View Point
India’s Dual Burden of Overweight/Obesity and Anemia: A Viewpoint on Trends, Determinants, and Policy Implications
Anita Khokhar
Director Professor & Head, Department of Community Medicine, Vardhman Mahavir Medical College & Safdarjung Hospital, New
Delhi-110029, India
*Corresponding author:Dr. Anita Khokhar, Director Professor & Head, Department of Community Medicine, Vardhman Mahavir Medical College & Safdarjung Hospital, New Delhi-110029, India. E-mail Id: anitakh1@yahoo.com
Article Information: Submission: 14/05/2025; Accepted: 15/07/2025; Published: 17/07/2025
Copyright: © 2025 Khokhar A. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
India is facing a unique public health crisis characterized by the simultaneous prevalence of overweight/obesity and anemia, especially among women, children, and adolescents. This dual burden of malnutrition poses significant challenges to health systems, as it affects both communicable and noncommunicable diseases. The National Family Health Survey (NFHS), National Health Profile (NHP), and National Institute of Nutrition (NIN) reports indicate that while overweight and obesity rates have risen, anemia remains widespread. This viewpoint explores the trends, gender and age-wise comparisons, and underlying determinants of these two conditions. It also discusses government interventions such as Anemia Mukt Bharat (AMB) and POSHAN Abhiyaan. Finally, the paper offers recommendations focused on integrated health and nutrition strategies, multisectoral coordination, and community-based interventions to address this dual burden effectively.
Keywords:Obesity; Anemia; India; Public Health; Malnutrition
Introduction
India is undergoing a complex nutrition transition, shifting from
undernutrition to a dual burden of overnutrition and micronutrient
deficiencies. This dual burden manifests as rising obesity alongside
persistently high anemia rates, especially among women of
reproductive age, adolescents, and children. The co-occurrence
of these conditions exacerbates both communicable and noncommunicable
disease burdens. This viewpoint article examines the
magnitude, determinants, and policy response to the dual burden of
obesity and anemia in India.
Magnitude and Trends
Determinants of the Dual Burden:
Dietary Transition: India’s nutritional landscape is characterized
by a shift towards calorie-dense, nutrient-poor diets. A decrease in
consumption of iron-rich foods—such as green leafy vegetables,
legumes, and animal sources—alongside increased intake of processed
and fried foods has contributed to both obesity and iron-deficiency
anemia (Misra et al., 2019) [1].Physical Inactivity:
Rapid urbanization and sedentary lifestyles, particularly among
youth and working adults, have led to a significant decrease in
physical activity, exacerbating overweight and obesity rates.Iron Metabolism and Obesity-Related Inflammation:
Recent studies emphasize that obesity induces chronic low-grade
inflammation, impairing iron metabolism through the hepcidin
pathway. Hepcidin, produced in response to inflammation, reduces
dietary iron absorption and impairs iron release from stores, leading
to functional iron deficiency despite adequate intake (Cepeda-Lopez
et al., 2019; Zhao et al., 2019; Qin et al., 2023) [2-4].Gender and Socioeconomic Inequities:
Women and adolescent girls in lower socioeconomic groups face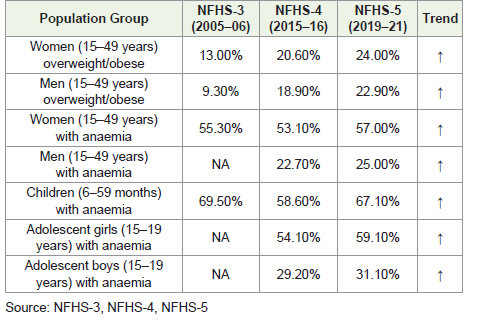
greater risks due to gender-based dietary restrictions, menstruation,
early pregnancies, and poor healthcare access. Boys, though less
affected, also show a rising anemia prevalence.
Scientific Evidence on the Obesity-Anemia Link:
Emerging evidence supports a bidirectional link between obesity
and anemia. Miao et al. (2022) [5] reported that overweight individuals
are more likely to consume nutrient-deficient foods, displacing ironrich
sources. Wang et al. (2020) [6] found that obese adolescent girls
were more prone to iron deficiency anemia, likely due to chronic
inflammation and irregular dietary patterns. Meta-analyses by Qin et
al. (2023) [4] further affirm the role of obesity-induced inflammation
and impaired iron homeostasis across age groups.Government Interventions and Their Evaluation
Anemia Mukt Bharat (AMB): AMB was launched in 2018 with a target to reduce anemia in women, children, and adolescents by
3% per year. Despite interventions like IFA supplementation and
deworming, NFHS-5 data show increasing anemia prevalence in
several target groups. Evaluation studies indicate challenges in IFA
compliance, irregular supply chains, and lack of awareness (MoHFW,
2021) [7-11].
POSHAN Abhiyaan: POSHAN Abhiyaan targets undernutrition
through cross-sector convergence. Though it promotes food
fortification and improved health delivery, it lacks a robust focus on
obesity or double-duty actions. Monitoring indicators remain more
undernutrition-centric.
Challenges in Implementation
• Logistical Barriers: Supply chain inefficiencies limit IFA tablet availability.
• Program Fragmentation: Multiple schemes operate in silos, reducing synergy.
• Obesity Neglect: No major policy yet addresses adolescent or adult obesity systematically.
• Monitoring Gaps: Weak program data limits real-time correction and planning.
• Logistical Barriers: Supply chain inefficiencies limit IFA tablet availability.
• Program Fragmentation: Multiple schemes operate in silos, reducing synergy.
• Obesity Neglect: No major policy yet addresses adolescent or adult obesity systematically.
• Monitoring Gaps: Weak program data limits real-time correction and planning.
Implications of the Dual Burden:
•Increased NCD Risk: Obese individuals with anemia have
higher risks of metabolic syndrome and cardiovascular
disease.• Maternal and Child Health: Anemia and obesity during pregnancy increase complications, including gestational diabetes and poor fetal growth.
• Economic Cost: Productivity loss, healthcare expenditure, and morbidity together impose significant economic burdens.
Recommendations
1. Promote Double-Duty Actions: Design nutrition programs that concurrently address both
anemia and obesity. Example strategies include fortifying low-calorie
staple foods with iron and incentivizing physical activity in schools.
2. Reform Existing Programs:
Update AMB and POSHAN Abhiyaan to include obesity
surveillance and control measures. Integrate nutrition and lifestyle
counseling into school health programs and urban health missions.3. Policy Reforms: Regulate marketing of high-fat, high-sugar foods. Introduce
front-of-pack labelling and strengthen FSSAI’s food fortification and
labelling mandates. Revamp the Public Distribution System (PDS)
to include fortified staples and reduce overdependence on refined
grains.
4. Enhance Multisectoral Convergence:
Encourage coordination among the Ministries of Health, Women
and Child Development, and Education. Deploy common indicators
for monitoring anemia and obesity under shared platforms.5. Community-Level Approaches:
Strengthen peer education, adolescent-friendly clinics, and
school-based deworming and nutrition programs. Mobilize frontline
workers (ASHA, AWWs) to conduct lifestyle counselling and
nutrition education.Conclusion
India’s public health landscape is at a crossroads, with
undernutrition and overnutrition coexisting dangerously. The rising
prevalence of both anemia and obesity—especially among women
and children—requires urgent, evidence-based, and multisectoral
action. Existing programs must be realigned to adopt doubleduty
strategies and strengthen community delivery mechanisms.
Long-term improvement in public health outcomes depends on
sustained investment in nutrition-sensitive interventions, proactive
policymaking, and community engagement.
References
Citation
Khokhar A. India’s Dual Burden of Overweight/Obesity and Anemia: A Viewpoint on Trends, Determinants, and Policy Implications. Indian J Nutri. 2025;12(2): 319.