Case Report
Large Benign Brenner Tumour of Ovary: - an Incidental Findings Case Report
Anita Kant* and Amrita Razdan Kaul
Department of Obstetrics and Gynecology, India
*Corresponding author: Anita Kant, Department of Obstetrics and Gynecology, AIMS, Faridabad, India; E-mail: dranitakant@
gmail.com
Article Information: Submission: 05/10/2019; Accepted: 06/11/2019; Published: 08/11/2019
Copyright: © 2019 Kant A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Brenner tumour is a rare, mostly benign, unilateral solid ovarian tumour that is a part of the surface epithelial group of ovarian neoplasms. It is usually
asymptomatic an incidental pathological finding. Although most of the benign Brenner tumours are small but the case presented here had a large size of
tumour and was diagnosed radiologically as sub serous fibroid.
Introduction
Ovarian tumours area common form of neoplasia in female’s
accounting for about 30% of female genital cancers [1,2]. These
tumours behave in diverse ways however due to their anatomical
location they can remain asymptomatic for a long period till they
attain a large size to be detectable clinically. Brenner tumour of
ovary is a relatively uncommon neoplasm constituting 1.4 - 2.5% of
all ovarian tumours with predilection for postmenopausal age group
average of presentation being 50 yrs with 71% of female bring more
then > 40 yrs [1,3]. Brenner tumour is composed of transitional
epithelial cell nests similar to bladder epithelium. Brenner tumour
is mostly small, solid, firm, unilateral and benign. Bigger ones are
rare < 2% [2]. Radiological imaging modalities (USG and computed
tomography) are less sensitive for diagnosing it due to its non specific
appearance. Histopathology remains the gold standard for confirming
the diagnosis microscopically it is characterized by abundant dense
fibrous stroma with epithelial cell nests with grooving suggestive of coffee bean shaped nucleus.
Case Report
A 49 yrs old P10 L10 female presented in OPD of OBG
department of ASIAN HOSPITAL FARIDABAD with complaints of
polymenorrhagia, pain and lump in abdomen since few months. Her
vitals were stable. Systemic examination was suggestive of large 5 x 5
cm para umbilical hernia with a palpable firm to hard 18 weeks size
mass arising from pelvis, mobile, non tender on left side of abdomen. Per speculum examination was normal. Per vaginum examination
also suggested a large firm to hard 18 weeks mass towards the left side
of uterus, non tender, moving with cervical movements. Ultrasound
findings were suggestive of cholelithiasis with para-umbilical hernia
with large lobulated iso to hypoechoic mass in pelvis 10 x 8 cm
size suggestive of a sub serous fibroid. MRI Pelvis/lower abdomen
again suggested large well circumscribed exophytic sub serous
pedunculated leiomyoma arising from uterine fundus of 11.2 x 10.5
x 8.6 cm size with multiple sub centimeter intramural leiomyoma.
She wished to retain her reproductive/menstrual function.
So, Laparoscopy for planned myomectomy was started however
preoperatively the mass was found to be involving left side ovary,
hard in consistency approx. 10 x 10 cm in size. Uterus was parous in
size with normal right sided ovary and tubes.
Grossly there was a circumscribed, multilobulated, glistening
white mass with nodular surface. Left sided salpingo-oophorectomy
was done with peritoneal wash cytology. Tumour was removed in
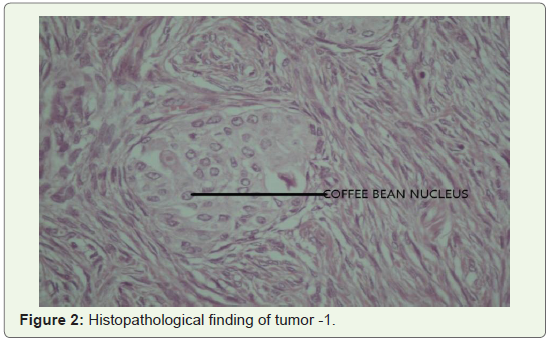
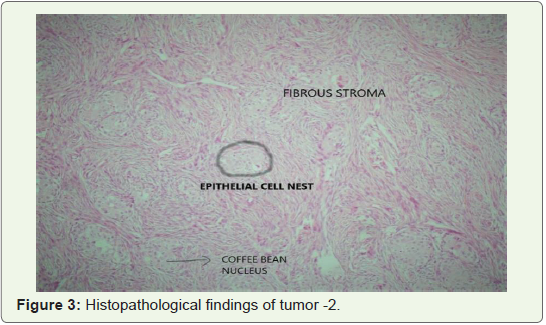
endobag by morcellation. Histopathological examination showed
well circumscribed epithelial cell nests with a surrounding abundant
fibromatous stroma. Epithelial cells were ovoid to polygonal with pale
cytoplasm and oval nuclei. Some of nuclei were found with central
longitudinal groove (coffee bean appearance) (Figures 1-3).
All feature suggesting benign Brenner tumour of ovary. Peritoneal
fluid cytology was negative for malignant cells. Post operatively
patient’s recovery remained uneventful.
Discussion
The ovarian lesions constitute a major burden in gynecology
practice due to the fact that these remain asymptomatic for a
longer period of time in view of their anatomical location. Among
symptomatic patients common symptoms include vaginal bleeding,
pelvic pain, pelvic mass, non specific gastric complaints of dyspepsia,
flatulence. Our patient presented with polymenorrhagia, pain and
lump abdomen. Brenner tumour is derived from pelvic mesothelium
or surface epithelium of ovary through transitional cell metaplasia to
form the typical urothelial like components [4]. It is mostly unilateral
with only 5-7% being bilateral. Histological pattern is typically benign
with only few reports of borderline or malignant counterparts [4,5].
Diagnosing Brenner tumour by radiological imaging modalities is difficult since the tumour has no specific appearance [6]. Brenner
tumour looks similar to other solid ovarian masses e.g, fibroma,
fibrothecoma, pedunculated leiomyoma in imaging techniques [7].
Grossly Brenner tumours are well circumscribed, hard with,
grey white or yellow cut surface. Borderline Brenner tumour
are characteristically cystic and unilocular or multi locular with
papillomatous masses protruding into one or more of locules.
Malignant Brenner tumour may be solid or cystic with mural nodules
without any descriptive features [8].
Microscopically Brenner tumour has abundant dense fibrous
stroma with epithelial nests of transitional cells. Fibrous component
is less prominent in borderline or malignant component. Complex
cystic tumours with varying amount of stroma often are in form of
papillary solid projections are common in borderline or malignant
histology pattern.
Most of the Brenner’s tumours are candidates for surgical
resection. Because of their vividly circumscribed nature these are
easily located and do not typically affect surrounding tissue. Surgical
resection is often curative and will reverse any symptoms of present.
Malignant Brenner tumours may affect surrounding tissues and
metastasis to other structures; however such incidents are so rare
that a standard treatment has not been developed. Even malignant
Brenner tumours if diagnosed early are usually candidates for
complete surgical resection.
Brenner tumour expresses several immunohistochemical markers
of urothelial differentiation including uroplakin-III, thrombo
modulator, p63, GATA-3, cytokeratin-7 helpful in diagnosis and
confirmation of Brenner tumour. However in view of high cost with
not much of clinical utility especially when histopathology confirmed
diagnosis of benign brenner tumor as in our case irrespective of size
of ovarian mass this was not recommended.
Conclusion
To conclude benign Brenner tumor although rare and usually
small ovarian tumor, can grow very large. Radiological imaging is
not of much help in diagnosing these tumors due to its non specific
features. Rather its solid consistency confuses it with other solid
uterine and ovarian tumors like thecoma, fibroma, leiomyoma.
Histopathology is hence mandatory and the gold standard for
diagnosing the Brenner tumour. Surgical removal is curative for these
tumours with reversal of all the symptoms. Hence clinician should be
aware of possibility of Brenner tumour while coming across a patient
with solid large pelvic mass.
References
Citation
Kant A, Amrita RK. Large Benign Brenner Tumour of Ovary: - an Incidental Findings Case Report. Indian J Gynecol. 2019;1(1): 101.