Case Report
Nevoid Hyperkeratosis of the Nipple and Areola: A Bilateral Idiopathic Presentation in a Young Female
Shatanik Bhattacharya
Department of Dermatology, Venereology & Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India
*Corresponding author:Dr. Shatanik Bhattacharya, Department of Dermatology, Venereology & Leprosy, Prafulla Chandra Sen Government Medical College, Arambag, India E-mail Id: shatanik.bhattacharya.97@gmail.com
Copyright: © 2026 Bhattacharya S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 10/02/2026; Accepted: 23/03/2026; Published: 25/03/2026
Abstract
Background: Nevoid hyperkeratosis of the nipple and areola (NHNA) is a rare benign dermatosis characterized by verrucous thickening and hyperpigmentation of the nipple–areola complex. It is frequently misdiagnosed due to its resemblance to inflammatory and malignant conditions.
Case Report: A 25-year-old female presented with a two-year history of progressive discoloration and thickening of both areolas. The condition began as pink, scaly eczematous plaques that gradually darkened and became verrucous. There was no history of atopy, nipple discharge, malignancy, drug intake, or systemic illness. Examination revealed bilateral diffuse brown hyperpigmentation with papillomatous thickening of the nipple–areola complex. No mass, lymphadenopathy, or nipple retraction was detected. Histopathology showed marked acanthosis, papillomatosis, filiform rete ridges with anastomosis, basal layer hyperpigmentation without melanocytic proliferation, and mild upper dermal fibrosis. A diagnosis of idiopathic NHNA was established.
Conclusion: Awareness of NHNA and its clinicopathological correlation is essential to avoid misdiagnosis, particularly of Paget’s disease or malignant acanthosis nigricans. Early recognition allows appropriate conservative or procedural management.
Case Report: A 25-year-old female presented with a two-year history of progressive discoloration and thickening of both areolas. The condition began as pink, scaly eczematous plaques that gradually darkened and became verrucous. There was no history of atopy, nipple discharge, malignancy, drug intake, or systemic illness. Examination revealed bilateral diffuse brown hyperpigmentation with papillomatous thickening of the nipple–areola complex. No mass, lymphadenopathy, or nipple retraction was detected. Histopathology showed marked acanthosis, papillomatosis, filiform rete ridges with anastomosis, basal layer hyperpigmentation without melanocytic proliferation, and mild upper dermal fibrosis. A diagnosis of idiopathic NHNA was established.
Conclusion: Awareness of NHNA and its clinicopathological correlation is essential to avoid misdiagnosis, particularly of Paget’s disease or malignant acanthosis nigricans. Early recognition allows appropriate conservative or procedural management.
Keywords:Nevoid Hyperkeratosis; Nipple; Areola; Verrucous Lesion; Benign Dermatosis
Introduction
Nevoid hyperkeratosis of the nipple and areola (NHNA) is a rare
benign dermatological condition characterized by hyperkeratotic,
verrucous thickening and hyperpigmentation of the nipple–areola
complex. The condition predominantly affects young women
and is frequently bilateral. Although benign, it often raises clinical
concern because it may mimic inflammatory dermatoses or
malignant conditions such as Paget’s disease of the breast. Therefore,
histopathological evaluation is essential to establish the diagnosis and
rule out malignancy.
Nevoid hyperkeratosis of the nipple and areola (NHNA) was first classified by Levy-Frenckel in 1938 into three types:
(1) associated with epidermal nevus,
(2) associated with other dermatoses such as acanthosis nigricans or ichthyosis, and
(3) idiopathic type without any associated systemic or cutaneous disease, which is most commonly seen in women of reproductive age. [1]
NHNA has been classified into three categories: lesions associated with epidermal nevus, lesions associated with systemic dermatoses, and idiopathic lesions occurring without underlying disease. The idiopathic variant is the most commonly encountered form in young females. We report a case of bilateral idiopathic NHNA in a young woman with characteristic clinical and histopathological findings.
Nevoid hyperkeratosis of the nipple and areola (NHNA) was first classified by Levy-Frenckel in 1938 into three types:
(1) associated with epidermal nevus,
(2) associated with other dermatoses such as acanthosis nigricans or ichthyosis, and
(3) idiopathic type without any associated systemic or cutaneous disease, which is most commonly seen in women of reproductive age. [1]
NHNA has been classified into three categories: lesions associated with epidermal nevus, lesions associated with systemic dermatoses, and idiopathic lesions occurring without underlying disease. The idiopathic variant is the most commonly encountered form in young females. We report a case of bilateral idiopathic NHNA in a young woman with characteristic clinical and histopathological findings.
Case Report
A 25-year-old female presented with a two-year history of
asymptomatic discoloration and progressive thickening of both
areolas. The condition initially began as a pink, scaly, eczematous
plaque over the areola, which gradually darkened and became
thickened over time. During the last two months, the lesions had
worsened, prompting the patient to seek medical attention.
There was no history of atopy, nipple discharge, breast malignancy, drug intake, pregnancy, or systemic illness. The patient denied any pruritus or pain associated with the lesions.
There was no history of atopy, nipple discharge, breast malignancy, drug intake, pregnancy, or systemic illness. The patient denied any pruritus or pain associated with the lesions.
Clinical Examination:
Dermatological examination revealed diffuse brownish
pigmentation and verrucous thickening involving the nipple–areola
complex of both breasts. The surface appeared dry, scaly, and mildly
erythematous with focal crusting. The lesions were well demarcated
and symmetrically distributed.“Clinical examination revealed diffuse
hyperpigmentation and verrucous thickening of the nipple–areola
complex [Figure 1].”“Closer inspection showed papillomatous surface and hyperkeratosis [Figure 2].”
“Lateral view demonstrated raised verrucous nipple thickening [Figure 3].”
No palpable breast mass, nipple retraction, discharge, or axillary lymphadenopathy was noted. The remainder of the cutaneous examination was unremarkable.
The patient was non-obese, and routine laboratory investigations were within normal limits.



Histopathological Findings
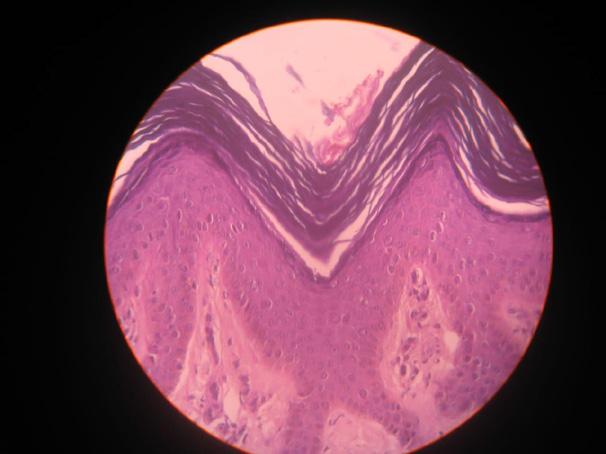
A punch biopsy specimen from the areolar lesion revealed the following features:
Marked orthokeratotic hyperkeratosis
Papillomatosis
Acanthosis
Downward filiform rete ridges anastomosing with each other
Basal layer hyperpigmentation without melanocytic proliferation
Keratotic plugging
Mild perivascular lymphocytic infiltration in the dermis
Mild fibrosis of the upper dermis.“Histopathology showed marked acanthosis, papillomatosis, and basal hyperpigmentation without atypia [Figure 4].”
These histopathological findings were consistent with nevoid hyperkeratosis of the nipple and areola.
Differential Diagnosis
Several dermatological and systemic conditions may mimic NHNA clinically. The differential diagnoses considered in this case included:
Nipple eczema with lichenification
Paget’s disease of the breast
Epidermal nevus
Malignant acanthosis nigricans
Seborrhoeic dermatitis
Seborrhoeic keratosis
A punch biopsy specimen from the areolar lesion revealed the following features:
Marked orthokeratotic hyperkeratosis
Papillomatosis
Acanthosis
Downward filiform rete ridges anastomosing with each other
Basal layer hyperpigmentation without melanocytic proliferation
Keratotic plugging
Mild perivascular lymphocytic infiltration in the dermis
Mild fibrosis of the upper dermis.“Histopathology showed marked acanthosis, papillomatosis, and basal hyperpigmentation without atypia [Figure 4].”
These histopathological findings were consistent with nevoid hyperkeratosis of the nipple and areola.
Differential Diagnosis
Several dermatological and systemic conditions may mimic NHNA clinically. The differential diagnoses considered in this case included:
Nipple eczema with lichenification
Paget’s disease of the breast
Epidermal nevus
Malignant acanthosis nigricans
Seborrhoeic dermatitis
Seborrhoeic keratosis
Graft-versus-host disease
Pregnancy-associated hyperkeratosis of the nipple
Candidiasis of the nipple with mucocutaneous candidiasis
Drug-induced hyperkeratosis (e.g., sorafenib therapy)
Darier disease
Areolar melanosis
Histopathological evaluation excluded these conditions and confirmed the diagnosis of NHNA.
Management
Management of NHNA is mainly aimed at cosmetic improvement, as the condition is benign.
Medical Treatment
The following therapies have been reported:
Mild topical corticosteroids (e.g., hydrocortisone)
Topical retinoids
Topical calcipotriol
Systemic retinoids such as oral acitretin
Procedural Treatment
Several procedural options have been described:
Electrosurgical superficial removal of hyperkeratosis
Cryosurgery
Radiofrequency ablation
Carbon dioxide (CO₂) laser therapy
Surgical excision with reconstruction
In our patient, treatment consisted of oral isotretinoin (1 mg/ kg/day for three months) along with topical clobetasol–calcipotriol combination ointment. At follow-up after three months, the patient demonstrated partial flattening of the lesions with reduction in verrucosity.
Pregnancy-associated hyperkeratosis of the nipple
Candidiasis of the nipple with mucocutaneous candidiasis
Drug-induced hyperkeratosis (e.g., sorafenib therapy)
Darier disease
Areolar melanosis
Histopathological evaluation excluded these conditions and confirmed the diagnosis of NHNA.
Management
Management of NHNA is mainly aimed at cosmetic improvement, as the condition is benign.
Medical Treatment
The following therapies have been reported:
Mild topical corticosteroids (e.g., hydrocortisone)
Topical retinoids
Topical calcipotriol
Systemic retinoids such as oral acitretin
Procedural Treatment
Several procedural options have been described:
Electrosurgical superficial removal of hyperkeratosis
Cryosurgery
Radiofrequency ablation
Carbon dioxide (CO₂) laser therapy
Surgical excision with reconstruction
In our patient, treatment consisted of oral isotretinoin (1 mg/ kg/day for three months) along with topical clobetasol–calcipotriol combination ointment. At follow-up after three months, the patient demonstrated partial flattening of the lesions with reduction in verrucosity.
Discussion
NHNA is a rare benign disorder of keratinization involving
the nipple–areola complex. Although the exact etiology remains
unknown, hormonal influence has been suggested due to the
predominance of cases in women of reproductive age.
The clinical presentation typically includes verrucous thickening, hyperpigmentation, and hyperkeratosis of the nipple and areola. Lesions may be unilateral or bilateral but are most often symmetrical in idiopathic cases.
Histopathology plays a crucial role in diagnosis. The characteristic findings include orthokeratotic hyperkeratosis, papillomatosis, acanthosis, elongation of rete ridges, and basal hyperpigmentation without atypical cells. These features help differentiate NHNA from malignant conditions such as Paget’s disease.
Treatment options remain variable, and no standardized therapy exists. Topical agents such as corticosteroids, retinoids, and calcipotriol may reduce hyperkeratosis. Procedural treatments including laser therapy and radiofrequency ablation have shown good cosmetic outcomes. Systemic retinoids may also be effective due to their ability to regulate epidermal differentiation and keratinization.
The clinical presentation typically includes verrucous thickening, hyperpigmentation, and hyperkeratosis of the nipple and areola. Lesions may be unilateral or bilateral but are most often symmetrical in idiopathic cases.
Histopathology plays a crucial role in diagnosis. The characteristic findings include orthokeratotic hyperkeratosis, papillomatosis, acanthosis, elongation of rete ridges, and basal hyperpigmentation without atypical cells. These features help differentiate NHNA from malignant conditions such as Paget’s disease.
Treatment options remain variable, and no standardized therapy exists. Topical agents such as corticosteroids, retinoids, and calcipotriol may reduce hyperkeratosis. Procedural treatments including laser therapy and radiofrequency ablation have shown good cosmetic outcomes. Systemic retinoids may also be effective due to their ability to regulate epidermal differentiation and keratinization.
Conclusion
Nevoid hyperkeratosis of the nipple and areola is an
uncommon benign dermatosis that may mimic inflammatory or
malignant conditions of the breast. Accurate diagnosis requires
clinicopathological correlation. Recognition of this entity is
important to prevent unnecessary anxiety and invasive investigations.
Both medical and procedural treatments may be used for cosmetic
improvement, with systemic retinoids showing promising results in
selected cases.
References
Citation
Bhattacharya S. Nevoid Hyperkeratosis of the Nipple and Areola: A Bilateral Idiopathic Presentation in a Young Female. Indian J Dermatol Res. 2026;4(1): 106.