Case Report
Pure Uterine Lipoma-A Review of Two Cases
Bhanji A1 and Neelakantan A2*
1Consultant Histopathologist, Plus Care Internationals Private Limited, Sewri, Mumbai, Maharashtra, India.
2Consultant Histopathologist & Laboratory Director, Plus Care Internationals Private Limited, Sewri, Mumbai, Maharashtra, India.
2Consultant Histopathologist & Laboratory Director, Plus Care Internationals Private Limited, Sewri, Mumbai, Maharashtra, India.
*Corresponding author:Amrita Neelakantan, Consultant Histopathologist & Laboratory Director, Plus Care Internationals Private Limited, Sewri, Mumbai-400015 Maharashtra, India. E-mail Id: amritaneel@yahoo.co.in
Article Information: Submission: 04/03/2024; Accepted: 17/04/2024; Published: 22/04/2024
Copyright:© 2024 Bhanji A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Lipomatous uterine tumours are not commonly encountered, and pure uterine lipomas are a rare entity, as compared to their mixed counterpart lipoleiomyomas, with a low incidence of reported cases. [1] Their reported incidence is 0.03-0.2%. [2] Most reported cases have been of mixed type, consisting of admixture with smooth muscle or fibrous tissue. [3] Clinical diagnosis is rarely made, and the diagnosis is usually confirmed on pathological examination.
We report two cases, one of a 68-year-oldand one of a 55-year-old, both postmenopausal females, who presented with a bulky uterus diagnosed as fibroid uterus on ultrasonography. Upon hysterectomy, the specimens were sent for histopathological examination which revealed well circumscribed lesions in the myometrium composed of sheets and lobules of mature adipose tissue, with thin fibrous septae. The endometrium lining was pushed to the periphery. A diagnosis of uterine lipoma/lipomatosis was made.
The histogenesis of pure uterine lipomas are debatable, and a possible theory involves fatty metaplasia of smooth muscle cells of the myometrium. Awareness about this entity is important, as an accurate diagnosis can reduce the need for hysterectomy in these patients, owing to the benign nature of these lesions, and conservative management can be done.
We report two cases, one of a 68-year-oldand one of a 55-year-old, both postmenopausal females, who presented with a bulky uterus diagnosed as fibroid uterus on ultrasonography. Upon hysterectomy, the specimens were sent for histopathological examination which revealed well circumscribed lesions in the myometrium composed of sheets and lobules of mature adipose tissue, with thin fibrous septae. The endometrium lining was pushed to the periphery. A diagnosis of uterine lipoma/lipomatosis was made.
The histogenesis of pure uterine lipomas are debatable, and a possible theory involves fatty metaplasia of smooth muscle cells of the myometrium. Awareness about this entity is important, as an accurate diagnosis can reduce the need for hysterectomy in these patients, owing to the benign nature of these lesions, and conservative management can be done.
Keywords:Uterine Lipoma; Benign; Lipomatosis; Lipoleiomyoma
Introduction
Lipomatous tumours of the uterus are rare, benign neoplasms,
with a low incidence rate varying from 0.3 to 0.12% [4]. These tumours
are commonly encountered in postmenopausal women from 50 to 70
years of age, and they may be associated with uterine fibroids. [4]
The clinical or macroscopic presentation may mimic a soft tissues
arcoma, leading to a diagnostic dilemma. They may mimicuterine
leiomyoma, except for their occurrence in postmenopausal women
[5]. Uterine lipomas are generally uterine and intramural in location
[6]. Most are asymptomatic; however, some present with vaginal
bleeding, lower abdominal distension and pain. [7]
Lipomatous tumours are usually classified into pure and mixed
types [7], with mixed types being more commonly encountered. The
histogenetic theories of these uncommon lesions are still debatable,
and a possible theory involves fatty metaplasia of smooth muscle cells
of the myometrium. [7]
We report two cases of uterine lipomas, both in post-menopausal
women, presenting with dysfunctional uterine bleeding.
Case Report
Case 1:
A 68-year-old post-menopausal woman presented with
dysfunctional uterine bleeding and pain; No history of previous
malignancies orhormonal therapy. Ultrasonography showed a large
uterine mass with endometrial thickness of 4 mm. Adnexa were
normal. The patient underwent total abdominal hysterectomy.Pathological findings:
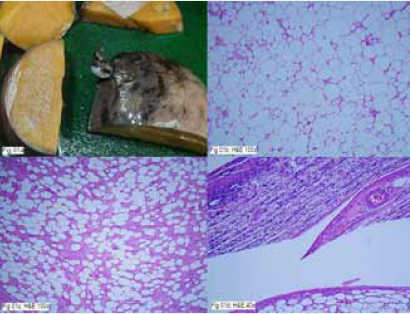
Gross examination revealed a bosselated uterus measuring 15 x 11
x 11 cm. Uterine cavity was distorted due to a large intramural mass
measuring 10 cm in diameter. Cut section was yellow, homogenous,
greasy (Figure1a). Another intramural mass was measuring 5 x 4 x 4
cm; cut section was yellow white.Microscopically larger tumour was composed of mature
adipocytes arranged in lobules separated by thin fibrovascular septae
and surrounded by myometrium (Figure 01b; H, E 100x). There was
no nuclear atypia, increase in mitosis or necrosis. Lipoblasts were
not seen. The other tumour showed mature adipocytes arranged in
lobules with varying proportion of intermixed fascicles and bundles
of smooth muscle fibres (Figure 01c; H, E 100x). Endometrium
showed senile cystic atrophy (Figure 01d; H, E 40x). A diagnosis of
pure uterine lipoma and lipoleiomyoma was proposed.
Immunohistochemistry (IHC) revealed S-100 positive adipocytes
in the larger tumour while SMA and Desmin positive for rim of
myometrium.The smaller tumour showed SMA positive smooth
muscle cells. This confirmed the diagnosis of a pure lipoma and a
lipoleiomyoma.
Case 2:
A 55-year-old post-menopausal woman presented with pain in
lower abdomen. On sonography a large uterine fibroid was noted,
with unremarkable endometrium and adnexa. Total abdominal
hysterectomy was done.Pathological findings:
Grossly uterus was bosselated, measuring 12 x 11 x 8 cm with
two intramural masses measuring 4 x 3 x 3 cm and 3 x 3 x 2 cm. Cut
section of the larger mass was yellow, homogenous, greasy (Figure
02a). Smaller mass was separately received, cut section being greywhite,
whorled.Microscopically larger mass was well circumscribed encapsulated
composed of mature adipocytes arranged in lobules separated by
thin fibrovascular septae surrounded by rim of myometrium (Figure
02b; H, E100x) (Figure 02c; H, E 100x). There was no nuclear atypia,
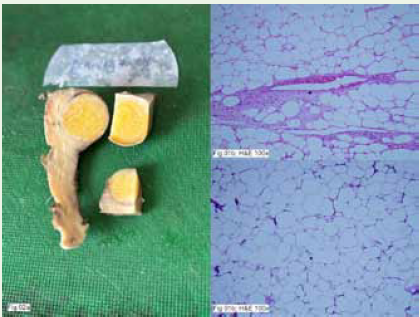
increase in mitosis or necrosis. Lipoblasts were not seen. The smaller
mass showed leiomyoma. A diagnosis of pure uterine lipoma and
leiomyoma were proposed.
Immunohistochemistry (IHC) on the larger mass revealed
adipocytes positive for S-100 while the surrounding smooth muscle
cells were positive for SMA and Desmin. The smaller mass showed
positivity for SMA and Desmin.
This confirmed the diagnosis of a pure lipoma co-existent with a
leiomyoma.
Discussion
Lipomas are the most common soft tissue tumours in the body;
however, lipomas of the uterus are rare, with a low reported incidence
of 0.03-0.2%. [2]. Uterine lipomas fall under the umbrella of uterine
fatty tumours (UFT) [10] which are a range of benign tumours
that may be composed entirely of adipocytes or may be intermixed
with connective tissue or smooth muscle. Due to the range of
histopathological possibilities based on the proportion of fat, smooth
muscle and fibrous tissues, UFTs encompass a spectrum that includes
pure lipomas, lipoleiomyomas and fibrolipomas [10],as smooth
muscle cells and fibroblasts are admixed with mature adipocytes
within the mass [1,4]. The exact incidence rate of these tumours is
unknown, as being benign causes them to be frequently undiagnosed
[4].
According to Willen R et al., a pure lipoma should be diagnosed
only if smooth muscle cells are present at the periphery [2].They
usually occur in asymptomatic, perimenopausal or postmenopausal
women and may be associated with leiomyomas, whose clinical
history could be indistinguishable [4,5,8].
Preoperative diagnosis of uterine lipomas is generally challenging
[6]. On ultrasound and CT, one may confuse with a fatty degeneration
of a leiomyoma or ovarian tumour, if the size is very large, and an
MRI provides more specific, but not always accurate, findings with
lipomas.
In our cases, only ultrasound was done which diagnosed both
cases as fibroid uteri. This reinforces the value of histopathology in
diagnosing pure lipomas of the uterus.
The coexistence of both pure uterine lipomas and uterine
lipoleiomyomas has rarely been reported in literature. [4] To our
knowledge, only two cases have been recently reported in literature
[4]. In one of these, the authors presented a case of association of
a pure uterine lipoma, a leiomyoma and endometrial cancer as a
tumour triplicity, which may have contributed to the pathogenesis of
mesenchymal tumours in this location [11].
The histogenesis of these tumours is still debated. As fat tissue
is not native to the uterus, various theories of histogenesis have been
proposed. These include misplaced embryonic fat cells, metaplasia
of the muscle or connective tissue cells into the fat cells, adipocytic
differentiation of primitive connective tissue cells, proliferation of
perivascular fat cells accompanying the blood vessels into the uterus,
inclusion of the fat cells into the uterine wall during surgery or fatty
infiltration or degeneration of the connective tissue. [6]
Some researchers have emphasized that a hyperestrogenic state
in metabolic disorders such as hyperlipidaemia, hypothyroidism,
diabetes mellitus, postmenopausal lipid metabolism changes and
toxaemia during pregnancy may contribute to its development. [9]
Fatty metaplasia of the connective tissue or the smooth muscle
cells seems to be the most plausible histogenetic theory involved in
the development of uterine lipomas [4].
Since leiomyomas and lipoleiomyomas were coexistent with
the uterine lipoma in our cases, we may hypothesise that fatty
metamorphosis of smooth muscle cells of leiomyomas favours the
development of the uterine lipoma.
In our cases, the histopathological examination revealed that the
tumour consisted exclusively of mature adipose tissue, peripherally
delimited by smooth muscle cells, which rule out the diagnosis of a
mixed lipoma and suggest a pure lipoma. We carefully analysed the
tumour, ensuring the absence of lipoblasts, nuclear atypia and brisk
or atypical mitosis. With this we concluded the diagnosis as pure
lipoma, excluding possibility of a liposarcoma or other malignancies.
Follow-up of our patient revealed no medical complaints till date.
In conclusion, pure uterine lipoma is very rare benign uterine
tumour which presents with clinical signs like that of leiomyoma,
and may be missed on radiological examination or confused with
leiomyomas. Treatment of the tumour is hysterectomy, if the patient
has excessive pain or vaginal bleeding. Our report throws light upon
this rare entity, its co-existence with lipoleiomyomas and leiomyomas,
and aims to increase awareness about its existence to avoid a delay in
the diagnosis and the accompanying morbidity, and if suspected preoperatively
in asymptomatic patients, to avoid major surgery in older
patients. It also makes the reader aware that such tumours could be
an incidental finding on hysterectomy specimens.
References
Citation
Bhanji A, Neelakantan A. Pure Uterine Lipoma-A Review of Two Cases. Indian J Gynecol. 2024;1(1): 107.