Research Article
A Nationwide Multicentric, in-Clinic, Observational Study on ChilRun full™: Real-World Effectiveness Data on Growth and Development in Indian Children
Jain Naveen K*, Dheeraj K, Amera K and Patil Chandrashekhar S
Department of Biology Research/New Products, Panacea Biotec Ltd., B-1 Extn. /A-27 Mohan Co-operative industrial Estate, Mathura Road, New Delhi, India
*Corresponding author:Naveen K Jain, Vice President- Biology Research/New Products,Panacea Biotec Ltd., B-1 Extn./A-27 Mohan Co-operative industrial Estate, Mathura Road, New Delhi, India. Email: naveenjain@panaceabiotec.com
Article Information:Submission: 17/04/2025; Accepted: 09/05/2025; Published: 12/05/2025
Copyright: © 2025 Jain Naveen K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:Malnutrition, encompassing undernutrition and micronutrient deficiencies, poses a significant threat to public health and it is a leading cause of kid’s growth restriction in formative years (2-12 years). Stunting and wasting, prevalent manifestations of malnutrition, have far-reaching consequences, impacting physical growth, cognitive development and overall well-being. Addressing this critical public health challenge necessitates effective nutritional interventions that not only alleviate immediate nutritional deficits but also resolve long-term growth, metabolic and development issues. The current study investigated the efficacy and safety of ChilRun full™, a commercially available oral nutritional supplement (ONS), in improving growth parameters among Indian children aged 2+ years.
Methods: The post-marketing, multicentric, in-clinic observational study was performed to evaluate the effectiveness and safety of ChilRun full™, a commercially available ONS, on the growth and development of children aged 2 years and above across India. A total of 3307 children were initially enrolled for this study and 2851 children successfully completed 90-day study period (day 0, 30, 60 and 90 days visit) Anthropometric measurements, including height, weight and body mass index (BMI), were recorded at four different time points baseline (day 0), day 30, 60 and 90. Children received two daily servings of ChilRun full™ for the entire 90-day study period. Growth parameters and Z-scores were analysed to assess the impact of ChilRun full™ on growth parameters. Focused analysis on the special population was conducted on children with baseline Z-scores ≤ -1, representing a subgroup at risk of malnutrition, to evaluate the effectiveness of ChilRun full™ in addressing growth deficiencies.
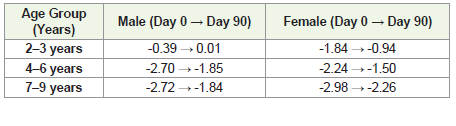
Results:Continuous supplementation with ChilRun full™ (twice a day for 90 days) led to significant improvements in anthropometric parameters height, weight and BMI across all age groups, with the 2-3 years group showing gain in height (2.20%), weight (9.68%) and BMI (4.82%) by end of day 90. Similarly, children aged 4-6 years and 7-9 years also showed substantial increase in height, weight and BMI. Further, in the subgroup analysis in children at the risk of malnutrition (Z-score ≤-1), weight increased by 20.56%, height by 10.30% and BMI by 14.36%, demonstrating effectiveness of ChilRun full™ in addressing growth deficits. Z-score analysis showed a positive shift towards standardized growth norms. Among children 2–3-year age, Z-scores for weight percentile improved from -0.39 to 0.01 in males and -1.84 to -0.94 in females, while, in children age 4–6-year, Z-scores increased from -2.70 to -1.85 in males and -2.24 to -1.50 in females and for 7–9-year age children from -2.72 to -1.84 in males and -2.98 to -2.26 in females. By the end of day 90, a significant number of children in both sexes from severely underweight (below the 3rd percentile) category moved to higher weight categories, demonstrating improved weight and a positive shift in nutritional status. The maximum shift was seen in children below the 3rd percentile, with 111 males and 73 females moving to the 3rd–15th percentile. Z-scores for height, weight and BMI showed positive shifts towards the standard population norms, indicating a normalization of growth patterns.
Conclusion:These findings highlight the efficacy of ChilRun full™ in promoting healthy growth and addressing malnutrition, as evidenced by improvements in weight, height, BMI, Z-scores and weight percentile distributions across all age groups and provides a strong nutritional foundation in growing kids to transform them into healthy, energetic and strong kids.
Methods: The post-marketing, multicentric, in-clinic observational study was performed to evaluate the effectiveness and safety of ChilRun full™, a commercially available ONS, on the growth and development of children aged 2 years and above across India. A total of 3307 children were initially enrolled for this study and 2851 children successfully completed 90-day study period (day 0, 30, 60 and 90 days visit) Anthropometric measurements, including height, weight and body mass index (BMI), were recorded at four different time points baseline (day 0), day 30, 60 and 90. Children received two daily servings of ChilRun full™ for the entire 90-day study period. Growth parameters and Z-scores were analysed to assess the impact of ChilRun full™ on growth parameters. Focused analysis on the special population was conducted on children with baseline Z-scores ≤ -1, representing a subgroup at risk of malnutrition, to evaluate the effectiveness of ChilRun full™ in addressing growth deficiencies.
Results:Continuous supplementation with ChilRun full™ (twice a day for 90 days) led to significant improvements in anthropometric parameters height, weight and BMI across all age groups, with the 2-3 years group showing gain in height (2.20%), weight (9.68%) and BMI (4.82%) by end of day 90. Similarly, children aged 4-6 years and 7-9 years also showed substantial increase in height, weight and BMI. Further, in the subgroup analysis in children at the risk of malnutrition (Z-score ≤-1), weight increased by 20.56%, height by 10.30% and BMI by 14.36%, demonstrating effectiveness of ChilRun full™ in addressing growth deficits. Z-score analysis showed a positive shift towards standardized growth norms. Among children 2–3-year age, Z-scores for weight percentile improved from -0.39 to 0.01 in males and -1.84 to -0.94 in females, while, in children age 4–6-year, Z-scores increased from -2.70 to -1.85 in males and -2.24 to -1.50 in females and for 7–9-year age children from -2.72 to -1.84 in males and -2.98 to -2.26 in females. By the end of day 90, a significant number of children in both sexes from severely underweight (below the 3rd percentile) category moved to higher weight categories, demonstrating improved weight and a positive shift in nutritional status. The maximum shift was seen in children below the 3rd percentile, with 111 males and 73 females moving to the 3rd–15th percentile. Z-scores for height, weight and BMI showed positive shifts towards the standard population norms, indicating a normalization of growth patterns.
Conclusion:These findings highlight the efficacy of ChilRun full™ in promoting healthy growth and addressing malnutrition, as evidenced by improvements in weight, height, BMI, Z-scores and weight percentile distributions across all age groups and provides a strong nutritional foundation in growing kids to transform them into healthy, energetic and strong kids.
Keywords:ChilRun full™; Child Growth; Malnutrition; Nutritional Supplement; Anthropometry; Observational Study.
Introduction
Childhood malnutrition remains among one of the most pressing
global public health challenges, affecting nearly one-third of the
world’s population including India. Micronutrient deficiencies,
or “hidden hunger” severely impact the growth and development
and it further contributes to the broader issue of malnutrition. The
consequences are significant, affecting children’s health (including
under nutrition- wasting, stunting and underweight), education
(school missing days) and future potential, advocating the urgent
need for targeted interventions [1].Various studies have indicated
that adequate nutrition and healthy growth in the first 1000 days of life
is crucial and contributes to long-term health benefits in adulthood.
Administration of nutritional interventions to undernourished
children can promote catch-up growth more effectively and prevent
growth faltering [2,12].
Despite advancements in healthcare, millions of children
worldwide still suffer from undernutrition, which can severely impact
their growth, immunity and cognitive development. According to
“UNICEF/ WHO/World Bank Group report 2023” an estimated 148.1
million children under five years suffered from stunting, 45 million
from wasting and 37 million from being overweight [3]. According
to the National Family Health Survey (NFHS-5) report 35% of Indian
children under five years are stunted, 19% are wasted and 32% are
underweight. These alarming numbers reflect acute and chronic
forms of undernutrition that not only affect physical growth but also
have long-term impacts on brain development, learning abilities,
immunity and overall well-being due to poor dietary diversity and
inadequate feeding practices [4].
A major contributor to this global situation is micronutrient
deficiency. Children’s diets in many low-income areas are mostly
starchy, staples and lack protein or micronutrient diversity (vitamins
and minerals). The deficiency of vital nutrients, such as iron, vitamin
A, zinc and iodine is a common issue that can slow down growth
and development and these deficiencies can go unnoticed for a
long time but lead to serious health consequences like anemia, poor
concentration, frequent infections and developmental delays/bone
disorders. Children with inadequate micronutrient intake often fall
behind in school, face higher risks of illness and struggle to reach
their full physical and mental potential [5].
Further the prevalence of childhood obesity/overweight is also
increasing at an alarming rate. According to the WHO report 37
million children under the age of 5 years were overweight and over
390 million children and adolescents aged 5–19 years were overweight
in 2022, including 160 million who were living with obesity [6,11].
This situation leads to various issues like psychological challenges not
only in the quality of life of parents but at school level (i.e. stigma,
discrimination and bullying behavior). Therefore, this issue needs to
be tackled at community level with better nutritional awareness and
related Nutraceutical products [7].
A variety of commercial Oral Nutritional Supplements (ONS)
are used clinically to promote catch-up growth in children with
undernutrition. Over the years ONS have emerged as a practical and
a convenient solution for nutritional enrichment along with regular
meals. When provided alongside regular meals, ONS helps to fill the
nutritional gaps, especially in children who are picky/fussy eaters,
recovering from illness, or living in food-insecure environments.
Clinical studies have shown that ONS, when combined with dietary
counseling, significantly improves height-for-age and weight-forage
scores, enhances attentional focus and reduces the frequency of
infections. In particular, they support catch-up growth in children
beyond the first 1,000 days, a critical window where early intervention
can reverse or reduce the long-term effects of malnutrition [8,9].
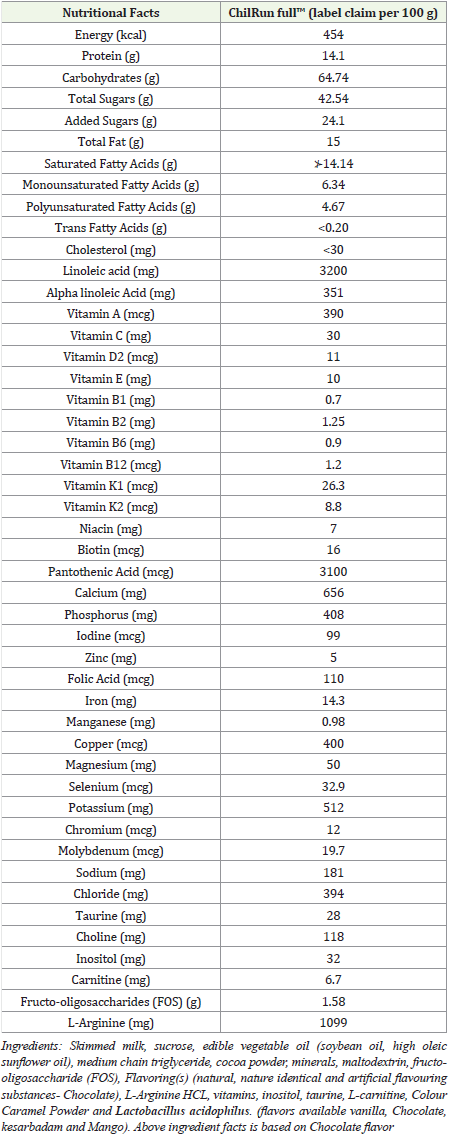
ChilRun full™, is a scientifically formulated Oral Nutritional
Supplement, designed to be an additional source of nutrition to
overcome the nutrition gap for growing children. It provides the
right blend of macronutrients and micronutrients (essential vitamins
and minerals) and functional ingredients (37 essential key nutrients)
to support physical and cognitive development and essential
for the critical growth, developmental and nutritional aspects
of transformative childhood years. ChilRun full™ also addresses
both visible and hidden hunger by bridging nutritional gaps in
everyday diets, especially in children who are picky/fussy eaters,
undernourished, or recovering from illness [10]. This in-clinic multicentric,
non-randomized, nationwide observational study, was aimed
to evaluate the effect of ChilRun full™ (scientifically designed with 37
key nutrients based ONS) on the growth and development of children
(2851 kids from all over the India), aged 2 years and above over a
three-month period along with a regular diet.
Materials and Methods
Study Design:
The post-marketing, multicentric, in-clinic observational
study was performed to evaluate the effectiveness and safety of
ChilRun full™, a commercially available ONS, on the growth and
development of children aged 2 years and above across India. A
total of 3307 children were initially enrolled for this study and 2851
children successfully completed the full 90-day study period. The
completed group comprised 1650 boys and 1201 girls, thus providing
a well-distributed demographic representation across genders for
comprehensive analysis [Figure 1] [Table 1]. This observational study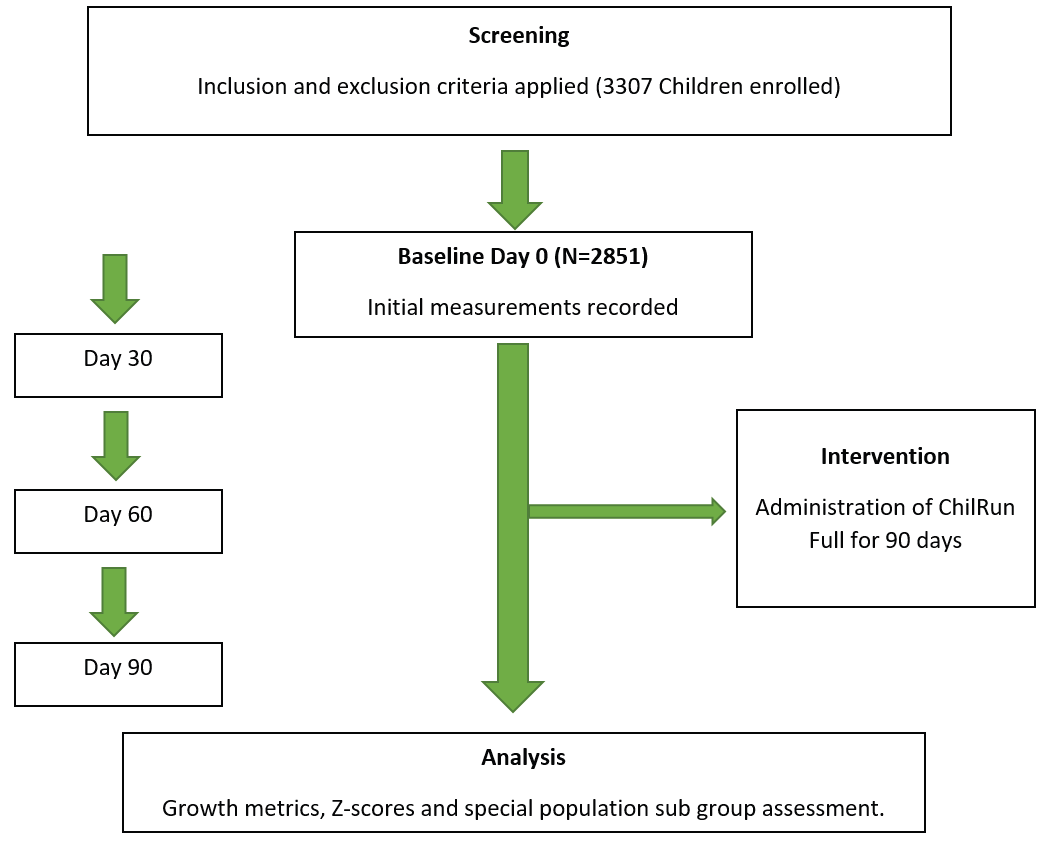

was performed at 282 clinics across 32 cities (Asansol, Bangalore,
Bareilly, Balasore, Bhubaneswar, Burdwan, Cuttack, Dehradun,
Delhi, Faridabad, Ghaziabad, Gorakhpur, Guwahati, Hyderabad,
Kanpur, Kolkata, Lucknow, Madurai, Medak, Mumbai, Nashik,
Patna, Pune, Ranchi, Siddhipet, Sivagangai, Thane, Varanasi, Vizag)
in India from 1st January 2024 to 31st Oct 2024 and was subjected for
analysis.
Study Population:
Children aged 2 years and above with regular eating habits
were enrolled across 282 sites under pediatrician supervision. Each
investigating pediatrician enrolled minimum 10 to 12 kids at their
respective clinics. Children enrolled in the study (n=2851) were
divided into three distinct age groups, each representing different
stages of childhood development. The youngest cohort, comprising
children aged 2-3 years (n=877), accounted for 30.8% of the study
population. This group is characterized by rapid growth and
heightened nutritional requirements, making it a critical period for
interventions aimed at supporting physical development. The largest
group, consisting of children aged 4-6 years (n=1670), represented
58.6% of the study population. These children were primarily in the
preschool and early school years, a phase marked by steady growth
and increasing physical and cognitive demands. Finally, the 7-9-year olds
(n=304) accounted for 10.7% of the study population. This
cohort included older children approaching late childhood, a stage
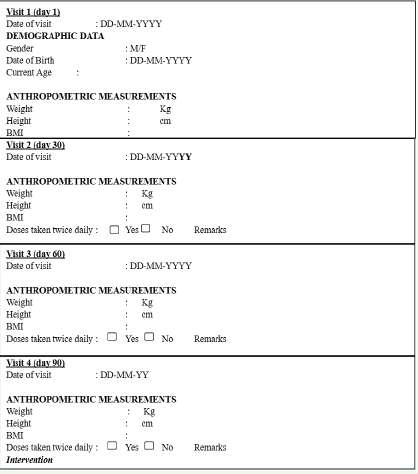
where growth rates typically stabilize [Figure 2].Anthropometric measurements in terms of weight, height and
BMI were measured during the visits on day 0 (baseline), 30, 60 and
90 (end of the study period) as per the Case Report Form (CRF).
The Z-score for height, weight and BMI was used to analyze the
results using Khadilkar (2015) growth chart [13]. All measurements
were performed by clinical/nursing staff (under the supervision of
pediatricians) using the standardized methods and data was captured
in the CRF as per protocol [Figure 3].
Inclusion and Exclusion Criteria:
Each child was included in the study following specific inclusion
criteria, ensuring uniformity and reliability of the data collected.
Data from children were included in the study analysis if they
had completed CRFs, documenting their height, weight and BMI
at all four measurement points: day 0, day 30, day 60 and day 90.
Children were excluded from participation if they had any of the
following conditions: 1. Concomitant systemic infections, clinically
significant diseases, stomach infections, infestations, or suspected
liver disorders. 2. Diagnosed lactose intolerance, galactosemia, or
other medical conditions that might interfere with the study product,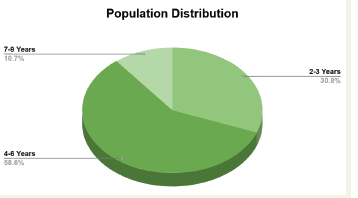
as identified through medical records or parent/guardian reports.
3. Known allergies or intolerances to any ingredient in ChilRun
full™. This rigorous screening ensured that the sample consisted of
children who could safely consume the supplement without medical
contraindications.
Intervention:
Eligible children received twice daily servings of ChilRun full™
(Manufactured by Panacea Biotec Pharma Ltd., New Delhi; FSSAI
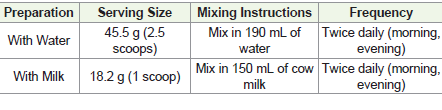
approved) as per label claim every day for 3 months as per [Table 2].
Parents were provided detailed instructions on the preparation and
administration of the supplement as per [Table 3].Parents were advised to administer the ChilRun full™ (twice daily)
in morning and evening, depending on their routine. This consistent
administration ensured adequate nutrient intake for optimal results.
All measurements were performed by clinical/nursing staff (under
the supervision of pediatricians) and data was captured in the CRF as
per protocol during the visits scheduled at day 0, 30, 60 and 90 post
enrollment.
Safety and tolerability, was reported by parents and caregivers to
supervising pediatricians, if any.
Data Analysis:
The data collected from enrolled children via CRF were
systematically analyzed to evaluate the effectiveness of ChilRun full™
in improving growth parameters.Growth Metrics:Average height, weight and BMI were calculated for each age group at each time point (day 0, 30, 60 and 90). The percentage increase over the 90-day period was determined to assess the supplement’s impact. Z-Score Analysis: Z-scores for height, weight and BMI were calculated at baseline and Day 90 using the Khadilkar (2015) growth chart. Improvements in Z-scores were analyzed and graphically represented to illustrate growth normalization relative to standard populations [13].
Weight Percentile Analysis:Using the IAP growth chart (2015), weight-for-age percentiles were calculated and categorized into four groups: below the 3rd percentile, 3rd-15th percentile, 15th- 50th percentile and 50th-85th percentile [14]. Changes in weight percentile distribution were analyzed to assess shifts toward healthier weight categories over the 90-day period.
Special Population Analysis:A focused analysis was conducted on children with baseline Z-scores ≤ -1, representing those at risk of malnutrition. Changes in height, weight, BMI and Z-scores were quantified and percentage improvements were compared to the general population to evaluate the impact of supplementation in addressing growth deficits.
Statistical Analysis The results were presented visually using the table and bar graphs to depict average changes in height, weight and BMI for each age group. Bar graphs were used to track Z-scores improvements for the overall cohort and the special population.
Results
The present study evaluated the impact of ChilRun full™, a
specially formulated ONS, on the growth and development of 2851
children aged 2 years and above over a 90-day period. ChilRun full™ is
fortified with a balanced mix of macronutrients, micronutrients and
functional ingredients, including proteins, carbohydrates, fats and
critical vitamins and minerals. Its composition is designed to address
nutrient deficiencies and support optimal growth (including healthy,
energetic and strong kids).
The data was obtained from the 282 clinics across 32 cities
(Asansol, Bangalore, Bareily, Balasore, Bhubaneswar, Burdwan,
Cuttack, Dehradun, Delhi, Faridabad, Ghaziabad, Gorakhpur,
Guwahati, Hyderabad, Kanpur, Kolkata, Lucknow, Madurai, Medak,
Mumbai, Nashik, Patna, Pune, Ranchi, Siddhipet, Sivagangai, Thane,
Varanasi, Vizag) across India from 1st January 2024 to 31st Oct
2024 and was subjected for analysis. A total of 3134 children were
enrolled and received the nutritional supplement ChilRun full™ out
of 3134 enrolled subjects 2851 completed the study. Demographics
and baseline characteristics are presented in Table 1. The median age
was 4.8 ± 0.5 years (range 2 - 12 years) and the gender distribution
included 1650 males and 1201 females. None of the children enrolled
had wasted (Z score ≥ -2).
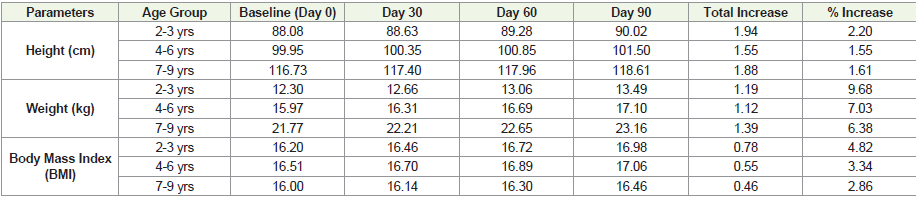
On continuous use of ChilRun full™ changes in height, weight
and BMI were observed on day 30, 60 and 90 [Table 4]. A substantial
increase in all three parameters among all age groups was observed at
the end of 90 days on continuous use of ChilRun full™ (in comparison
to baseline values prior to start of ChilRun full™ initiation). The data
suggest that ChilRun full™ had a positive effect on the growth metrics
on continuous use for 90 days.
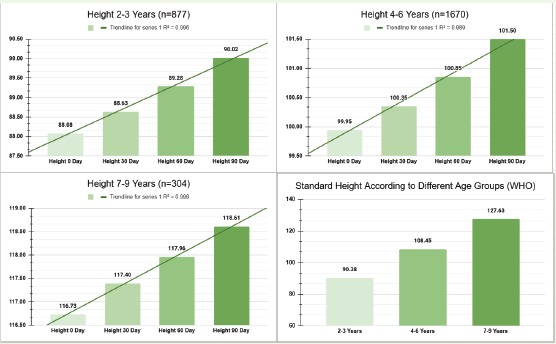
Height: ChilRun full™ exhibited a steady and linear increase
in height across all the age groups. The maximum increase of 2.2%
(88.08 cm at baseline to 90.02 cm on day 90) was seen in children age
2-3 years, followed by 1.55% in 4-6 years (from 99.95 cm to 101.50
cm on day 90) and 1.61% (116.73 cm at baseline to 118.61 cm on
day 90) in 7-9 years age group (Table 4). This increase in height
gain was as per the WHO standard height for different age groups
[Figure 4] and was within the range of baseline height of study
children. Further, trend line, R2 (linear line of regression) was almost
unity for various age groups of 2-3 years, 4-6 years and 7-9 years
was 0.996, 0.989 and 0.999 for height, respectively. These results
indicate that ChilRun full™ positively influences linear growth, a
critical marker of physical development. The steady increases across
age groups suggest the ChilRun full™ applicability in fostering height
gains during childhood.
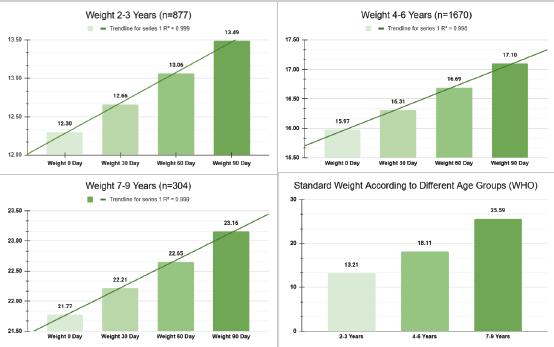
Weight:ChilRun full™ demonstrated a consistent gain in weight
metrics across all the age groups with the youngest children showing
the highest relative increase. The weight increase was 9.68% in 2-3
years age group (1.19 kg increase from 12.30 kg to 13.49 kg), 7.03%
in 4-6 years age (1.12 kg increase from 15.97 kg to 17.10 kg) and
6.38% in 7-9 years age (1.39 kg rise from 21.77 kg to 23.16 kg).
This indicates that the ChilRun full™ supports healthy weight gain,
particularly important in growing children and the standard weight
as per WHO for different age groups was in the range of baseline
weight for enrolled children [Figure 5]. The trend line, R2 (linear
line of regression) for various age groups of 2-3 years, 4-6 years and
7-9 years was 0.999, 0.998 and 0.999 for weight, respectively. The
consistent gains across all age groups reflect the ability of ChilRun
full™ to enhance weight metrics in children in both normal and
nutritionally at-risk populations, contributing to improved overall
health and vitality.
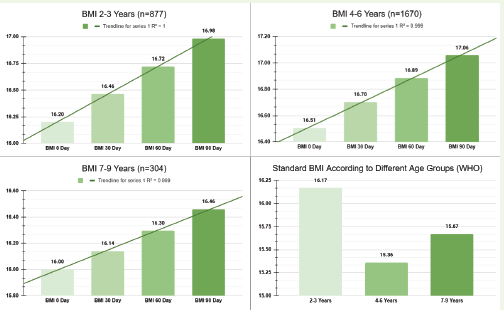
BMI: BMI values showed a positive upward trend, indicating
proportional gain in both height and weight, thereby reflecting
an overall balanced growth supported by ChilRun full™. The BMI
increased by 4.82%, 3.34% and 2.86% in age groups 2-3 years, 4-6
years and 7-9 years, respectively at the end of 90 days (Table 4). The
standard BMI as per WHO for different age groups was within the
range of baseline BMI [Figure 6]. The trend line, R2 (linear line of
regression) for various age groups of 2-3 years, 4-6 years and 7-9 years
was 1.0, 0.999 and 0.999 for BMI, respectively. The increase in BMI
underscores the supplement’s effectiveness in promoting healthy and
proportional growth. The data suggest that ChilRun full™ supports
weight and height increases, while maintaining appropriate BMI,
thereby avoiding the risk of excessive or disproportionate weight gain.
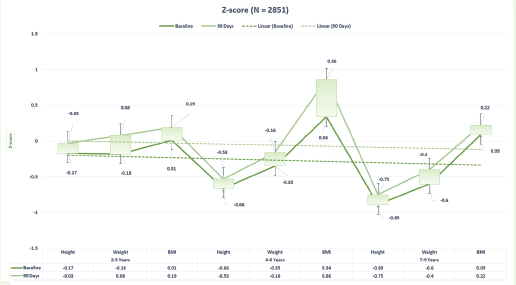
Z-score: ChilRun full™ exhibited a significant improvement in
Z-scores for weight, height and BMI across all the age groups (Figure
7). In children aged 2-3 years the Z-score for height, weight and
BMI improved from -0.17, -0.18 and -0.01 at baseline to -0.03, 0.08
and 0.19 on day 90, respectively. Similarly, the improvement in the
Z-scores was noted in children aged 4-6 years (for height, weight and
BMI from -0.66, -0.35 and 0.34 at baseline to -0.53, -0.16 and 0.86)
and 7-9 years (for height, weight and BMI from -0.89, -0.60 and -0.09
at baseline to -0.75, -0.40 and 0.22) on day 90. The uptrend suggests
ChilRun full™ has the potential to support the optimal growth patterns
in children of all age groups.
Further, on continuous use for 90 days ChilRun full™ was well
tolerated as no adverse events were reported in any age group from
any one of the centers during the study period.
Special Population (Z-Scores ≤ -1):
Subset analysis in special population was conducted for (a)
Z-score analysis for weight, height and BMI in children at risk of
malnutrition (Z-scores ≤ -1) and (b) Gender wise Z-score distribution
based on weight percentile profile(a) Z-score analysis for weight, height and BMI in children
at risk of malnutrition (Z-scores ≤ -1):In a subset analysis Z-score
data from all age groups (2-4 years, 4-6 years and 7-9 years) were
combined. Based on Z-scores ≤ -1, 2094 out of 2851 children were
classified as children at risk of malnutrition based on height (n=934),
weight (n=1009) and BMI (n=151).
Z-score in all age group children increased from -1.88 to -1.69 for
height, -1.75 to -1.35 for weight and -1.40 to -1.20 for BMI (Figure 8).
This change in Z-score for height, weight and BMI was 10.30%, 20.56%
and 14.59%, respectively. These results indicate that children at risk of
malnutrition (Z-scores ≤ -1), on continuous use of ChilRun full™ for
90 days addressed the severe nutritional deficits and promoted catchup
growth during the critical periods of development, thereby, having
profound implications on long-term health, cognitive development
and educational outcomes.
(b) Gender wise Z-score distribution based on weight percentile
profile: To examine gender-based weight percentile profiles, Z-scores
for weight percentile were calculated for 2851 children (1650 males,
1201 females) using the IAP growth chart (2015). The weight for
age data for both male and female was analysed to calculate the
weight percentile and categorized into four groups: (i) below the 3rd
percentile, (ii) 3rd to 15th percentile, (iii) 15th to 50th percentile and
(iv) 50th-85th percentile. In children with lower weight percentiles

based on the IAP Growth Chart, the impact of ChilRun full™
supplementation was assessed by evaluating changes in both weight
percentiles and weight-for-age Z-scores over a 90-day period. The
analysis of weight-for-age Z-scores and weight percentile distribution
from day 0 to day 90 revealed a positive trend in weight gain among
both male and female participants, reflecting improved nutritional
status and growth outcomes.
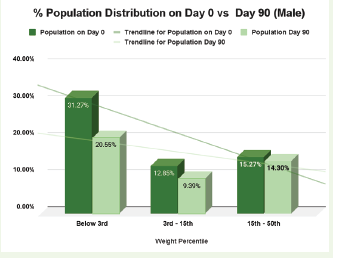
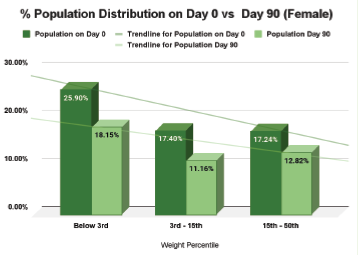
Among children aged 2–3 years, the proportion of those in the
below 3rd percentile category decreased from 31.27% to 20.55% in
males and from 25.90% to 18.15% in females, with corresponding
Z-score improvements from -0.39 to 0.01 in females and -1.84 to
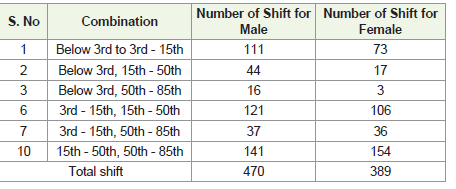
-0.94 in males. This shift was accompanied by 111 females and 73
female participants moving to the 3rd-15th percentile, 44 males and
17 females progressing to the 15th-50th percentile and 16 males
and 3 females reaching the 50th-85th percentile, demonstrating a
significant weight gain and improved nutritional recovery [Figure 9]
[Figure 10,11,12], [Table 5,6]. For children aged 4–6 years, those in the 3rd-15th percentile category showed a notable reduction, from
12.85% to 9.39% in males and 17.40% to 11.16% in females, alongside
Z-score increases from -2.70 to -1.85 in females and -2.24 to -1.50
in males. Within this group, 121 males and 106 females moved to
the 15th-50th percentile, while 37 males and 36 females moved to the
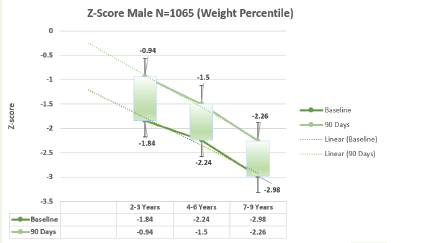
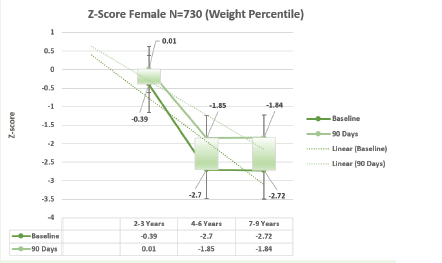
50th-85th percentile, further reinforcing the trend of weight gain and
percentile improvement [Figure 9,10,11,12] [Table 5,6]. A similar pattern was observed in children aged 7–9 years, where those in the
15th-50th percentile category experienced an upward shift, with the
proportion decreasing from 15.27% to 14.30% in males and 17.24% to
12.82% in females, as Z-scores improved from -2.72 to -1.84 (males)
and -2.98 to -2.26 (females). A total of 141 males and 154 females
from this percentile group successfully progressed to the 50th-85th
percentile, indicating an overall positive shift in weight status
[Figure 9,10,11,12] [Table 5,6] .
These findings demonstrate the effectiveness of nutritional
supplementation in promoting weight gain across all age groups,
as evidenced by increased Z-scores and upward shifts in weight
percentiles. The maximum improvements were observed in
younger children, suggesting that early intervention plays a crucial
role in addressing growth deficits and supporting healthier weight
trajectories.
Discussion
Optimal nutrition during early childhood provides a strong
foundation for lifelong health, cognitive development and
socioeconomic productivity. ChilRun full™ offers a comprehensive
nutritional intervention designed specifically for children above 2
years of age, addressing critical nutritional needs of growing kids.
Early childhood represents a critical period during which
nutritional deficiencies can lead to irreversible developmental
consequences [15]. Adequate nutrition supports physical
growth, cognitive development, immune function and metabolic
programming, with effects extending into adulthood [16]. Nutritional
deficiencies during this growth period impair neurogenesis,
synaptogenesis and myelination, resulting in suboptimal cognitive
outcomes and reduced school performance [17]. Furthermore,
malnutrition disrupts normal endocrine function, affecting growth
hormone secretion, Insulin-like growth factor (IGF-1) activity
and thyroid hormone metabolism [18]. The relationship between
nutrition and immune function creates a bidirectional cycle, where
malnutrition increases infection susceptibility, which further
exacerbates nutritional deficiencies. This scenario significantly led
to childhood morbidity in resource-limited settings, with long-term
consequences on growth, development and economic productivity.
Nutritional intervention during early childhood, therefore,
represents a high-impact strategy for improving health trajectories
and developmental outcomes [20].
Globally, approximately 149 million children under five experience
stunting and 45 million suffer from wasting, with disproportionate
burden in South Asia and Sub-Saharan Africa (UNICEF-WHOWorld
Bank, 2020) [3]. Despite progress in reducing malnutrition
over recent decades, significant disparities persist between regions
and within countries. Malnutrition affects approximately 25% of
children globally, with stunting and wasting impacting physical
development, cognitive function and immune competence [15,16].
In India, malnutrition represents a critical public health challenge,
with the highest child wasting rate globally at 18.7% according to the
Global Hunger Index 2024 (UNICEF-WHO-World Bank, 2020).
This alarming statistic places India at the 105th position among 124
countries, behind neighboring nations including Sri Lanka (56th),
Bangladesh (84st) and Nepal (68th). The National Family Health
Survey-5 (2019-21) reports 35.5% of children under five as stunted and
19.3% as wasted, with significant state-level variation in prevalence
(ICMR-NIN, 2020) [23]. To effectively address malnutrition in
India, a multi-faceted approach is needed, focusing on education,
healthcare, agriculture and community empowerment. The
Government of India, through various schemes like PoshanAbhiyaan
and the Integrated Child Development Services (ICDS), is actively
addressing malnutrition in India. These initiatives focus on improving
nutritional content, delivery and outreach, particularly targeting
vulnerable groups like children, pregnant women and lactating
mothers. Oral Nutritional Supplements (ONS) are a crucial tool in
addressing malnutrition in India, particularly for vulnerable groups
like children and pregnant women. By supplementing their usual diet
with a complete blend of macronutrients and micronutrients, ONS
can improve growth, nutrient intake and reduce the frequency of
illness in nutritionally at-risk children.
In this PAN India study (at 282 clinics across 32 cities across India),
we studied the effect of ChilRun full™, an oral nutritional supplement
on anthropometric parameters (including height, weight and BMI)
in children (2851 children aged 2 years and above over a 90-day
period). ChilRun full™ 2+ provides 37 essential nutrients specifically
formulated to support critical developmental processes in children
above two years. This ONS is a balanced profile of macronutrients
(carbohydrates, proteins and fats) and micronutrients (vitamins and
minerals: including Vitamin K2, zinc and iron), complemented by
functional ingredients including fructooligosaccharides (FOS) as
prebiotic, L. Acidophillus as probiotic [10]. As per earlier study by
Jain et al; 2024, ChilRun full™ plays a significant role in supporting
the growth and development of growing children and contributed to
significant upward trend in height, weight and BMI across the various
age groups of children of Eastern regions of India and contributed in
optimalgrowth, transforming into healthy, energetic and strong kids.
The present post marketing surveillance (PMS) study findings
reveal significant and linear improvements in anthropometric
parameters—height, weight and BMI—across all age groups, with
particularly remarkable outcomes in children at risk of malnutrition
(Z-scores ≤ -1) (Figure 4) (Figure 6). In this study, ChilRun full™ also
exhibited a significant improvement in Z-scores for weight, height
and BMI across all the age groups [Figure 7]. In children aged 2-3
years the Z-score for height, weight and BMI improved from -0.17,
-0.18 and -0.01 at baseline to -0.03, 0.08 and 0.19 on day 90. Similarly,
the improvement in the Z-scores was noted in children aged 4-6 years
(for height, weight and BMI from -0.66, -0.35 and 0.34 at baseline
to -0.53, -0.16 and 0.86) and 7-9 years (for height, weight and BMI
from -0.89, -0.60 and -0.09 at baseline to -0.75, -0.40 and 0.22) on day
90. The upward trends suggest that ChilRun full™ has the potential
to support the optimal growth patterns in children of all age groups.
In subset analysis of special population was conducted for
(a) Z-score analysis for weight, height and BMI in children at
risk of malnutrition (Z-scores ≤ -1): it was clearly observed that
those children at risk of malnutrition and initiated ChilRun full™, a
comprehensive total nutritional supplement addressed their severe
nutritional deficits and promoted catch-up growth during critical
periods of development. Z-score in all age group children increased
from -1.88 to - 1.69 for height, -1.75 to -1.35 for weight and -1.40 to -
1.20 for BMI [Figure 8]. This change in Z-score for height, weight and
BMI was 10.30%, 20.56% and 14.59%, respectively. It indicates timely
intervention of nutritional supplements is essential in malnourished
children. (b) Gender wise Z-score distribution based on weight
percentile profile: The analysis of weight-for-age Z-scores and weight
percentile distribution from day 0 to day 90 revealed a positive trend
in weight gain among both male and female participants, reflecting
improved nutritional status and growth outcomes, defines its
potential role of ChilRun full™ in growth and development in both
genders. Further, on continuous use for 90 days ChilRun full™ was
well tolerated as no adverse events were reported in any age group
from any one of the clinics.
According to ICMR-NIN data, malnutrition-related disability adjusted
life years (DALYs) demonstrate a 6.8-fold difference between
lowest and highest socio-demographic index states, accounting for
68.2% of total under-five deaths nationally (ICMR-NIN, 2020). These
statistics highlight the critical importance of nutritional interventions
in addressing India’s child health challenges. The ICMR-NIN
Dietary Guidelines for Indians (2020) emphasize the importance of
dietary diversity, micronutrient adequacy and appropriate feeding
practices for addressing childhood malnutrition, with specific
recommendations for different age groups and physiological states
(ICMR-NIN, 2020) [23]. Based on this study data, ChilRun full™ is
a potential nutritional intervention for growing kids to combat not
only India Child health challenges but also for specific populations
who are associated with micronutrient deficiency due to pick/fussy
eating behaviours.
Considering this, supplementing with macronutrients,
micronutrients and functional ingredients are crucial for the optimal
child growth and development of kids, especially in situations where
a balanced diet is not readily available or when specific nutrient
needs are not met. Supplementation can help prevent deficiencies,
optimize growth and enhance overall health making the kid healthy,
energetic and strong. Macronutrients (fat, protein, carbohydrates)
deliver energy substrates necessary for growth while supporting
tissue synthesis and repair. Adequate protein intake is essential for
building and repairing tissues, supporting growth and providing
energy. Carbohydrates, which are the primary source of energy for the
body and brain, support physical activity and brain function. While
healthy fats are essential for brain development, hormone balance,
cell membrane integrity and fat-soluble vitamin absorption [24].
In this study we have also explored that child aged 2–3 years (in
subset analysis) who are on continuous supplementation of ChilRun
full™ for 90 days, the growth parameters in terms of percentile
category, the proportion of those in the below 3rd percentile category
decreased from 31.27% to 20.55% in males and from 25.90% to
18.15% in females, with corresponding Z-score improvements from
-0.39 to 0.01 in males and -1.84 to -0.94 in females. This shift was
accompanied by 111 male and 73 female participants moving to the
3rd-15th percentile, 44 males and 17 females progressing to the 15th-
50th percentile and 16 males and 3 females reaching the 50th-85th
percentile, demonstrating a significant weight gain and improved
nutritional recovery.
These findings demonstrate the effectiveness of nutritional
supplementation in promoting weight gain across all age groups,
as evidenced by increased Z-scores and upward shifts in weight
percentiles. The maximum improvements were observed in younger
children (2-3 years), suggesting that early intervention plays a crucial
role in addressing growth deficits and supporting healthier weight
trajectories.
The micronutrients iron, zinc, calcium, vitamin A, vitamin D
and B-complex vitamins, addresses the common deficiencies seen in
children [25]. Iron supports hemoglobin synthesis, oxygen transport
and cognitive development, with iron deficiency anemia affecting
58.1% of Indian children under five years (ICMR-NIN, 2020),
zinc facilitates immune function, protein synthesis and wound
healing, with specific requirements outlined in ICMR-NIN
guidelines, supporting linear growth and neurodevelopment [1].
Vitamins play a vital role in numerous bodily functions, including
immunity, energy production and bone health. The inclusion of
specialized functional nutrients such as choline (essential for brain
development), taurine (supporting neurological development),
L-carnitine (facilitating energy metabolism), L-arginine (promoting
growth hormone secretion and support bone health) and inositol
(involved in cell signaling) enhances the formulation’s capacity to
support comprehensive development. These components target
specific physiological processes critical during periods of rapid
growth and development during early childhood [25,26,27]. Various
micronutrients in ChilRun full™ influence childhood growth through
multiple physiological mechanisms, including modulation of
endocrine pathways, participation in redox reactions and facilitation
of hormone synthesis. Zinc influences testosterone metabolism
through inhibition of aromatase and 5α-reductase enzymes, affecting
androgenic signaling pathways essential for growth, while selenium
supports thyroid hormone synthesis and metabolism [28,29].
Vitamin D participates in steroidogenesis and influences sex
hormone synthesis through prostaglandin involvement, while
modulating calcium homeostasis through parathyroid hormone
regulation, directly impacting bone mineralization Iron, magnesium
and zinc contribute to IGF-1 metabolism, influencing IGF-1
synthesis, bioavailability and receptor signaling, thereby modulating
somatic growth and cellular proliferation [29]. The antioxidant
properties of vitamins C, E and selenium participate in cellular redox
regulation, protecting against oxidative stress that could impair
cellular function and prote inflammation. This antioxidant capacity
protects developing tissues, particularly the brain, from oxidative
damage while supporting immune function and cellular longevity
[30].
Micronutrients function as enzymatic cofactors in metabolic
pathways essential for energy production, macromolecule synthesis
and cellular proliferation. B-complex vitamins serve as cofactors
in carbohydrate, protein and lipid metabolism, while magnesium
activates over 300 enzymatic reactions including those involved
in DNA synthesis. These metabolic functions provide the overall
energetic and synthetic foundations necessary for tissue growth during
childhood and regular supplementation of these micronutrients in
growing children transform society as healthy, energetic and strong
kids. [31]
Further, ChilRun full™ also contains digestive nutrients, i.e.
fructooligosaccharides (FOS) & Lactobacillus acidophilus [10], which
support beneficial gut microbiota and facilitate production of short chain
fatty acids (SCFAs) including acetate, propionate, butyrate and
valerate that demonstrates anti-inflammatory properties. Further
SCFAs also interact with G-protein coupled receptors expressed in
multiple tissues, affecting energy homeostasis, insulin sensitivity
and appetite regulation [33]. SCFAs additionally modulate immune
function through regulation of regulatory T-cell development and
cytokine production, supporting balanced immune responses while
reducing growth-inhibiting inflammation [34].These SCFAs enhance
intestinal barrier function through promotion of tight junction
protein expression and mucin production, reducing translocation
of pathogenic organisms while facilitating nutrient absorption.
[32]. In addition, it is also known that the gut microbiome and
central nervous system function through the “gut-brain axis,”
suggesting another mechanism through which prebiotics support
neurodevelopment. Metabolites produced by gut microbiota
influence neural development, myelination and neurotransmitter
metabolism, contributing to cognitive and behavioral development.
[35]
Based on this observational study data, it is evident that
continuous use of ChilRun full™ not only provide significant and
linear improvements in anthropometric parameters—height, weight
and BMI across all age groups, but also provide remarkable outcomes
in children at risk of malnutrition (Z-scores ≤ -1). These findings
highlight the critical role of targeted nutritional interventions in
supporting optimal growth and development. The results further
suggest that ChilRun full™ may play a pivotal role in public health
strategies aimed at combating malnutrition and growth deficits.
Future studies could explore and evaluate broader developmental
outcomes such as cognitive and immune function, reinforcing the
comprehensive impact of nutritional supplementation in childhood
development.
Conclusion
ChilRun full™ offers a comprehensive nutritional supplementation
approach supporting multiple physiological mechanisms
through its balanced nutrient profile and functional ingredients.
The supplement’s components influence endocrine pathways,
redox balance, hormone synthesis and gut microbiome function,
collectively supporting physical growth, cognitive development and
immune function. As global and national efforts continue to address
childhood malnutrition, comprehensive nutritional supplements like
ChilRun full™ represent valuable nutritional products for growing
kids and develop them as healthy, energetic and strong kids.
Acknowledgement
We are thankful to all the following site investigators, who have
participated in this study and extended their significant time in
subject recruitment and data collection.
West Bengal / Odisha / Assam: Dr. Abhishek Ghosh, Dr. Abhirup Das, Dr. Achintya Kumar, Dr. Aditya, Dr. Ajay Kumar Mohanty, Dr. Akash Bhutra, Dr. Alok, Dr. Alok Satyaprakash Nayar, Dr. Amita Sinha Mondal, Dr. Amit Adhikary, Dr. Anindya Bandyopadhyay, Dr. Ankit Agarwal, Dr. Arindam Butt, Dr. Aritra Batabayal, Dr. Arpan Saha, Dr. Arunansu Beras, Dr. Arup Ratan Halder, Dr. Ashique Iqbal Alam, Dr. Ashish Saha, Dr. Ashok Priyadarshini, Dr. Ashutosh Kumar, Dr. Azara Sultana, Dr. B. K. Mohanthy, Dr. Baikuntha Nath Kayshap, Dr. BasanthaRaut, Dr. Bhibudatta Mishra, Dr. Bichitrananada, Dr. Bikash Sarkar, Dr. Biswajit Ghosh, Dr. C K Tiwari, Dr. D K Shetty, Dr. Debadeep Cha, Dr. Debanjan Saha, Dr. Debashish Sahu, Dr. Deepak Kumar Behera, Dr. Dibyendu Chakrobathy, Dr. Dilip Kumar Das, Dr. G. Medhi, Dr. Gautam Kumar Maity, Dr. Gopal Kumar Khemka, Dr. Goutam Kumar Sahoo, Dr. Hariprasad Mohanty, Dr. Himanshu, Dr. Himanshu Palai, Dr. Hirumoni Saikla, Dr. Janaki Ballav Pradhan, Dr. Jaydeep Chakrobathy, Dr. Jyotiranjan, Dr. Jyotiranjan Sathapathy, Dr. K. P. Behera, Dr. Kishore Chandra, Dr. Mukesh Jain, Dr. Mujibur Rahman, Dr. N. P. Modi, Dr. Nihant Dash, Dr. Nirmal Kumar Jain, Dr. Palash Das, Dr. Pankaj Kr Nath, Dr. Piyush Shukla, Dr. Pranab Kr Pati, Dr. Pranabesh Ghosh, Dr. Pratap Kumar Behera, Dr. Pratik Dey, Dr. Probin Prakash Pahi, Dr. R. K. Singh, Dr. Rabi Kumar, Dr. Rafiqul Hasan, Dr. Raj Kr Paul, Dr. Rajib Kumar Roy, Dr. Rakibuddin Ahmed, Dr. Ranjeet Kumar Agarwal, Dr. Rashmi Pattnaik, Dr. Rashna Das Hazarika, Dr. Ravi Kant, Dr. Rishi Kant Bajaj, Dr. S K Bhattacharya, Dr. S. K. Paul, Dr. Sabyasachi Bhatacharya, Dr. Sanchita Roy, Dr. Sarthak Naik, Dr. Satish Sethy, Dr. Sayan Chaterjee, Dr. Sayantan Banerjee, Dr. Sebaranjan Biswal, Dr. Seema Rungta, Dr. Shakti Pad Das, Dr. Siddharta Sankar Kuanr, Dr. Subhakanta Patel, Dr. Subhankar Samel, Dr. Sudip K. Maity, Dr. Sujan Mitra, Dr. Sumeet Kumar Balali, Dr. Sumit Bishayi, Dr. Sunil Agarwal, Dr. Sushrut Das, Dr. Swarna Khaur, Dr. Swarupa Panda, Dr. Swastika Pal, Dr. Tapas Karmarkar, Dr. Vikram Samal, Dr. Virendra Katoch, Dr. Vivek Maheshwari. North India: Dr. A. Dixit, Dr. A. K. Agarwal, Dr. A. K. Rastogi, Dr. Abhineet Srivastav, Dr. Abhishek Goel, Dr. Abhishek Singh Rauthan, Dr. Ajit Sahay, Dr. Amit Verma, Dr. Anitab Kumar, Dr. Anuj Srivastav, Dr. Anup Kumar, Dr. Arvind Kumar, Dr. Ashok Bhuwalka, Dr. Ashwani Gupta, Dr. Awadh Agarwal, Dr. Badiyanath Das, Dr. Bharati Jha, Dr. D S Kumawat, Dr. Deepak Kumar Gupta, Dr. Dilip Kumar Jha, Dr. Dvendra Singhal, Dr. Gagan, Dr. Gurpreet Singh, Dr. H. Agnihotri, Dr. H. P. Bhainsala, Dr. Hash Vaish, Dr. Jatin Garg, Dr. Jitender Kumar, Dr. K. K. Jindal, Dr. Kushagra Gupta, Dr. Lalit Gulati, Dr. M K Shukla, Dr. M. S. Thomar, Dr. Madhu Sinha, Dr. Madhur Gupta, Dr. Manit Sakhuja, Dr. Mohd M. Khan, Dr. Mohit Aggarwal, Dr. MohitGhai, Dr. Naresh Mongia, Dr. Naveen Rana, Dr. Neelu Arora, Dr. Nikhil Melhotra, Dr. Ninesh Kumar, Dr. O. N. Srivastav, Dr. O. P. Mahansaria, Dr. P. C. Gupta, Dr. P. S. Narang, Dr. Pallavi Kumar, Dr. Pankaj Garg, Dr. Pankaj Maria, Dr. Parmanand Singh, Dr. PrabhasRanjan, Dr. Pradeep Singh, Dr. Pradeep Tandon, Dr. Prem R. Kumar, Dr. Pritosh Shrivastav, Dr. Rakesh Kumar, Dr. Rajan Pandey, Dr. Rajeev Arora, Dr. Rajeev Garg, Dr. Rajesh Kumar, Dr. Rajesh Patel, Dr. Rajiva Kumar, Dr. Rajnish Chandra, Dr. Raju Dixit, Dr. Raman Ghai, Dr. RamaniRanjan, Dr. Ranjeet Kumar, Dr. Reena Sinha, Dr. Ritesh Kamat, Dr. Rahul Garg, Dr. S. C. Gupta, Dr. S. K. Agarwal, Dr. S. K. Trivedi, Dr. S. P. Mishra, Dr. Sajeev Kumar Jha, Dr. Sanjay Prasad, Dr. Sanjay Singla, Dr. Satyajeet Kumar, Dr. Sekhar Biswas, Dr. SekharVashisht, Dr. Setu Kumar, Dr. Shalini Gandhi, Dr. Shamullah, Dr. Shanu Prabhakar, Dr. Shashank R. Ojha, Dr. Shilpi Jain, Dr. Shrey Rastogi, Dr. ShyamBabu Gupta, Dr. Subhash Chandra, Dr. Sunil Kumar Singh Mothari, Dr. Supriya Rastogi, Dr. Suresh Bali, Dr. Syed Zeya Karim, Dr. Tarun Anand, Dr. Vineet Sehgal, Dr. Vineet Tyagi, Dr. Vipin Jain, Dr. Yogita Arora, Dr. Zaheer Iqbal
Maharashtra and South India: Dr. Abhijit Agrawal, Dr. Adari Murali, Dr. Aijaz Ahmed, Dr. Amarnadha Reddy, Dr. AmolSonje, Dr. Angam Hari Kishore, Dr. Anuja Pethe, Dr. Archana Anil Kumar, Dr. Ashwin Reddy Katapally, Dr. AvinashWalawalkar, Dr. Awais Mirza, Dr. Basantha Kumar, Dr. Baswaraj Tandur, Dr. Bharat Parmar, Dr. C Vijaya Sainadh, Dr. Chakra Pani, Dr. Cyril J. D’Souza, Dr. D M Sneha Reddy, Dr. Dayanand Sagar, Dr. Donthamsetty Manoj, Dr. Eashwar Yerranguta, Dr. Faizan Bhoira, Dr. G Sai Ram, Dr. Gangissetty Vishal, Dr. Gaurav Sharma, Dr. Gentila Hari Krishna, Dr. Guruprasad, Dr. Hiren N Doshi, Dr. I. Paul Robinson, Dr. Iftekhar, Dr. J Kumar Raja, Dr. Jayalakshmi Sadanand Shetty, Dr. Jitendra Rajput, Dr. K Pawan Kumar, Dr. Kannam Durgesh, Dr. Khalid Saifur Rahman Khan, Dr. Kiran Kumar Pelle, Dr. Konda Shravan Kumar, Dr. Mahesh Sancheti, Dr. Manchala Sundeep Kumar, Dr. Manoj Kumar Gulabrao, Dr. Manoj Nalge, Dr. Mazhar Ali, Dr. Mhetre Amitraj Shivraj, Dr. Mithun Ghosh, Dr. N. Venkata Krishna, Dr. Nafees Ahmed, Dr. Nagesh Sali, Dr. Nandanapalli Nanda Kishore, Dr. Nikhil Bhandari, Dr. P Sureshkumar, Dr. Palavi Taritha, Dr. Parmeshwar Chandawade, Dr. Prabhakar Rao, Dr. Prasanna Pramod Kulkarni, Dr. R Venugopal, Dr. RajagiriHarika, Dr. Rajesh Subhramanyam, Dr. Raju Samudrala, Dr. Rao Narayanan Babu, Dr. Rashmi J. Begani, Dr. Raviteja Ch., Dr. Ritesh Kumar Singh, Dr. Rohit Kamble, Dr. Rupesh Mendedkar, Dr. S Sabari Raja, Dr. S. Raju Md, Dr. Sailesh Gupta, Dr. Sajid Musani, Dr. Sanath Shetty, Dr. Santosh Kumar, Dr. Satish Kulkarni, Dr. Simhachalan, Dr. Sita Rama Vara Prasad Chebrolu, Dr. Sultan Amarender, Dr. Suraj Doshi, Dr. Suraj Upadhya, Dr. Suresh Nighot, Dr. Sushant Vila, Dr. Swapnil Janbandhu, Dr. T Shilpa Reddy, Dr. Thadure Krishnachaitanya, Dr. Umesh Choudhari, Dr. Unmesh Phadnis, Dr. V Veera Ratnakar, Dr. Vatsal Surti, Dr. Veladi Kalyan, Dr. Vikas Sharma, Dr. Vinodkumar Hotkar, Dr. Y Sunil Kumar, Dr. Yogesh Tank.
West Bengal / Odisha / Assam: Dr. Abhishek Ghosh, Dr. Abhirup Das, Dr. Achintya Kumar, Dr. Aditya, Dr. Ajay Kumar Mohanty, Dr. Akash Bhutra, Dr. Alok, Dr. Alok Satyaprakash Nayar, Dr. Amita Sinha Mondal, Dr. Amit Adhikary, Dr. Anindya Bandyopadhyay, Dr. Ankit Agarwal, Dr. Arindam Butt, Dr. Aritra Batabayal, Dr. Arpan Saha, Dr. Arunansu Beras, Dr. Arup Ratan Halder, Dr. Ashique Iqbal Alam, Dr. Ashish Saha, Dr. Ashok Priyadarshini, Dr. Ashutosh Kumar, Dr. Azara Sultana, Dr. B. K. Mohanthy, Dr. Baikuntha Nath Kayshap, Dr. BasanthaRaut, Dr. Bhibudatta Mishra, Dr. Bichitrananada, Dr. Bikash Sarkar, Dr. Biswajit Ghosh, Dr. C K Tiwari, Dr. D K Shetty, Dr. Debadeep Cha, Dr. Debanjan Saha, Dr. Debashish Sahu, Dr. Deepak Kumar Behera, Dr. Dibyendu Chakrobathy, Dr. Dilip Kumar Das, Dr. G. Medhi, Dr. Gautam Kumar Maity, Dr. Gopal Kumar Khemka, Dr. Goutam Kumar Sahoo, Dr. Hariprasad Mohanty, Dr. Himanshu, Dr. Himanshu Palai, Dr. Hirumoni Saikla, Dr. Janaki Ballav Pradhan, Dr. Jaydeep Chakrobathy, Dr. Jyotiranjan, Dr. Jyotiranjan Sathapathy, Dr. K. P. Behera, Dr. Kishore Chandra, Dr. Mukesh Jain, Dr. Mujibur Rahman, Dr. N. P. Modi, Dr. Nihant Dash, Dr. Nirmal Kumar Jain, Dr. Palash Das, Dr. Pankaj Kr Nath, Dr. Piyush Shukla, Dr. Pranab Kr Pati, Dr. Pranabesh Ghosh, Dr. Pratap Kumar Behera, Dr. Pratik Dey, Dr. Probin Prakash Pahi, Dr. R. K. Singh, Dr. Rabi Kumar, Dr. Rafiqul Hasan, Dr. Raj Kr Paul, Dr. Rajib Kumar Roy, Dr. Rakibuddin Ahmed, Dr. Ranjeet Kumar Agarwal, Dr. Rashmi Pattnaik, Dr. Rashna Das Hazarika, Dr. Ravi Kant, Dr. Rishi Kant Bajaj, Dr. S K Bhattacharya, Dr. S. K. Paul, Dr. Sabyasachi Bhatacharya, Dr. Sanchita Roy, Dr. Sarthak Naik, Dr. Satish Sethy, Dr. Sayan Chaterjee, Dr. Sayantan Banerjee, Dr. Sebaranjan Biswal, Dr. Seema Rungta, Dr. Shakti Pad Das, Dr. Siddharta Sankar Kuanr, Dr. Subhakanta Patel, Dr. Subhankar Samel, Dr. Sudip K. Maity, Dr. Sujan Mitra, Dr. Sumeet Kumar Balali, Dr. Sumit Bishayi, Dr. Sunil Agarwal, Dr. Sushrut Das, Dr. Swarna Khaur, Dr. Swarupa Panda, Dr. Swastika Pal, Dr. Tapas Karmarkar, Dr. Vikram Samal, Dr. Virendra Katoch, Dr. Vivek Maheshwari. North India: Dr. A. Dixit, Dr. A. K. Agarwal, Dr. A. K. Rastogi, Dr. Abhineet Srivastav, Dr. Abhishek Goel, Dr. Abhishek Singh Rauthan, Dr. Ajit Sahay, Dr. Amit Verma, Dr. Anitab Kumar, Dr. Anuj Srivastav, Dr. Anup Kumar, Dr. Arvind Kumar, Dr. Ashok Bhuwalka, Dr. Ashwani Gupta, Dr. Awadh Agarwal, Dr. Badiyanath Das, Dr. Bharati Jha, Dr. D S Kumawat, Dr. Deepak Kumar Gupta, Dr. Dilip Kumar Jha, Dr. Dvendra Singhal, Dr. Gagan, Dr. Gurpreet Singh, Dr. H. Agnihotri, Dr. H. P. Bhainsala, Dr. Hash Vaish, Dr. Jatin Garg, Dr. Jitender Kumar, Dr. K. K. Jindal, Dr. Kushagra Gupta, Dr. Lalit Gulati, Dr. M K Shukla, Dr. M. S. Thomar, Dr. Madhu Sinha, Dr. Madhur Gupta, Dr. Manit Sakhuja, Dr. Mohd M. Khan, Dr. Mohit Aggarwal, Dr. MohitGhai, Dr. Naresh Mongia, Dr. Naveen Rana, Dr. Neelu Arora, Dr. Nikhil Melhotra, Dr. Ninesh Kumar, Dr. O. N. Srivastav, Dr. O. P. Mahansaria, Dr. P. C. Gupta, Dr. P. S. Narang, Dr. Pallavi Kumar, Dr. Pankaj Garg, Dr. Pankaj Maria, Dr. Parmanand Singh, Dr. PrabhasRanjan, Dr. Pradeep Singh, Dr. Pradeep Tandon, Dr. Prem R. Kumar, Dr. Pritosh Shrivastav, Dr. Rakesh Kumar, Dr. Rajan Pandey, Dr. Rajeev Arora, Dr. Rajeev Garg, Dr. Rajesh Kumar, Dr. Rajesh Patel, Dr. Rajiva Kumar, Dr. Rajnish Chandra, Dr. Raju Dixit, Dr. Raman Ghai, Dr. RamaniRanjan, Dr. Ranjeet Kumar, Dr. Reena Sinha, Dr. Ritesh Kamat, Dr. Rahul Garg, Dr. S. C. Gupta, Dr. S. K. Agarwal, Dr. S. K. Trivedi, Dr. S. P. Mishra, Dr. Sajeev Kumar Jha, Dr. Sanjay Prasad, Dr. Sanjay Singla, Dr. Satyajeet Kumar, Dr. Sekhar Biswas, Dr. SekharVashisht, Dr. Setu Kumar, Dr. Shalini Gandhi, Dr. Shamullah, Dr. Shanu Prabhakar, Dr. Shashank R. Ojha, Dr. Shilpi Jain, Dr. Shrey Rastogi, Dr. ShyamBabu Gupta, Dr. Subhash Chandra, Dr. Sunil Kumar Singh Mothari, Dr. Supriya Rastogi, Dr. Suresh Bali, Dr. Syed Zeya Karim, Dr. Tarun Anand, Dr. Vineet Sehgal, Dr. Vineet Tyagi, Dr. Vipin Jain, Dr. Yogita Arora, Dr. Zaheer Iqbal
Maharashtra and South India: Dr. Abhijit Agrawal, Dr. Adari Murali, Dr. Aijaz Ahmed, Dr. Amarnadha Reddy, Dr. AmolSonje, Dr. Angam Hari Kishore, Dr. Anuja Pethe, Dr. Archana Anil Kumar, Dr. Ashwin Reddy Katapally, Dr. AvinashWalawalkar, Dr. Awais Mirza, Dr. Basantha Kumar, Dr. Baswaraj Tandur, Dr. Bharat Parmar, Dr. C Vijaya Sainadh, Dr. Chakra Pani, Dr. Cyril J. D’Souza, Dr. D M Sneha Reddy, Dr. Dayanand Sagar, Dr. Donthamsetty Manoj, Dr. Eashwar Yerranguta, Dr. Faizan Bhoira, Dr. G Sai Ram, Dr. Gangissetty Vishal, Dr. Gaurav Sharma, Dr. Gentila Hari Krishna, Dr. Guruprasad, Dr. Hiren N Doshi, Dr. I. Paul Robinson, Dr. Iftekhar, Dr. J Kumar Raja, Dr. Jayalakshmi Sadanand Shetty, Dr. Jitendra Rajput, Dr. K Pawan Kumar, Dr. Kannam Durgesh, Dr. Khalid Saifur Rahman Khan, Dr. Kiran Kumar Pelle, Dr. Konda Shravan Kumar, Dr. Mahesh Sancheti, Dr. Manchala Sundeep Kumar, Dr. Manoj Kumar Gulabrao, Dr. Manoj Nalge, Dr. Mazhar Ali, Dr. Mhetre Amitraj Shivraj, Dr. Mithun Ghosh, Dr. N. Venkata Krishna, Dr. Nafees Ahmed, Dr. Nagesh Sali, Dr. Nandanapalli Nanda Kishore, Dr. Nikhil Bhandari, Dr. P Sureshkumar, Dr. Palavi Taritha, Dr. Parmeshwar Chandawade, Dr. Prabhakar Rao, Dr. Prasanna Pramod Kulkarni, Dr. R Venugopal, Dr. RajagiriHarika, Dr. Rajesh Subhramanyam, Dr. Raju Samudrala, Dr. Rao Narayanan Babu, Dr. Rashmi J. Begani, Dr. Raviteja Ch., Dr. Ritesh Kumar Singh, Dr. Rohit Kamble, Dr. Rupesh Mendedkar, Dr. S Sabari Raja, Dr. S. Raju Md, Dr. Sailesh Gupta, Dr. Sajid Musani, Dr. Sanath Shetty, Dr. Santosh Kumar, Dr. Satish Kulkarni, Dr. Simhachalan, Dr. Sita Rama Vara Prasad Chebrolu, Dr. Sultan Amarender, Dr. Suraj Doshi, Dr. Suraj Upadhya, Dr. Suresh Nighot, Dr. Sushant Vila, Dr. Swapnil Janbandhu, Dr. T Shilpa Reddy, Dr. Thadure Krishnachaitanya, Dr. Umesh Choudhari, Dr. Unmesh Phadnis, Dr. V Veera Ratnakar, Dr. Vatsal Surti, Dr. Veladi Kalyan, Dr. Vikas Sharma, Dr. Vinodkumar Hotkar, Dr. Y Sunil Kumar, Dr. Yogesh Tank.
References
Citation
Jain Naveen K, Dheeraj K, Amera K, Patil Chandrashekhar S. A Nationwide Multicentric, in-Clinic, Observational Study on ChilRun full™: Real-World Effectiveness Data on Growth and Development in Indian Children. Indian J Nutri. 2025;12(1): 314.