Case Report
Eosinophilic Annular Erythema Presenting as Chronic Polycyclic Plaques: A Clinicopathological Case Report
Shatanik Bhattacharya*
Department of Dermatology, Venereology and Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India
*Corresponding author:Dr. Shatanik Bhattacharya, Department of Dermatology, Venereology & Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India E-mail Id: shatanik.bhattacharya.97@gmail.com
Copyright: © 2026 Bhattacharya S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 12/03/2026; Accepted: 14/04/2026; Published: 16/04/2026
Abstract
Eosinophilic annular erythema (EAE) is a rare chronic figurate dermatosis characterized by recurrent annular plaques associated with tissue eosinophilia. Due to its clinical resemblance to granuloma annulare and other annular dermatoses, accurate diagnosis requires clinicopathological correlation. We report
a case of a 60-year-old postmenopausal woman who presented with multiple erythematous annular plaques over the forehead, trunk, upper limbs, and buttocks for two years. The lesions began as papules and gradually enlarged centrifugally with central clearing, eventually coalescing into polycyclic plaques.
Mild pruritus was present without systemic symptoms. Histopathological examination revealed an unremarkable epidermis with dense perivascular and interstitial inflammatory infiltrate composed predominantly of lymphocytes and eosinophils extending into the deep dermis and superficial fat. Flame figures were identified, while mucin deposition, collagen degeneration, and palisading granulomas were absent. The patient responded well to topical corticosteroids, systemic corticosteroids, and hydroxychloroquine. This case highlights the importance of recognizing EAE in the differential diagnosis of chronic annular dermatoses and underscores the role of histopathology in establishing the diagnosis.
Introduction
Figurate erythemas represent a heterogeneous group of
dermatological conditions characterized by annular, polycyclic,
or arciform lesions with centrifugal spread. Eosinophilic annular
erythema (EAE) is a rare entity within this group and is often
considered a chronic variant of Wells syndrome. Clinically, it closely
mimics granuloma annulare (GA) and other annular dermatoses,
making diagnosis challenging. Histopathological examination
remains crucial for differentiation.[1]
Case Report
A 60-year-old postmenopausal woman presented with a two-year
history of multiple circular erythematous lesions over the forehead,
trunk, upper limbs, abdomen, and buttocks. The lesions had an
insidious onset and gradually progressed in size and number. Initially
appearing as small papules, they enlarged centrifugally with relative
central clearing and eventually coalesced to form polycyclic plaques.
The lesions were mildly pruritic and painless.
There was no history of fever, weight loss, systemic symptoms, drug intake, insect bites, or preceding infection. The patient had no history of atopy, tuberculosis, hypertension, or diabetes. She had received multiple courses of oral itraconazole without improvement.
There was no history of fever, weight loss, systemic symptoms, drug intake, insect bites, or preceding infection. The patient had no history of atopy, tuberculosis, hypertension, or diabetes. She had received multiple courses of oral itraconazole without improvement.
On examination, multiple well-defined annular plaques ranging
from 2 cm to 15 cm in diameter were noted, predominantly over
the upper and mid-back with relative peripheral sparing [Figure 1-3]. Some lesions showed raised active borders with occasional


satellite papules. Scaling was absent. There was no lymphadenopathy,
hepatosplenomegaly, sensory deficit, or nerve thickening.
Peripheral blood examination did not reveal eosinophilia, with absolute eosinophil counts within normal limits.
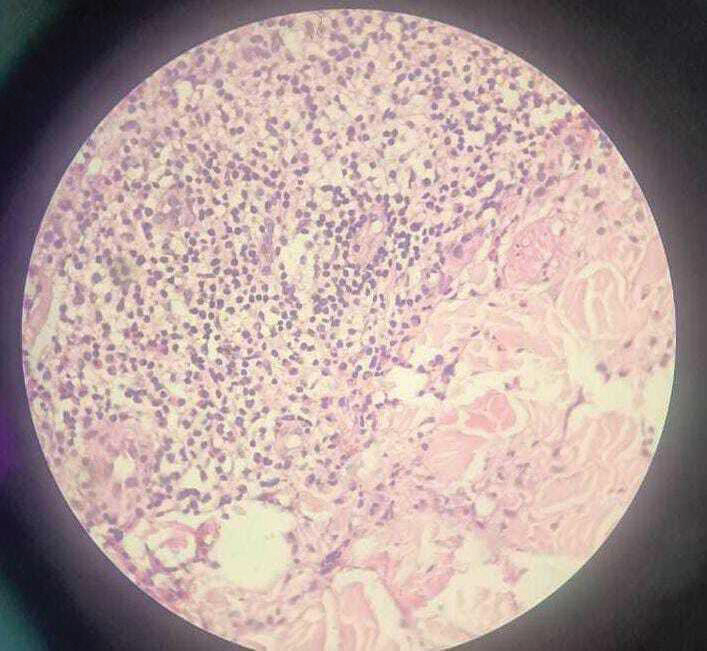
Histopathological examination [Figure 4-6] revealed an unremarkable epidermis. The dermis showed dense perivascular and interstitial inflammatory infiltrate composed predominantly of lymphocytes, eosinophils, and histiocytes extending into the deep dermis and superficial fat. Flame figures were present [Figure 5,6], characterized by deposition of eosinophilic granule proteins on
Peripheral blood examination did not reveal eosinophilia, with absolute eosinophil counts within normal limits.
Histopathological examination [Figure 4-6] revealed an unremarkable epidermis. The dermis showed dense perivascular and interstitial inflammatory infiltrate composed predominantly of lymphocytes, eosinophils, and histiocytes extending into the deep dermis and superficial fat. Flame figures were present [Figure 5,6], characterized by deposition of eosinophilic granule proteins on
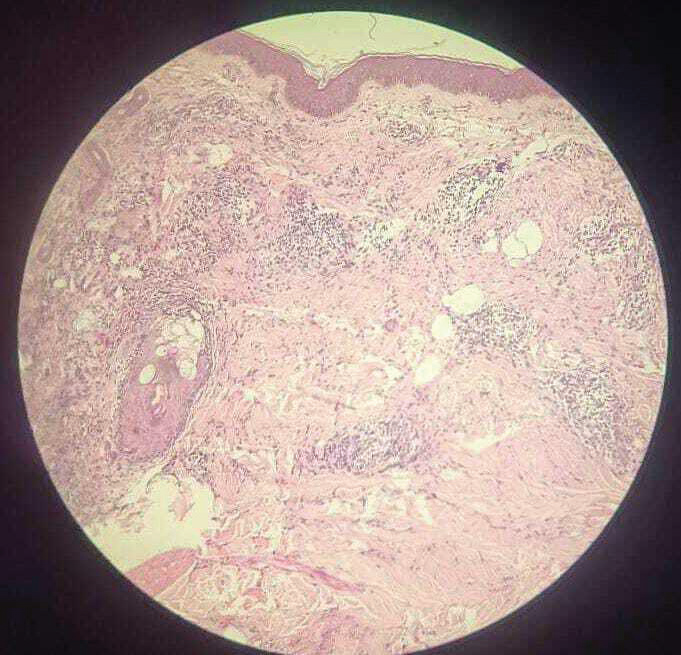
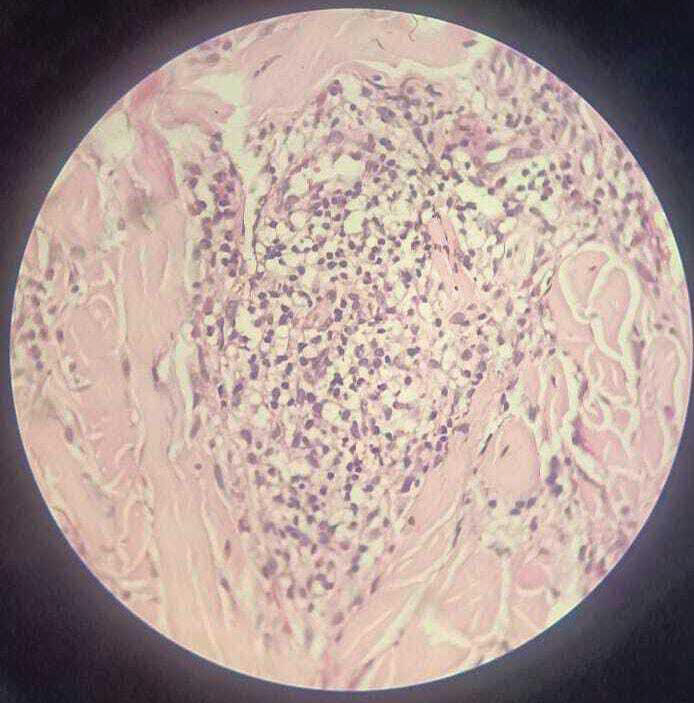
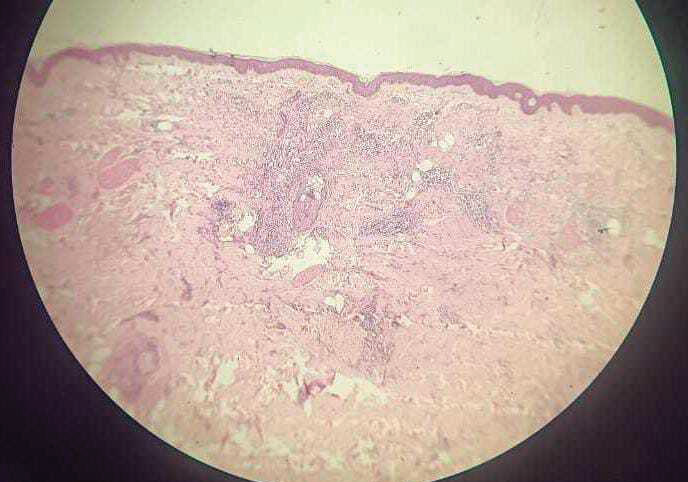
collagen bundles, appearing as intensely eosinophilic flame-shaped
structures representing eosinophil degranulation. There was no mucin
deposition, collagen degeneration, or palisading granulomatous
inflammation.
Based on clinicopathological findings, a diagnosis of eosinophilic annular erythema was made..
The patient was treated with topical betamethasone dipropionate 0.05% cream applied twice daily for three weeks. Systemic therapy included oral prednisolone 40 mg daily for two weeks, followed by gradual tapering from 30 mg to 7.5 mg. Hydroxychloroquine 200 mg twice daily was administered for three months after baseline ophthalmologic evaluation. Antihistamines were prescribed for symptomatic relief. Significant improvement was observed within three weeks.
Based on clinicopathological findings, a diagnosis of eosinophilic annular erythema was made..
The patient was treated with topical betamethasone dipropionate 0.05% cream applied twice daily for three weeks. Systemic therapy included oral prednisolone 40 mg daily for two weeks, followed by gradual tapering from 30 mg to 7.5 mg. Hydroxychloroquine 200 mg twice daily was administered for three months after baseline ophthalmologic evaluation. Antihistamines were prescribed for symptomatic relief. Significant improvement was observed within three weeks.
Discussion
Eosinophilic annular erythema is a rare chronic dermatosis
characterized by annular plaques with tissue eosinophilia. It is often
considered part of the Wells syndrome spectrum, although it differs
clinically by its chronic course and absence of acute inflammatory
features.[2]
Granuloma annulare is an important differential diagnosis due to its similar clinical presentation. However, histopathology differentiates the two conditions. GA typically shows palisading granulomas, mucin deposition, and collagen degeneration, whereas EAE demonstrates eosinophil-rich infiltrate with flame figures and lacks mucin and granulomatous architecture. [3,4]
Eosinophils may be present in GA in a subset of cases, but they are usually sparse and not associated with flame figures. The presence of prominent eosinophilic infiltrate and flame figures strongly favors EAE.[4]
The pathogenesis of EAE is not fully understood but is thought to involve a hypersensitivity reaction with eosinophilic activation. Various treatments have been described, including corticosteroids, antimalarials, dapsone, and immunomodulators. Our patient responded well to systemic corticosteroids and hydroxychloroquine, consistent with previous reports. [5-7]
Granuloma annulare is an important differential diagnosis due to its similar clinical presentation. However, histopathology differentiates the two conditions. GA typically shows palisading granulomas, mucin deposition, and collagen degeneration, whereas EAE demonstrates eosinophil-rich infiltrate with flame figures and lacks mucin and granulomatous architecture. [3,4]
Eosinophils may be present in GA in a subset of cases, but they are usually sparse and not associated with flame figures. The presence of prominent eosinophilic infiltrate and flame figures strongly favors EAE.[4]
The pathogenesis of EAE is not fully understood but is thought to involve a hypersensitivity reaction with eosinophilic activation. Various treatments have been described, including corticosteroids, antimalarials, dapsone, and immunomodulators. Our patient responded well to systemic corticosteroids and hydroxychloroquine, consistent with previous reports. [5-7]
Conclusion
Eosinophilic annular erythema is an important differential
diagnosis in chronic annular dermatoses. Histopathological
evaluation is essential for accurate diagnosis and appropriate
management.
References
Citation
Bhattacharya S. Eosinophilic Annular Erythema Presenting as Chronic Polycyclic Plaques: A Clinicopathological Case Report. Indian J Dermatol Res. 2026;4(1): 108.