Review Article
Efficacy of Soybean in Menopausal Syndrome (Literature Review)
Velhal A1* Kirti B2
1Department of Swasthavritta and Yoga S.G.R, Ayurved College, India
2Bharati Vidyapeeth College of Ayurved, Deemed to be University, Pune, India
*Corresponding author: Velhal A, Department of Swasthavritta and Yoga S.G.R. Ayurved College, Solapur, India, Tel:
9175403402 / 9271207790; Email:velhalamol@gmail.com
Article Information: Submission: 19/05/2021; Accepted: 18/06/2021; Published: 21/06/2021
Copyright: © 2021 Velhal A. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Menopause is the critical time period in the life of a woman when menstruation ceases. It is also known as the climacteric. There isa decrease in hormone
estrogen production by the ovariesand is commonly associated with symptoms such as fatigue, hot flashes, joint pain, mood fluctuations,sweating and vaginal
dryness. Approximately one third of the Indian womenexperience menopausal symptoms. Alternative methods to deal with these menopausal symptoms
are lifestyle changes, use of Yoga and meditation, use of hormone replacement therapy, and phytoestrogen-rich foods such as soybeans. Some Studies
reveal that phytoestrogen supplementation offers a possible alternative to conventional hormonal replacement therapy (HRT). Among available food Soybean
exhibits the highest concentration of isoflavones. Regular consumption of soybeans had been evidenced to have diminished menopausal symptoms. Due to
safety profile and benefit to overall female health soybean is preferred food.
Keywords
Menopause; Phytoestrogen; Soybeans
Introduction
India has a large population, with 71 million people over 60
years of age and about 43 million menopausal women already above
one billionmarks. The expected population in India is projected to
be 1.4 billion in 2026.Out of which 173 million people will be over
60 years and 103 million menopausal women. In Indian women,
the median age of menopause is 47.5 years with an average life
expectancy of 71 years [1]. Also India, with a population of 1.2 billion
people, is the second largest emerging economy and second most
populated country in the world. According to the latest World Health
Organization (WHO) data published in 2018, the life expectancy in
India for a female is 70.3 years, expected to increase to 77 years by
2050. Non communicable diseases account for 60% of the total deaths
in India. Currently, approximately 10% of India’s population, i.e.,
more than 100 million, is aged over 50 years[2].
The estimated mean age of menopause is 46 years in India. This
early age of menopause predisposes a woman to chronic health
disorders. Breast cancer is the most common cancer in Indian women,
and the incidence peaks before the age of 50 years [3].
Although menopause is physiological process it leads to various
symptoms due to estrogen deficiency. This affects quality of life.
Soybean commonly available in India is one of the most nutritious
pulses feasible under cultivation. It has all macronutrients for better
nutrition, protein, fat, carbohydrates, calcium, iron, vitamin B1,
and phytoestrogens which are helpful to alleviate the menopausal
problems [4]. Also soybean is available in many forms. Soy products
of wide varieties have been prepared such as roasted soybean, boiled
soybean, soymilk, soy mayonnaise, miso, soy cheese, soy yogurt,
tempeh, soy sauce, tamari, Textured Vegetable Protein (TVP), or
Textured Soy Protein (TSP) and tofu [5]. This article isa review article
that has assessed the efficacy of soy beans in menopausal symptoms.
An overview of menopause:
Menopause is a natural biological and physiological process
that leads to the permanent cessation of menstrual cycle of a
woman’s reproductive life. It usually occurs around 40 to 50 years
of age. It is characterized by the cessation of menstrual periods for
twelve continuous months, hormonal disturbances,and menopausal
symptoms, which include hot flashes and night sweats along with vasomotor symptoms. During menopause various organs undergo
changes, e.g., the cortex of the ovaries becomes thinner and contains
fewer follicles and the vaginal layers become dry and thinner
and lose elasticity. Furthermore, evidence suggests that estrogen
deficiency leads to an increase in osteoclastic activity, which results
in an imbalance between osteoclastic and osteoblastic activities.
Moreover, estrogen deficiency leads to vasoconstriction in the wall
of arteries and an accelerated increase of low-density lipoproteins,
thereby increasing the risk of cardiovascular diseases, disturbed sleep
patterns, mood swings, vasomotor symptoms, and generally a lower
quality of life [6].The symptom complex can be divided into VMS, somatic
symptom, genitourinary syndrome of menopause (GSM), and
neuropsychiatric symptom. Vasomotor symptoms (VMS) such as hot
flushes and sweating, are very common in menopausal populations
and can cause physical and mental discomfort [7].There is deficiency in
the production of estrogen. This deficiency leads to various symptoms
such as hot flashes, night sweats, mood swings, lack of concentration,
loss of confidence, fatigue, dryness of vagina, sleep disturbances,
irritability etc. Throughout the menopause transition, estrogen
deficiency results in an increase in weight and fat accumulation. Also,
various organs undergo changes, e.g. the cortex of the ovaries becomes
thinner and contains fewer follicles and the vaginal layers become dry
and thinner and lose elasticity[8]. Furthermore, evidence suggests
that estrogen deficiency leads to an increase in osteoclastic activity,
which results in an imbalance between osteoclastic and osteoblastic
activities 6. Moreover, estrogen deficiency leads to vasoconstriction
in the wall of arteries and an accelerated increase of low-density
lipoproteins, thereby increasing the risk of cardiovascular diseases,
disturbed sleep patterns, mood swings, vasomotor symptoms, and
generally a lower quality of life [9]. In short, estrogen deficiency is
responsible for range of physiological and psychological changes
during menopause.
Management of Menopausal Symptoms:
Traditionally estrogen remains the most effective treatment for
all menopausal symptoms. Administration of estrogen is called as
Hormone Replacement Therapy (HRT).It is also called as menopausal
hormone therapy (MHT). MHT covers therapies including
estrogens, progestogen, combined therapies, androgens, and
tibolone. Various terminology used in MHT: ET-estrogen therapy:
EPT-estrogen progesterone therapy: AT-androgen therapy: SERMsselective
estrogen receptor modulators (raloxifene and bazedoxifene):
Gonadomimetics- tibolone, which contains estrogen, progestogen,
and androgen activity [10].But it causes breast pain or tenderness,
vomiting, loss of appetite, leg cramps and joint pain, weight gain or
loss, nervousness, depression and irritability. Non-hormonal drugs
or agents may relieve VMS but have their own side effects.Adverse effects of MHT:
In the WHI trial, prior randomized use of CEE plus MPA,
compared with placebo, among women who had an intact uterus,
was significantly associated with a higher breast cancer incidence but
no significant difference in breast cancer mortality [10]. MHT affects
glucose metabolism, both in women with and without type 2 diabetes mellitus. MHT is relatively contraindicated – in leiomyosarcoma,
EC type II, advanced metastatic malignant melanoma, lung cancer,
gastric cancer, and bladder cancer, breast cancer, endometrial
stromal sarcoma, uterine carcinosarcoma, ovarian cancer (estrogen
dependent granulosa cell, low grade serous, and Sertoli–Leydig,
endometroid types of ovarian tumors), adenocarcinoma of the
cervix meningioma, glioma, and hormone receptor positive gastric
and bladder cancer. If bleeding starts after commencement of
progesterone therapy in cyclical regimens or there is a change in
the duration or intensity of blood flow which is not normal for that
woman extensive investigations are required. The dose and duration
of use of MHT should be individualized after extensive follow up.
Risk–benefit assessment is carried out annually. Follow-up every
month may also be required.MHT is generally preferred to women below the age of 50
years or within 10 years of menopause. The risk of VTE (Venous
thromboembolism) is increased by oral MHT. There is an increased
risk of stroke with oral MHT. There is a dose dependent relationship
among the dose and duration of MHT with VTE. Risk of gallstones,
cholecystitis, and cholecystectomy is increased with oral estrogen
alone and combination MHT. If economy is considered menopause
management has significant direct and indirect costs. Direct
costs include gynecologist’s visits, specialist’s visit, traditional
pharmacotherapy or alternative, complementary medicine therapy.
Indirect costs include laboratory testing, management of adverse
events, loss of productivity at home and at workplace, treatment of
associated medical disorders.
Menopause is a critical window of opportunity for use of other
non-hormonal, traditional dietary regimen and adopting healthy life
style.
Soybean: A boon for menopause:
Due to the potential undesirable health consequences and many
adverse effects caused by hormonal therapies, numbers of women are
searching for herbal therapies or secondary metabolites from plants
as alternatives to treat typical menopausal symptoms. This trend has
been increasing since last decade.In recent years, nutraceuticals such as phytoestrogens and herbal
derivatives have gained popularity due to their claimed ability to
relieve menopausal symptoms. Nutraceuticals are defined as foods,
parts of foods, or botanicals that provide medical and health benefits,
such as the prevention and treatment of disease [11].
The word “phytoestrogen” comes from the Greek term for plant
(“phyto”) and from the term
“Estrogen”, that is a hormone that influences the female fertility
in vertebrates. Phytoestrogens are compounds found in plants.
Among the phytoestrogens, isoflavones and lignans are commonly
used to relieve menopausal symptoms, as they are abundant in fruits,
vegetables, legumes, and soy [12]. A study on soy intake in various
countries revealed that the average daily soy intake is nine times
higher in Asian countries compared to North American and European
countries, resulting in a higher life expectancy on average [13]. Among
the isoflavones used to treat menopause symptoms, genistein has been widely used because of its important properties and the fact that
it accounts for about 60% of the total isoflavones found in soy [14]. A
search for the terms “genistein” and “cancer” using PubMed revealed
that the main molecular targets of genistein are estrogen receptors,
protein tyrosine kinases, and topoisomerase II. So genistein can be
used in the treatment of typical postmenopausal symptoms, cancer,
obesity, osteoporosis, hormonal changes, gene activity alterations,
cardiovascular disease, atherosclerosis, and diabetes, and provide
a comprehensive overview of the underlying mechanisms and
therapeutic actions of genistein [15].
Isoflavone Classification:
Phytoestrogens are naturally occurring nonsteroidal phenolic
plant compounds and can be divided into two main groups: flavonoids
and non-flavonoids [16]. Flavonoids include isoflavones, coumestans
and prenylflavonoids, and non-flavonoids include lignans.Genistein, daidzein, glycitein, biochanin A, and formononetin
belong to isoflavone phytoestrogens. Equol, as a daidzein metabolite,
is sometimes also ranked among this group [16]. It is solely a metabolic
product of intestinal bacteria. Isoflavones are ranked among the
compounds having substantial amount of estrogen. The main source
of isoflavones is legumes from the family Fabaceae, namely soybean
(Glycine max) as a source of daidzein, genistein, and glycitein and
red clover (Trifolium pratense) as a source of formononetin and
biochanin A.
Absorption
Soy isoflavones (genistein, daidzein and glycitein) are present in
significant quantities (up to 4-5 mg g-1 on a dry basis) in legumes,
mainly soy, green beans, mung beans [17]. In cereals (raw materials)
they are generally present as glycosides, and are poorly absorbed.
The main metabolite of soy isoflavones is equol, produced through
digestion by the bacterial flora, and is thought to be the most
responsible for the isoflavone activity[18]. After soy intake, a biphasic
model is found in the absorption of soy isoflavones in plasma and
urine, which appears to be due to the absorption in the small intestine
(about 10%) during the first 2 hours after the intake and to that in the
large intestine (about 90%) 4-6 hours after taking. The bioavailability
of isoflavones is also influenced by intestinal bacteria and treatment
with oral antibiotics. While daidzain and genistein begin to be
absorbed a few minutes after intake, the equol appears in plasma only
at least 8 hours after taking soy, due to the required transit time of
daidzain to colon, where the conversion of daidzain to equol occurs
thanks to the intestinal microbiota [18].
Phytoestrogens, found in the diet as glucoconiugates (daidzin,
genistin), are hydrolysed in the intestine in the active aglycon forms
(daidzein and genistein) by the action of UDP-glucuronosyltransferase,
which is secreted by intestinal bacteria. Genistein and daidzein are
also produced by the demethylation of their precursors, respectively
biocanin A and formononetin. The aglycones are absorbed from the
intestinal tract towards the liver, where they are mainly conjugated
with glucuronic acid and sulfates. Some of the conjugated aglycones
are excreted in the bile, where they are hydrolysed, and some of
the unconjugated aglycones are excreted in the faeces, whereas
some of them are reabsorbed in the liver through the enterohepatic circulation. In the blood, isoflavones are metabolised mainly in equol
and O-desmethylangolensin, which are excreted in the urine[18]. In
short the major factor that presence of specific bacteria equipped with
the right β-glucosidase in the intestinal microbial flora regulates the
production of equol.
Estrogenic Activity of Isoflavones:
Vasomotor symptoms of menopause, including hot flashes,
night sweats, and insomnia (as a consequence), are the essential
symptoms of postmenopausal estrogen deficiency [19].Various
study showed that soy intake reduced the incidence of hot flashes as
compared to the beginning of the study.During clinical research, a
randomized double-blind study in menopausal women found that
the administration of 30 mg of genistein for 12 weeks reduced hot
flashes by 51% (9.4–4.7/day), whereas, the placebo group experienced
only a 27% reduction (9.9–7.1/day) [20].Studies have also pointed out that the ability of women to produce
equol may be the major determinant of whether or not isoflavones
can effectively reduce VMS. A systematic review and meta-analysis
of RCTs assessed the efficacy of soy isoflavones and equol for
alleviating menopausal symptoms (especially vasomotor symptoms)
in postmenopausal women who were either equol producers or
nonproducers [20]. The result of this meta-analysis revealed a
significant benefit of equol for decreasing hot flash scores. This
study concluded that supplementing equol to equol nonproducers
significantly lowered the incidence and/or severity of hot flashes in
menopausal women [21].
The mechanistic mode of action of Isoflavones is not yet
completely understood. The limitations of definitive conclusions
is due to the reason that studies have mostly been done through in
vitro assays using concentrations higher than those found under
physiological conditions. These isoflavones particularly equol is
found in plasma mainly as a 7-O-glucuronide derivative [22], which
makes it difficult to discern the biologically-active form(s) at tissue and
cellular levels. In spite of these deficits, evidence from experimental
studies suggests that equol may act in multiple ways [23]. Based on
its structural similarity to 17-beta -estradiol, equol binds to both
estrogen receptors (ERs) alpha (ER alpha) and beta (ER beta which
is the preferred target) with greater affinity. It is well-known fact ERs
are not equally distributed among the different tissues. So equol might
have different effects depending on the ratio of ER alpha and ER beta
isoforms present. Whether it acts as an agonist or an antagonist may
further depend on the level of endogenous estrogens present, as they
bind to both receptors more tightly [24]. The antioxidant activity of
equol seems to be mostly mediated by its interaction with the ER
beta, which induces the extracellular signal-regulated protein kinases
(ERK1/2) and the NF-kB peptide, factors that control transcription,
cytokine production, and cell survival [24]. Isoflavones and equol
may not act as antioxidants themselves but rather by triggering cell
signaling pathways leading to changes in the expression of cellular
enzymes such as superoxide dismutase, catalase, and glutathione
peroxidase (all involved in counteracting oxidative stress) [25].
These activities may provide the basis for therapeutic strategies, for
instance by restoring endothelial function in cardiovascular diseases.
An improvement in atherosclerosis has also been reported via equol attenuating ER stress, mediated by the activation of the NF-E2 p45-
related factor 2 (Nrf2) signaling pathway [26].
It can be hypothesized that genistein may act in cells via the
classical genomic mechanism, entering the cells by diffusing through
the lipid bilayer due to genistein being an effective ER modulator.
This complex moment stimulates the nucleus, mRNA synthesis, and
production of tissue-specific proteins [27]. These findings suggest
that genistein has the potential to ameliorate some emotional and
vasomotor symptoms. Further studies using genistein could help
to find a promising agent to treat typical symptoms associated with
menopause [27].
Combination of soybean and exercise:
Fontvieille et al. [28] verified the efficacy of phytoestrogen
supplementation (PHY: each capsule contained 325 mg of soy extract
with 17.5 mg of isoflavones for a 70-mg daily dose of 44 mg of daidzein,
16 mg of glycitein and 10 mg of genistein) combined with exercise
(EXT) on improving climacteric symptoms in postmenopausal
women, compared with EX plus placebo (PL). The 12-month exercise
program consisted of three non-consecutive sessions (1 h each) per
week of combined exercise, which means combination of aerobic
(30 min) and resistance (30 min) exercises. Climacteric symptoms
were assessed using the Kupperman Index questionnaire, including
11 symptoms: hot flushes, night sweats, insomnia, nervousness,
melancholy, dizziness, asthenia, arthralgia, headache, palpitation and
vaginal dryness. After 1 year of intervention, while the EX + PL group
showed improvements in the total score of menopausal symptoms and
hot flushes, the combination with phytoestrogens prevented positive
effects in the long term in overweight postmenopausal women. The
results of this study did not support the usefulness of phytoestrogen
supplementation in the long term when exercise is performed on a
regular basis and suggested that adding phytoestrogens may interfere
with exercise training adaptations as beneficial impacts were observed
in the EX + PL group only. Authors [28] suggested that exercise
(activating ERα) and phytoestrogens (activating ER β) may induce
opposite effects in the long term (Table 1).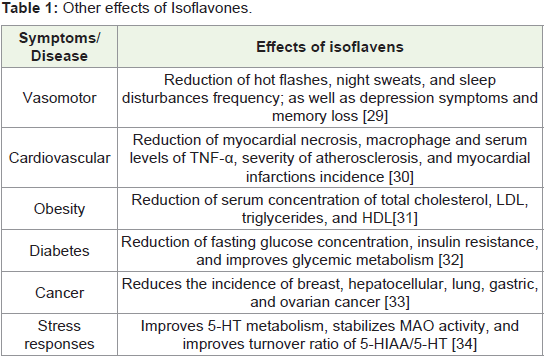
Abbreviations:
5-HIAA: 5-Hydroxyindoleacetic acid; 5-HT: serotonin; HDL:
high-density lipoprotein; LDL: low-density lipoprotein; MAO: monoamine oxidase; TNF-α tumor necrosis factor alpha. Information
is supported by references [29-34].Adverse effects of Isoflavones:
Isoflavones are generally well-tolerated by women. Some
gastrointestinal disturbances are found such as nausea, bloating,
diarrhea, and constipation. They are generally mild.Conclusions
Isoflavones are polyphenolic compounds usually represent most
common categories of phytoestrogens.They are structurally similar
to 17 beta estradiol and are found in the Fabaceae family. Before
metabolism, they are hydrolysed into aglycones by the microflora
present in the human digestive tract by the enzymes present in the
gastrointestinal tract.
Isoflavones reduce hot flashes, has good effect on attenuate
lumbar spine BMD loss, may show beneficial effects on systolic blood
pressure during early menopause, and may improve glycemic control
in vitro. Also benefits of isoflavones on urogenital symptoms were
observed.
A survey found that 70% of women would be “satisfied with a
non hormonal intervention that provided at least a 50% reduction in
hot flashes” [35]. As far as the safety profile of isoflavones combined
with exercise their makes them a compelling treatment option
for postmenopausal women unwilling or unable to use hormone
replacement therapy.
References
Citation
Velhal A, Kirti B. Efficacy of Soybean in Menopausal Syndrome (Literature Review). Indian J Gynecol. 2021;2(1): 104.