Case Series
Invasive Fusariosis: Case Series and Review of the Fusarium Infection
Ruiz-Beguerie J1*, Barbini C1, Busso C1 and Anaya J2
1Dermatology Department, Austral University Hospital, Argentina
2Pathology Department, Austral University Hospital, Argentina
Corresponding author: Ruiz-Beguerie J, Dermatology Department, Austral University Hospital, Av Peron 1500, Derqui, Buenos Aires, Argentina, E-mail: jruiz@cas.austral.edu.ar; julietarb8@gmail.com
Citation: Ruiz-Beguerie J, Barbini C, Busso C, Anaya J. Invasive Fusariosis: Case Series and Review of the Fusarium Infection. Indian J Dermatol Res. 2019;1(1): 102.
Copyright ©2019 Ruiz-Beguerie J, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Dermatological Research | Volume: 1, Issue: 1
Submission: 29/03/2019; Accepted: 27/05/2019; Published: 30/05/2019
Abstract
Fusarium species cause a broad spectrum of infections in human beings, including superficial, locally invasive and disseminated infections. The clinical manifestations of fusariosis depend on the portal of entry of the infection and the intensity and duration of immunosuppression. Disseminated infections typically occur among the severely immunocompromised patients as it occurred to the individuals we are reporting in this article.
These infections may be clinically suspected on the basis of a combination of clinical manifestation, prolonged fever and laboratory findings, which should lead to prompt therapy avoiding the high rate of death in these patients. Treatment options include amphotericin B, voriconazole and posaconazole. Classification of high-risk patients and preventive measures of fusarial infection among them should be considered.
This manuscript summarizes the main aspects of morphology, pathology and toxigenicity of the Fusarium species while reporting three cases of disseminated fusariosis which occurred this current year at the Austral University Hospital in Buenos Aires, Argentina.
Keywords:
Fusarium; Fusariosis infection; Fungal; Disseminated fusariosis
Introduction
Fusarium species are widely distributed in soil; subterranean and aerial plant parts, plant debris and other organic substrates. They are present in water worldwide as part of water structure biofilms [1]. The widespread distribution of Fusarium species (spp.) may be attributed to their ability to grow on a wide range of substrates and their efficient dispersal mechanisms [2].
More than 50 species of Fusarium are already identified but only twelve species are associated with infection. Fusarium spp. possesses several virulence factors, including the ability to produce mycotoxins, such as trichothecenes, which suppress humoral and cellular immunity and even cause tissue breakdown. In addition, Fusarium spp. has the ability to adhere to prosthetic material and to produce proteases and collagenases. Fusarium solani is the most virulent among this specie [3].
In a review published in 2002 by Nucci and colleagues, Fusarium solani was the most frequent among the 259 cases (50% of cases), followed by Fusarium oxysporum in 20% and Fusarium verticillioides together with Fusarium moniliforme (10% each). Others, which were found included Fusarium dimerum, Fusarium proliferatum, Fusarium chlamydosporum, Fusarium sacchari, Fusarium nygamai, Fusarium napiforme, Fusarium antophilum and Fusarium vasinfectum [4].
The principal portal of entry for Fusarium spp. is the airways, followed by the skin at site of tissue breakdown and the mucosal membranes. Airborne fusariosis is thought to be acquired by the inhalation of airborne fusarial conidia, as suggested by the occurrence of sinusitis and pneumonia [5,6]. In a prospective study, Fusarium was recovered from a hospital water system (water, water storage tanks, shower and sink drains, shower heads, and sink faucet aerators) as in our 3 cases reported in this manuscript [7]. In the mentioned study, they also recovered this fungal pathogen from hospital air and other environments. Hence, they supported the risk of nosocomial waterborne fusariosis [7,8].
Fusarium is a fungal pathogen of universal distribution which causes important plant diseases such as crown rot, head blight, and scab on cereal grains [1]. This brings as a result mycotoxin contamination of food and feed products. Among the most important mycotoxins produced by Fusarium spp. are the trichothecenes and the fumonisins. These last ones cause fatal livestock diseases and are considered potentially carcinogenic mycotoxins for humans, while trichothecenes are potent inhibitors of protein synthesis [9].
The clinical form of fusariosis depends largely on the immune status of the host and the portal of entry. The superficial and localized form of disease occurs mainly in immunocompetent hosts and invasive or disseminated disease affects immunocompromised patients [4].
Case 1
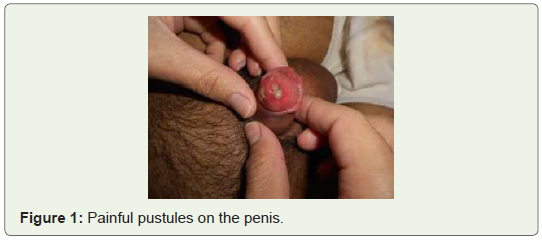
Male patient, 24 years old, with diagnosis of Acute Lymphocytic Leukemia and allogeneic transplant in 2007. In September 2018, after a relapse he started with intrathecal chemotherapy (dexamethasone, methotrexate and cytarabine) and intravenous administration of clofarabine and etoposide. Firstly, he presented with painful papules on the trunk and a necrotic lesion involving the penis accompanied by neutropenia of more than 15 days. After a curettage and culture, Fusarium infection was diagnosis and he started amphotericin B but a sepsis and death overcame soon after (Figure 1).
Case 2
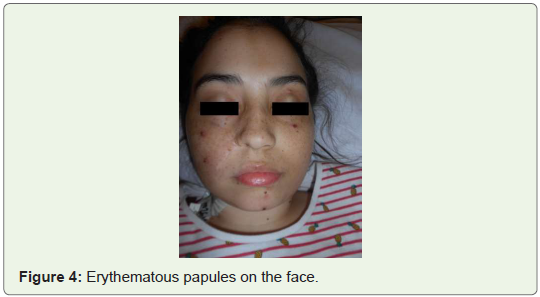
Female patient of 24 years old with a diagnosis of Acute Lymphoblastic Leukemia in 2005 had skin and sinusal aspergillosis infection that same year. She was treated with voriconazole and amphotericin B with good evolution. In June of last year, with a leukemia relapse, multiple erythematous nodules appeared on her legs and arms (Figure 2-4). A deep skin biopsy was done with the diagnosis of Fusarium fujikuroi, which was also found in blood cultures. Amphotericin B 7mg/kg/dia+ oral voriconazole started before she came out of neutropenia and she was discharged with oral voriconazole (300mg/12hs) for 6 months.


Case 3
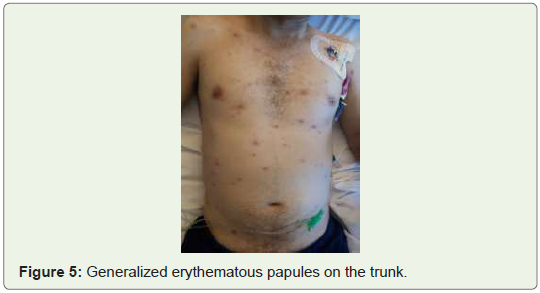
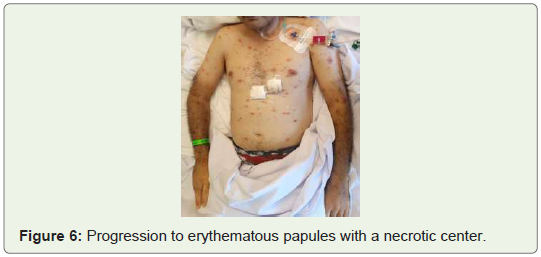
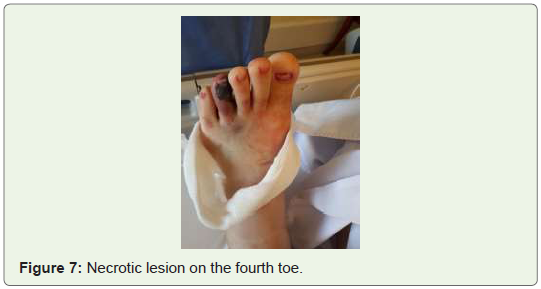
Male patient of 38 years old, with a diagnosis of Acute Myeloid Leukemia with generalized erythematous papules and pustules accompanied by prolonged neutropenia and fever while receiving antibiotics (imipenem, amikacin and piperacillin tazobactam) plus amphotericin B (Figure 5-7). Some weeks before he had a toe infection, which was treated with surgery debridement and oral antibiotics. In the CT scan of sinuses, thorax and abdomen there were some infiltrative images, which were interpreted as septic embolism. Skin biopsy, blood and urine culture and bronchoalveolar lavages were done which confirmed disseminated fusariosis with lung involvement. Voriconazole was added to the treatment without response, finally dying in the intensive care unit of the Austral Hospital.
The innate immunity plays a major role in the defense against mold infections [10].
Macrophages and neutrophils damage fusarial hyphae, by gamma interferon, Granulocyte Colony-Stimulating Factor (G-CSF), Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF) and interleukin-15. The effect of interleukin-15 is mediated by the release of interleukin-8 and by direct stimulation of hyphal damage. Although little is understood about Toll-like receptors and Fusarium, it is believed to be important in invasive fusariosis [11,12].
The superficial form of human infection with Fusarium is seen as keratitis (specially in contact lenses wearers) and onychomycosis. Other non disseminated infections by this agent are sinusitis, septic arthritis, and osteomyelitis, thrombophlebitis or endophthalmitis and pneumonia [13-18].
The most important risk factors for severe fusariosis include prolonged neutropenia and T-cell immunodeficiency, especially in hematopoietic stem cell transplant recipients with severe graftversus- host disease. These last concepts are considered when the neutropenia is prolonged more than 10 days in a row and less than 100/mm3. Other risk factors to consider are skin breakdown close to onychomycosis by Fusarium, prolonged corticoid therapy, diagnosis of aplastic anemia, acute leukemia and allogeneic hematopoietic stem cell transplantation.
The most frequent presentation of disseminated fusariosis is a cutaneous manifestation accompanied by a positive blood culture, with or without lung or sinus involvement. Once recovered the neutropenia, the prognostic of the Fusarium infection improves [4]. The Fusarium infection can develop in any human organ. Fever and skin lesions especially in the face and extremities frequently appeared. These skin lesions can be nodules, erythematous papules and macules, target lesions, which sometimes can have necrotic centers. Cellulitis with or without fasciitis can be diagnosed as well. Lung involvement is associated with higher mortality, even after controlling for immune status.
Fusarium systemic dissemination is considered as having two or more organs involved. It is believed that when a hospitalized patient develops Fusarium infection, the fungus probably have been inside the body before checking in and while in the hospital with the immune system compromised, the fungus develop the systemic infection, as it is considered an opportunistic fungus.
Alert of disseminated fusariosis in the severely immunocompromised patients is brought up when skin lesions in the form of cellulitis or papules appear and a positive blood cultures for mold is received. Blood cultures are frequently positive in fusariosis unlike other severe fungal infection such as aspergillosis due to the fact that Fusarium spp. produces yeast-like structures (adventitious sporulation) that facilitate their dissemination and growth in the blood [19].
The prognosis of disseminated fusariosis is poor and the level of immunosuppression and the extent of the infection determine it. The death rate in persistent neutropenic hosts is close to 100% [4]. The prognosis of fusariosis in the immunocompromised host is directly related to the immune status of the patient, with high death rates in patients with persistent immunodeficiency. Host of HSCT and presence of persistent neutropenia, disseminated disease, and lung involvement predict fatal development [4]. By contrast, patients who had no risk factors as mentioned above or whose only risk factor was high or prolonged corticosteroid therapy have a 67% and 30% survival rates, respectively (P < 0.0001) [4,6].
Severe T-cell immunodeficiency is the major risk factor for fusariosis in the group of patients who had Hematopoietic Stem Cell Transplant (HSCT) [20]. The overall incidence of fusariosis is 6 cases per 1,000 HSCTs. The incidence is lowest (1.5 to 2/1,000) among autologous recipients, intermediate (2.5 to 5/1,000) in matched related and matched unrelated allogeneic recipients, and highest (20/1,000) among recipients of mismatched related donor allogeneic HSCTs [20]. Locally invasive and usually late infections may also develop among solid organ transplant recipients, but these appear to be less common than those among HSCT patients [21] (Table 1).
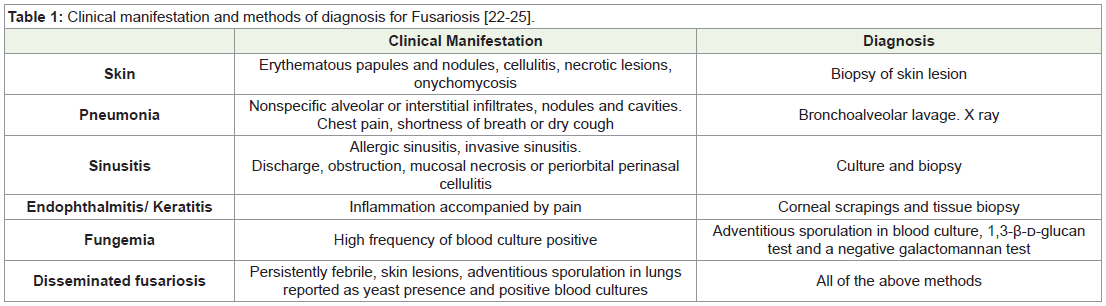
The diagnosis comes from biopsies or cultures with Fusarium isolation. The 1,3-β-D-glucan test is usually positive in invasive fusarial infections but cannot distinguish Fusarium from Candida, Aspergillus or Trichosporon, which are also detected by this method of diagnosis. However, in a high-risk patient with fungal infection is highly suggestive of fusariosis is a positive 1,3-β-D-glucan test and a negative galactomannan test, which would be positive in case of aspergillosis. Additionally, PCR technique can be used for the detection of Fusarium spp. in blood and tissue [22,23].
Diagnostic work up with Fusarium infection
1. Culture and biopsy of skin site or sinus if involvement suspected.
2. Bronchoalveolar lavage and biopsy if pneumonia suspected.
3. Blood culture, 1,3-β-D-glucan test, galactomannan test (positive in aspergillosis).
4. Check for adventitious sporulation in blood and tissue biopsies as it is found in fusariosis and not in aspergillosis.
Microbiologist must be very cautious in diagnosing Fusarium infection, because Fusarium spp. may contaminate laboratory specimens and pseudo-outbreaks of fusariosis may occur giving away a false positive [24]. In tissue, the hyphae are similar to those of Aspergillus spp. with hyaline and septate filaments that typically dichotomize in acute and right angles. However, adventitious sporulation may be present in tissue and is highly suggestive of fusariosis especially in the high-risk population [25].
The European Organization for Research and Treatment of Cancer and the Mycoses Study Group classify invasive fungal disease in three types: proven, probable and possible. Based on this classification it is defined as a proven invasive fungal infection if the fungus is detected in the histological analysis or in a culture of a sample of tissue obtained from a site of the disease or from blood. “Probable” depends on the simultaneous presence of 3 elements: the factors of the host, the clinical manifestations of mycosis and the mycological evidence in the laboratory. If it meets the criteria of a host factor plus the clinical manifestation, but does not meet the mycological lab evidence it is considered “possible”. It should be noted that in the three patients mentioned above, a proven invasive fungal disease was defined, since they met the criteria of the host, the clinical criteria and the demonstration of fungal elements in tissues with positive culture for Fusarium [26].
Treatment of localized infection in these patients result beneficial by surgical debridement, while disseminated infection requires the use of systemic agents and immunotherapy. Localized skin lesions in immunocompromised patients deserve special attention, since the skin may be the source for disseminated infections. Hence, local debridement should be performed and topical natamycin or amphotericin B should be used before starting with immunosuppressive therapies.
Keratitis is usually treated with topical natamycin or else topical and oral voriconazole [27]. Depending on the Fusarium species, the susceptibility to treatments. Usually the treatments of choice are voriconazole and posaconazole or amphotericin B. Data on combination therapy for fusariosis are limited to a few case reports with no solid recommendation: caspofungin plus amphotericin B, amphotericin B plus voriconazole, amphotericin B and terbinafine, and voriconazole plus terbinafine [21,28-30]. Special air filters, such as HEPA filters in hospitals are important to control airborne indoor fungi. This filter consists of a High Efficiency Particulate Air (HEPA)- type filter, filtering virus, bacteria, fungus and molecules up to 1.0μm size particles. Fusarium spores can easily be carried by wind, causing transmission and subsequent infection to humans. Suggesting that the air may be a potential source for fusariosis in an indoor environment such as a hospital [31].
Conclusion
In a hospital where there are high-risk patients, efforts should be done to avoid fungal infection. Patients should be put in rooms with HEPA filters (High Efficiency Particulate Air) and positive pressure, avoiding contact with reservoirs of Fusarium spp. such as tap water, and cleaning the shower facilities and floors with chlorhexidine, prior to the use by high-risk patients [7,30-32]. Monitoring fungal aero contamination in hospitals is an essential measure to prevent severe invasive infections. Fusariosis is a very serious condition, with greater mortality in T-cell immune-incompetent patients in intensive care units and in non-neutropenic hosts treated with corticosteroids or lifelong immunosuppressant medication.
References
- Nelson PE, Dignani MC, Anaissie EJ (1994) Taxonomy, biology, and clinical aspects of Fusarium species. Clin Microbiol Rev 7: 479-504.
- Burgess LW (1981) General ecology of the fusaria. In: Nelson PE, Toussoun TA, Cook RJ (eds.), Fusarium: diseases, biology, and taxonomy. Pennsylvania State University Press, Philadelphia, pp: 225-235.
- Nucci M, Anaissie E (2007) Fusarium Infections in Immunocompromised Patients. Clin Microbiol Rev 20: 695-704.
- Nucci M, Anaissie E (2002) Cutaneous infection by Fusarium species in healthy and immunocompromised hosts: implications for diagnosis and management. Clin Infect Dis 35: 909-920.
- Boutati EI, Anaissie EJ (1997) Fusarium, a significant emerging pathogen in patients with hematologic malignancy: ten years’ experience at a cancer center and implications for management. Blood 90: 999-1008.
- Nucci M, Anaissie EJ, Queiroz-Telles F, Martins CA, Trabasso P, et al. (2003) Outcome predictors of 84 patients with hematologic malignancies and Fusarium infection. Cancer 98: 315-319.
- Anaissie EJ, Kuchar RT, Rex JH, Francesconi A, Kasai M, et al. (2001) Fusariosis associated with pathogenic Fusarium species colonization of a hospital water system: a new paradigm for the epidemiology of opportunistic mold infections. Clin Infect Dis 33: 1871-1878.
- O’Donnell K, Sutton DA, Rinaldi MG, Magnon KC, Cox PA, et al. (2004) Genetic diversity of human pathogenic members of the Fusarium oxysporum complex inferred from multilocus DNA sequence data and amplified fragment length polymorphism analyses: evidence for the recent dispersion of a geographically widespread clonal lineage and nosocomial origin. J Clin Microbiol 42: 5109-5120.
- Munkvold GP (2017) Fusarium species and their associated mycotoxins. Methods Mol Biol 1542: 51-106.
- Shoham S, Levitz SM (2005) The immune response to fungal infections. Br J Haematol 129: 569-82.
- Gaviria JM, van Burik JA, Dale DC, Root RK, Liles WC (1999) Comparison of interferon-gamma, granulocyte colony-stimulating factor, and granulocyte-macrophage colony-stimulating factor for priming leukocyte-mediated hyphal damage of opportunistic fungal pathogens. J Infect Dis 179: 1038-1041.
- Sridhar H, Subramanyam JR, Appaji L, Shafiulla M, Vijaykumar BR (2001) Fusarium solani fungemia in a patient with acute lymphoblastic leukemia. Indian J Cancer 38: 19-21.
- Kurien M, Anandi V, Raman R, Brahmadathan KN (1992) Maxillary sinus fusariosis in immunocompetent hosts. J Laryngol Otol 106: 733-736.
- Jakle C, Leek JC, Olson DA, Robbins DL (1983) Septic arthritis due to Fusarium solani. J Rheumatol 10: 151-153.
- Bourguignon RL, Walsh AF, Flynn JC, Baro C, Spinos E (1976) Fusarium species osteomyelitis. Case report. J Bone Joint Surg Am 58: 722-723.
- Murray CK, Beckius ML, McAllister K (2003) Fusarium proliferatum superficial suppurative thrombophlebitis. Mil Med 168: 426-427.
- Madhavan M, Ratnakar C, Veliath AJ, Kanungo R, Smile SR, et al. (1992) Primary disseminated fusarial infection. Postgrad Med J 68: 143-144.
- Ma LJ, Geiser DM, Proctor RH, Rooney AP, O’Donnell K, et al. (2013) Fusarium pathogenomics. Annu Rev Microbiol 67: 399-416.
- Liu K, Howell DN, Perfect JR, Schell WA (1998) Morphologic criteria for the preliminary identification of Fusarium, Paecilomyces, and Acremonium species by histopathology. Am J Clin Pathol 109: 45-54.
- Nucci M, Marr KA, Queiroz-Telles F, Martins CA, Trabasso P, et al. (2004) Fusarium infection in hematopoietic stem cell transplant recipients. Clin Infect Dis 38: 1237-1242.
- Sampathkumar P, Paya CV (2001) Fusarium infection after solid-organ transplantation. Clin Infect Dis 32: 1237-1240.
- Odabasi Z, Mattiuzzi G, Estey E, Kantarjian H, Saeki F, et al. (2004) Beta-D-glucan as a diagnostic adjunct for invasive fungal infections: validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin Infect Dis 39: 199-205.
- Ostrosky-Zeichner L, Alexander BD, Kett DH, Vazquez J, Pappas PG, et al. (2005) Multicenter clinical evaluation of the (1-->3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis 41: 654-659.
- Grigis A, Farina C, Symoens F, Nolard N, Goglio A (2000) Nosocomial pseudo-outbreak of Fusarium verticillioides associated with sterile plastic containers. Infect Control Hosp Epidemiol 21: 50-52.
- Hayden RT, Isotalo PA, Parrett T, Wolk DM, Qian X, et al. (2003) In situ hybridization for the differentiation of Aspergillus, Fusarium, and Pseudallescheria species in tissue section. Diagn Mol Pathol 12: 21-26.
- De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, et al. (2008) Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 46: 1813-1821.
- Bunya VY, Hammersmith KM, Rapuano CJ, Ayres BD, Cohen EJ (2007) Topical and oral voriconazole in the treatment of fungal keratitis. Am J Ophthalmol 143: 151-153.
- Makowsk MJ, Warkentin DI, Savoie ML (2005) Caspofungin and amphotericin B for disseminated Fusarium verticillioides in leukemia. Ann Pharmacother 39: 1365-1366.
- Durand-Joly I, Alfandari S, Benchikh Z, Rodrigue M, Espinel-Ingroff A, et al. (2003) Successful outcome of disseminated Fusarium infection with skin localization treated with voriconazole and amphotericin B-lipid complex in a patient with acute leukemia. J Clin Microbiol 41: 4898-4900.
- Howden BP, Slavin MA, Schwarer AP, Mijch AM (2003) Successful control of disseminated Scedosporium prolificans infection with a combination of voriconazole and terbinafine. Eur J Clin Microbiol Infect Dis 22: 111-113.
- Moretti ML, Busso-Lopes AF, Tararam CA, Moraes R, Muraosa Y, et al. (2018) Air borne transmission of invasive fusariosis in patients with hematologic malignancies. PLoS One 13: e0196426.
- Anaissie EJ, Stratton SL, Dignani MC, Lee CK, Mahfouz TH, et al. (2002) Cleaning patient shower facilities: a novel approach to reducing patient exposure to aerosolized Aspergillus species and other opportunistic molds. Clin Infect Dis 35: E86-E88.