended leave during
the study period, or declined participation.
A total of 70 traffic police personnel aged 40 to 60 years were
recruited using convenience sampling and list of traffic police
personnel obtained from the Belagavi Police Department. The
sample size was estimated based on anticipated prevalence from
prior studies, with a 95% confidence level and acceptable margin
of error [6]. A non-probability convenience sampling method was
used. Participants were recruited from multiple traffic junctions and
police stations to ensure diversity in location and work exposure.
Data collection was performed during daytime hours at or near the
workplace to minimize disruption to duty.
Ethical approval was obtained from the Institutional Ethics Committee of Jawaharlal Nehru Medical College, Belagavi (Ref. No. MDC/JNMC/IEC/441, dated 24/08/2024). Written informed consent was obtained from all participants prior to data collection. Administrative permission was also secured from the office of the Deputy Commissioner of Police, Belagavi.
All participants underwent a standardized interview, anthropometric assessment, and questionnaire-based evaluation. Trained investigators conducted face-to-face interviews in Kannada or English, as per participant
Ethical approval was obtained from the Institutional Ethics Committee of Jawaharlal Nehru Medical College, Belagavi (Ref. No. MDC/JNMC/IEC/441, dated 24/08/2024). Written informed consent was obtained from all participants prior to data collection. Administrative permission was also secured from the office of the Deputy Commissioner of Police, Belagavi.
All participants underwent a standardized interview, anthropometric assessment, and questionnaire-based evaluation. Trained investigators conducted face-to-face interviews in Kannada or English, as per participant
Study Variables:
1. Data on socio-demographic and occupational characteristics
were collected using a pre- tested, interviewer-administered
questionnaire. Participants were asked to report their age
(in completed years), gender, and religious affiliation.
Occupational data included the current designation or cadre
(e.g., constable, head constable, assistant sub- inspector),
as well as the total number of years in service. Participants
were asked about any existing medical conditions, including
diagnosed chronic diseases (e.g., hypertension, diabetes,
joint disorders), and whether they were currently receiving
treatment or taking medications. Dietary preferences were
documented and categorized as vegetarian, ovo-vegetarian,
or non-vegetarian.2. Nutritional Status Assessment:
a. Anthropometric assessments were conducted following
the WHO STEPS protocol to evaluate participants’
general and central adiposity. Body weight was measured
to the nearest 0.1 kg using a calibrated digital scale, with
participants in light clothing and no footwear. Height was
recorded to the nearest 0.1 cm using a non-stretchable
measuring tape. Body mass index (BMI) was calculated
as weight in kilograms divided by the square of height in
meters (kg/m²) and categorized according to the WHO
Asia-Pacific guidelines: underweight (<18.5), normal
(18.5–22.9), overweight (23–24.9), obese class I (25–29.9),
and obese class II (≥30) [7]. Waist circumference (WC)
was measured at the midpoint between the lower margin
of the last palpable rib and the top of the iliac crest at the
end of expiration. Hip circumference (HC) was measured
at the point of maximum protrusion of the buttocks.
Waist-hip ratio (WHR) was calculated (WC ÷ HC), with
cut-offs of >1.0 for males and >0.8 for females indicating
central obesity [14]. Neck circumference was recorded
just below the laryngeal prominence with participants
seated upright [8].b. Dietary Assessment: Two tools were used to assess dietary
intake. A 3-day 24- hour dietary recall was administered
to capture food and beverage consumption over two
weekdays and one weekend day. Standard utensils,
measuring cups, and visual charts were used to improve
portion estimation. Nutrient composition
C. (energy, protein, fat, carbohydrates) was calculated using
the Indian Food Composition Table 2017 [9], and an
average of the three days was used for analysis. In addition,
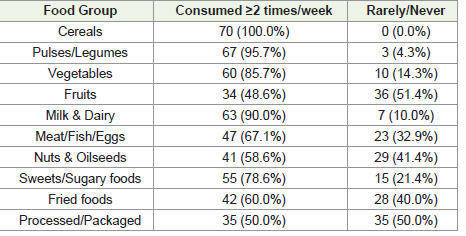
a semi-quantitative food frequency questionnaire (FFQ)
was used to assess habitual intake of key food groups
including cereals, pulses, vegetables, fruits, milk and dairy,
meat, nuts, and oils. Intake frequency was categorized as
daily, 2–3 times per week, weekly, occasionally, or never.
A Food Diversity Score was calculated based on the
number of food groups consumed at least twice per week,
with scores categorized as poor (1–3), average (4–6), or
good (7–10) [10].
3. Health Outcomes Assessment:
a. Work Ability Index (WAI): Work ability was assessed
using the validated Work Ability Index, which evaluates
an individual’s capacity to perform work in relation to
job demands, physical and mental resources, and existing
health conditions. The total WAI score ranges from 7 to
49, and is classified as poor (7–27), moderate (28–36),
good (37–43), or excellent (44–49) [11].b. Perceived Stress Scale (PSS-10): Stress levels were assessed
using the 10-item Perceived Stress Scale, which measures
perceived stress over the previous month. Responses are
rated on a 5-point Likert scale (0–4), with total scores
ranging from 0 to 40. Scores were categorized as low (0–
6), moderate (7–13), and high (≥14) [12].
c. Pittsburgh Sleep Quality Index (PSQI): Sleep quality was
evaluated using the PSQI, which measures subjective
sleep quality across seven domains. The global score
ranges from 0 to 21, with a score >5 indicating poor sleep
quality [13].
d. International Physical Activity Questionnaire – Short
Form (IPAQ-SF): Physical activity levels were assessed
using the short form of the IPAQ, which captures
walking, moderate, and vigorous activity over the past
7 days. Total activity was converted into MET-minutes
per week and categorized as low (<600 MET-min/week),
moderate (600–1499), or high (≥1500) [14].
Data were entered into Microsoft Excel and analysed using IBM
SPSS Statistics version 29. Descriptive statistics (means, standard
deviation, proportions) were calculated. Pearson’s correlation test
was used to analyse relationships between dietary intake and BMI.
Chi-square tests were used to determine associations between
categorical variables (e.g., food group intake vs. BMI categories). A
p-value of <0.05 was considered statistically significant.
Results
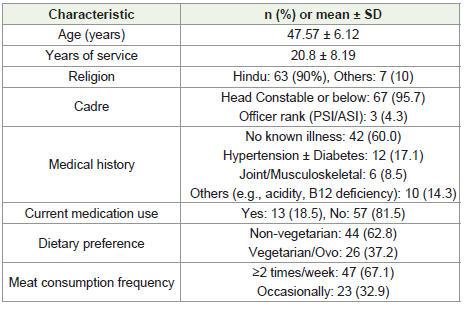
Categories with <5% frequency were merged into ‘Others’ for
clarity. **
The mean age of the participants was 47.6 years, with an average
of 20.8 years of service. Nearly all were in lower to mid-level traffic
policing roles. A majority (60%) reported no known chronic illness;
however, around 17% had hypertension or diabetes, and nearly
one in five were on regular medications. Non-vegetarian diets were
predominant (63%), with two- thirds of non-vegetarian participants
consuming meat more than twice a week. [Table 1]
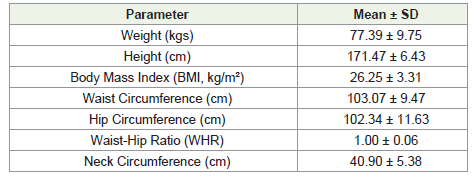
The anthropometric assessment revealed that the mean weight of
the participants was 77.39 ± 9.75 kg, and the mean height was 171.47
± 6.43 cm. The calculated mean BMI was 26.25 ± 3.31 kg/m², placing
the average participant in the overweight category as per WHO Asia-
Pacific classification. Waist and hip circumferences were 103.07 ±
9.47 cm and 102.34 ± 11.63 cm, respectively, with a mean waist-hip
ratio (WHR) of 1.00 ± 0.06. This WHR exceeds the cut-off for central
obesity (>1.0 for males), indicating a high prevalence of abdominal
adiposity among the participants. Additionally, the average neck
circumference was 40.90 ± 5.38 cm, further suggesting elevated risk
for cardiometabolic conditions, as increased neck circumference has
been linked to insulin resistance and obstructive sleep apnea in several
occupational studies. Overall, these findings reflect a significant
burden of both general and central obesity in the study. [Table 2]
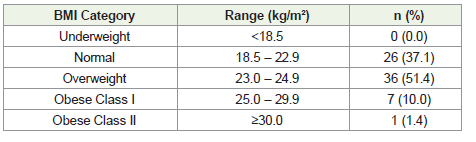
Classification based on WHO Expert Consultation for Asian
Populations (2004) (Ref. 6).
According to WHO classification for Asian populations, more than half of the participants (51.4%) were overweight, and an additional 11.4% were obese (Class I and II combined). No participants were under-weight. These findings reinforce the elevated
According to WHO classification for Asian populations, more than half of the participants (51.4%) were overweight, and an additional 11.4% were obese (Class I and II combined). No participants were under-weight. These findings reinforce the elevated
risk of cardiometabolic conditions in this occupational group.
[Table 3]
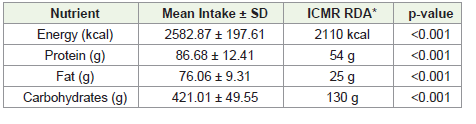
*RDA values based on ICMR-NIN guidelines for moderately active Indian adult males [15].
*RDA values based on ICMR-NIN guidelines for moderately active Indian adult males [15].
The mean energy intake among participants was 2582.87 kcal/
day, which significantly exceeded the recommended level of 2110
kcal for moderately active adult males (p < 0.001). Similarly, the
intake of all macronutrients, protein (86.68 g), fat (76.06 g), and
carbohydrates (421.01 g) was considerably higher than ICMRNIN
recommended dietary allowances, with statistically significant
differences (p < 0.001 for all). [Table 4] seen for nuts and oilseeds
(58.6%), while intake of fried and processed foods was relatively high
(60% and 50%, respectively). These findings suggest a carbohydratedense
but micronutrient-poor dietary pattern, which may contribute
to excess energy intake without corresponding dietary quality. The
low frequency of fruit and nut intake also aligns with the observed
low dietary diversity scores in a significant proportion of participants.
[Table 5]
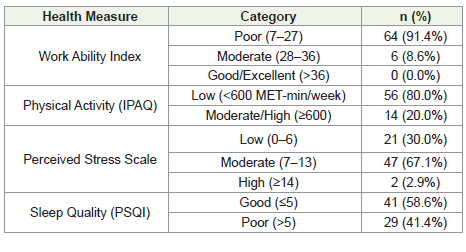
Work performance was notably compromised, with 91.4% of
participants categorized as having poor work ability scores, and none
scoring in the good or excellent range. Low physical activity levels
were reported by 80% of participants, further compounding health
risks. Regarding psychological health, the majority (67.1%) reported
moderate stress levels, and 41.4% had poor sleep quality based on the
PSQI. These findings suggest a substantial burden of occupational
and lifestyle-related health challenges among traffic police personnel,
which may impact both their well being and work efficiency. [Table 6]
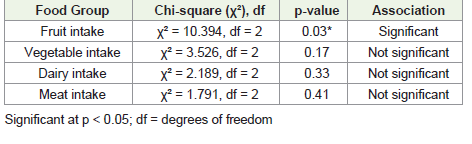
Fruit intake showed a statistically significant association with
BMI categories (χ² = 10.394, df = 2, p = 0.03), suggesting that higher
fruit intake was more common among participants with normal BMI.
No significant associations were observed between BMI and intake of
vegetables, dairy, or meat.
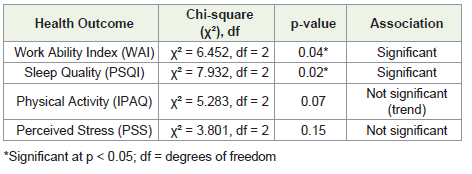
There was a statistically significant association between BMI
and work ability (p = 0.04), with overweight and obese participants
more likely to report poor work ability scores. Similarly, a significant
relationship was observed between BMI and sleep quality (p = 0.02),
indicating that those with higher BMI were more prone to poor sleep
patterns. No statistically significant associations were found between
BMI and perceived stress or physical activity levels, although the
relationship with physical activity showed a non-significant trend.
Discussions
This study assessed the nutritional status and health outcomes
of traffic police personnel in Belagavi, India. The findings reveal a
significant burden of overweight and central obesity, excessive caloric
intake, low dietary diversity, and poor health outcomes related to
work ability, physical activity, stress, and sleep. These findings align
with concerns reported in occupational health literature regarding
law enforcement personnel in India and other low- and middle income
settings.
The mean BMI in this study (26.25 ± 3.31 kg/m²) placed the
average participant in the overweight category according to WHO
Asia-Pacific guidelines [7]. More than 62% of participants were
overweight or obese. This is consistent with earlier studies. [1,16]
which also found high rates of overweight among Indian police
officers. Similarly, Wirth et al. [2] reported elevated BMI and
metabolic risk in American law enforcement populations. The high
prevalence of central obesity, as indicated by waist circumference
and WHR, further underscores the cardiometabolic risk in this
population. These findings mirror those of Santana et al. [5], who
reported similar anthropometric trends among Brazilian military
police. Elevated neck circumference in our study, a lesser-used but
emerging predictor of metabolic risk and sleep apnea, also supports
the growing evidence of hidden adiposity in seemingly mobile
occupational roles.
Dietary assessment revealed that while total energy and
macronutrient intake far exceeded ICMR recommendations, only
8.6% of participants had good dietary diversity. These results are
consistent with Kayapinar and Savas [4], who found that police
personnel often consume high-calorie but low-nutrient-density diets
due to irregular work hours and poor access to balanced meals. The
inverse association between fruit intake and BMI observed in our
study (p = 0.03) is in line with prior findings linking low fruit and
fiber intake to increased body weight [17].
The occupational health outcomes further emphasize the
physiological and psychological burden in this workforce. Over
90% of participants scored poorly on the Work Ability Index.
Among participants with a moderate workload, 84.4% experienced
moderate fatigue, n=34(84.4%) experienced moderate fatigue, while
n=6(15.2%) reported mild fatigue. In comparison, n=23(57.1%)
of those with a low workload experienced moderate fatigue, and
n=17(42.9%) reported mild fatigue [18].
Sleep quality was poor in 41.4% of participants and was
significantly associated with BMI (p = 0.02). While moderate to
high perceived stress was present in most participants (67.1%), the
association with BMI was not statistically significant.
Despite traffic policing being a mobile job, 80% of participants reported low physical activity levels per IPAQ scoring. A study done by Shweta et al. reported high prevalence of Musculo skeletal pains among Traffic Police Personnel’s.
Despite traffic policing being a mobile job, 80% of participants reported low physical activity levels per IPAQ scoring. A study done by Shweta et al. reported high prevalence of Musculo skeletal pains among Traffic Police Personnel’s.
Limitations:
This study is limited by its cross-sectional design, which precludes
causal inference. Dietary data relied on self-reported recall, which
may be subject to under- or overestimation. The use of convenience
sampling limits generalizability beyond Belagavi traffic policeConclusion
Traffic police personnel in Belagavi demonstrate a high burden
of overweight, inadequate dietary quality, low physical activity, and
compromised work-related health. Associations between BMI, work
ability, and sleep highlight the importance of integrated occupational
health interventions, including nutrition education, structured
physical activity programs, and stress/sleep management strategies.
References
Citation
Pirjade S, Kour H. Nutritional Status and Health Outcomes Among Traffic Police in Belagavi, India: A Cross-Sectional Study. Indian J Nutri. 2025;12(2): 320.