Case Report
Unraveling the Enigmatous Path of a Nulliparous Intraoperative Case of Adnexal Torsion
Anitha K* and Susmitha G
Department of Obstetrics and Gynecology, Yashoda Hospitals, Hitec city, Hyderabad, Telangana, India
*Corresponding author: Anitha K, Department of Obstetrics and Gynecology, Yashoda Hospitals, Hitec city, Hyderabad,Telangana, India. E-mail: Anithak11422@gmail.com
Article Information: Submission: 12/09/2023; Accepted: 04/10/2023; Published: 09/10/2023
Copyright: © 2023 Anitha K, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Adnexal torsion is a rare and rare occurrence, particularly in non-gravid anomalous uterus. Preoperative diagnosis is difficult, and the condition is diagnosed during surgical exploration. Delay in diagnosis can be lethal, as the uterus and adnexa can undergo irreversible gangrenous changes. Timely surgical intervention is crucial for managing such cases. This case involves a 27-year-old nulliparous lady with an anomalous uterus who presented with acute abdominal pain.
Keywords: Adnexal Torsion; Anomalous Uterus; Nulliparous; Ovarian Torsion
Introduction
Torsion of adnexal structures is a rare surgical emergency,
affecting women of any age group, particularly reproductive age
[1]. It often causes sudden abdominal pain and increases the risk of
ovarian twisting due to an ovarian mass larger than 5 cm [2,3].
The right ovary is more likely to undergo torsion due to its longer
utero-ovarian ligament compared to the left. The sigmoid colon
on the left may help prevent torsion [4]. Delay in diagnosis and
correction can lead to adverse effects like hemorrhage, ischemia, loss
of ovarian function, necrosis, abscess, or peritonitis. Ultrasound with
Doppler flow is the primary imaging modality. [5] Laparoscopy is the
ideal procedure for diagnosis and treatment of adnexal torsion, and
conservative surgery is preferred over removal. A rare presentation of
an anomalous non-gravid uterus with adnexal torsion has not been
reported in literature.
Case Report
A 27-year-old nulliparous woman presented with sudden,
colicky lower abdominal pain for 30 minutes, radiating to the back
and accompanied by four episodes of vomiting. She had a regular
menstrual history and had a left iliac fossa tenderness, and no
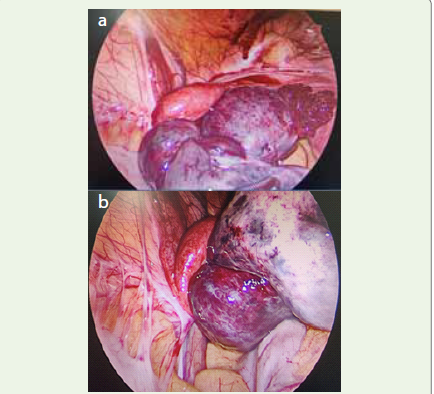
guarding. A USG scan showed a grossly enlarged left ovary with
multiple hemorrhagic follicles and no vascularity. The [Figure 1a,1b]
left ovary measured 50cc and had left ovarian torsion.

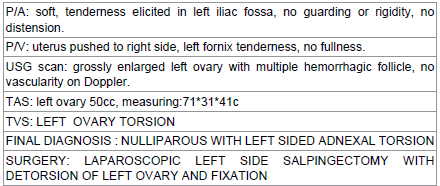
The final diagnosis was nulliparous with adnexal torsion was
followed by left ovarian torsion surgery, involving laparoscopic left
salpingectomy with detorsion of the left ovary and fixation. [Figure 2a-d Table1].
Discussion
This is a rare presentation of an anomalous non-gravid uterus
with adnexal torsion which has not been reported in literature yet.
Since being unique, this case cannot be compared with other cases
of gravid or adnexal torsions. Adnexal torsion, a 3-5% emergency
case, primarily affects reproductive-age women and involves rotation
of adnexal structures, causing ischemic changes and affecting the
reproductive system. [6,7] Ovarian torsion is most common in women
aged 20-30, with 70% occurring on the right side due to longer
uteroovarian ligament and limited space from the sigmoid colon.
[6]
Adnexal torsion is a significant risk in females with acute
abdominal pain. Early diagnosis and intervention are crucial
to prevent complications like hemorrhage, ischemia, abscess,
peritonitis, and organ function loss [6]. A minimally invasive surgical
approach with detorsion and preservation of adnexal structures is
recommended. Surgeons should not remove a torsed ovary unless
oophorectomy is unavoidable, such as when a severely necrotic ovary
falls apart. This case is significant due to its rarity and the need for
conservative fertility preserving surgery. A young nulliparous woman
sought to preserve her fertility, and prompt intervention prevented
serious consequences. Oophorectomy was not the final treatment,
but oophoropexy was performed to prevent recurrence risk. Rody
et al. recommend conservative management of ovarian torsion,
regardless of macroscopic appearance, as no severe complications
occur. Animal studies show reperfusion of ischaemic ovaries after 24
hours improves ovarian viability [Figure 3]
[8].
Pathogenesis:
Ovarian torsion occurs when an ovarian cyst rotates in fundibulo
pelvic and UO ligaments, affecting normal ovaries and premenarchal
girls with elongated ligaments. The occurrence may decrease postpuberty
due to ligament shortening. [9] A 10-year review found 2.7%
of emergency surgery cases involved ovarian torsion, with 2%-15%
of surgically treated adnexal masses causing torsion. Most ovarian
torsion occurs in reproductive age groups, with less common in
premenarchal girls and postmenopausal women.Risk Factors:
[10] Over 80% of ovarian torsion patients have 5 cm or larger
ovarian masses, with a correlation between mass size and torsion risk.
Large cysts in ovarian induction may increase the risk of torsion.
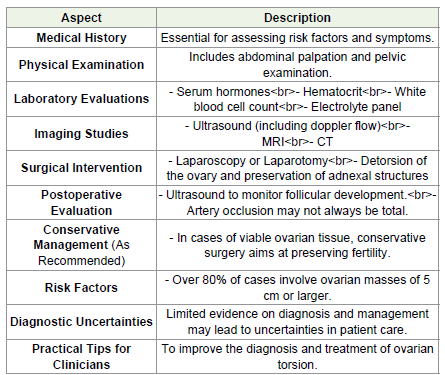
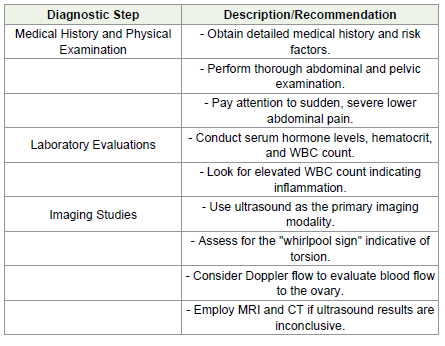
A medical history and physical examination are essential for
diagnosing ovarian torsion. Laboratory evaluations include serum
hormones, hematocrit, white blood cell count, and electrolyte panel.
Imaging studies, such as ultrasound, doppler flow, MRI, and CT, are
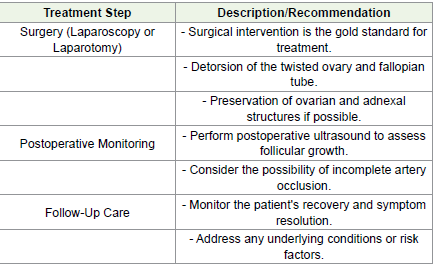
crucial for evaluating pelvic masses. Surgery, including laparoscopy
and laparotomy, is the gold standard for treating ovarian torsion.
Postoperative ultrasound shows normal follicular development,
and animal studies suggest that artery occlusion may not be total in
We purpose a table for Diagnostic and Management Aspects of
Ovarian Torsion [Table 2].As per our experience, here are the diagnostic and treatment guidelines for ovarian torsion in table format [Table 3,4].
Please note that these are general guidelines, and individual cases may vary. Prompt diagnosis and intervention are crucial to prevent complications associated with ovarian torsion.
Limited evidence on ovarian torsion diagnosis and management raises uncertainties in patient care. This article provides practical tips for clinicians.
Conclusion
Strong clinical suspicion is the key factor to diagnose adnexal
torsion and for timely intervention which could prevent morbidity.
Ultrasound with Doppler helps in diagnosing adnexal mass with
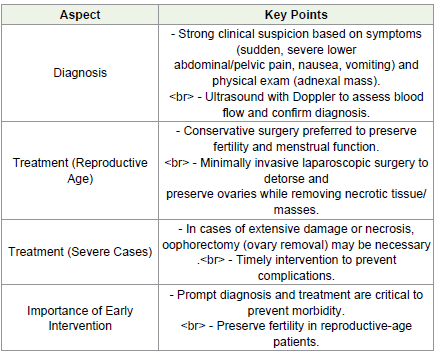
torsion. Conservative surgery is the preferred mode of treatment
for patients in the reproductive age group to preserve the menstrual
function.
Summary:
Adnexal torsion diagnosis is challenging, surgical likelihood
depends on clinical suspicion, laparoscopy is preferred, and
detorsion is safe. The case highlights the difficulty in accurate adnexal
torsion diagnosis, urging management as a surgical emergency and
considering early laparoscopy/laparotomy for fertility.References
Citation
Anitha K, Susmitha G. Unraveling the Enigmatous Path of a Nulliparous Intraoperative Case of Adnexal Torsion. Indian J Gynecol. 2023;3(1): 106.