Research Article
Socio-Demographic Profile of HIV Seropositive Patients in a Tertiary Care Hospital in Vadodara - A 5 Year ICTC Record Based Study
Rashmi M, Srishti J*, Kishan N and Som L
Department of Dermatology, Sumandeep Vidyapeeth, India
Corresponding author: Srishti J, 2nd year MD Resident, Department of Dermatology, Sumandeep Vidyapeeth, Vadodara, India, Tel no: 9638639617/9810536424; E-mail: dr.srish.jain@gmail.com
Citation: Rashmi M, Srishti J, Kishan N, Som L. Socio-Demographic Profile of HIV Seropositive Patients in a Tertiary Care Hospital in Vadodara - A 5 Year ICTC Record Based Study. Indian J Dermatol Res. 2019;1(1): 101.
Copyright ©2019 Rashmi M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Dermatological Research | Volume: 1, Issue: 1
Submission: 15/03/2019; Accepted: 17/04/2019; Published: 20/04/2019
Abstract
Background: An Integrated Counselling and Testing Centre (ICTC) is a place where counselling and testing of a person is done for HIV, of his own free will or as advice of a medical provider [1]. It is necessary to understand the socio-demographic profile and risk behaviour of attendees of ICTC in order to create awareness and hence achieve disease control.
Aim: To study the socio-demographic characteristics of patients attending the ICTC of a tertiary care hospital in Vadodara, Gujarat.
Objectives: To study the trend of HIV positive cases attending the ICTC over a period of 5 years; to study the socio-demographic features and route of transmission among HIV seropositive clients; to find out the prevalence of HIV-TB co-infection; to determine the prevalence of HIV positive cases among the ante-natal cases attending the ICTC; to find out prevalence of pediatric cases among the seropositive cases.
Materials and Methods: Records of all patients attending ICTC in Dhiraj Hospital, Vadodara over a period of 5 years from April 2013 to March 2018 were obtained to carry out a retrospective observational study. HIV seropositive patients were analysed for various parameters. Chi square test was used wherever applicable. Data is presented in the form of percentages and bar charts.
Results: Between the year 2013-14 to 2017-18: Total HIV seropositive cases decreased from 3.16% (64.52% males) to 2.72% (82.0% males); antenatal cases newly detected positive for HIV decreased from 0.24% to 0.13%; spouse HIV seropositivity rate decreased from 25.81% to 16%; TB-HIV co-infection increased from 4.84% to 6.0%. Most of the HIV seropositive patients were above 50 yrs. of age (32.38%), married (65.40%), most males were labourers by occupation (64.86%) and females were housewives (44.09%), majority were illiterate (60.32%), belonging to rural areas (89.84%), most common route of transmission was by the sexual contact (96.83%). Marital Status and Occupation were found to have significant p value (< 0.05) with respect to HIV positive serostatus.
Conclusion: Data generation in ICTC provides an important clue in understanding the epidemiology in a particular geographic region and local planning for new models of care and cost-effective treatment of those infected with HIV and preventive strategies for those at risk in order to reduce new infections. This will also be useful for State AIDS Control Society (SACS) to plan and arrange for resources to deal with the future situation.
Keywords:
HIV; ICTC; Socio-demographic
Introduction
“Investment in AIDS will be repaid a thousand-fold in lives saved and communities held together.” -Dr. Peter Piot, Former Executive Director, UNAIDS [2].
HIV can result in fatal illness that breaks down the body’s immune system, hence leaves the victim vulnerable to a number of life threatening opportunistic infections, neurological disorders, or unusual malignancies [3].
As per the India HIV Estimation report of 2017, National adult (15 - 49 years) HIV prevalence in India has been estimated at 0.22% (0.16% - 0.30%) in the year 2017. Among males, adult HIV prevalence has been estimated at 0.25% (0.18 - 0.34) while among females, it is estimated at 0.19% (0.14 - 0.25) in the year 2017. At the national level, the adult HIV prevalence has been shown to continue its steady decline from an estimated peak of 0.38% in the year 2001 - 2003 through 0.34% in 2007, 0.28% in 2012 and 0.26% in 2015 to 0.22% in 2017 [4].
An Integrated Counselling and Testing Centre (ICTC) is a place where counselling and testing of a person is done for HIV, of his own free will or as advice of a medical provider.
An ICTC serves as an entry point to services of support and care, providing people with opportunities to learn about and hence accept their HIV serostatus in a confidential environment. It aims at reducing the psycho-social stress of the person [5]. It is the foremost interface between the public health system and the individual with a will to get tested [6]. Data generation by ICTC helps by providing necessary clues and understanding the disease epidemiology in specified areas, along with risk behaviour pattern of the population.
In countries with poor resources, like India, integrated counselling and testing may be considered a cost-effective method to reduce the transmission of HIV [5].
ICTC
Integrated Counselling and Testing Centre (ICTC) was 1st developed in India in the year 1997 [1]. An integrated counselling and testing centre is a place where a person is counselled and tested for HIV, on his own free will or as advised by a medical provider and convinced that the test is mandatory. He/She is assured that the process will be confidential. The main functions of an ICTC include early detection of HIV; providing basic information on modes of transmission and prevention of HIV/AIDS to promote behavioural change and reduce vulnerability; linking positive people with other HIV prevention, care and treatment services; follow up counselling; Preventing Parent to Child Transmission (PPTCT); cross referrals - TB/STI/ART/TI-NGO/DIC/CCC etc. There are more than 9400 ICTC Centers in India, mainly located in the government hospitals [1]. Approximately 1621 ICTC Centers are there in Gujarat.
The Challenge lies in making all HIV Infected People in the Country and Gujarat aware of their status so that they adopt healthy life styles and hence prevent the transmission of HIV to others, and access life- saving care and treatment.
Elements of HIV counselling
A confidential dialogue; evaluating personal risk of HIV transmission and facilitating preventive behaviour; helping them to make a decision about whether to be tested or not. Providing support and facilitated decision-making following testing.
Under NACP-III, Voluntary Counselling and Testing Centres (VCTC) and facilities providing Prevention of Parent to Child Transmission of HIV/AIDS (PPTCT) services were remodelled as a hub or Integrated Counselling and Testing Centre (ICTC) for providing services to all clients under one roof.
Commonly used screening tests are
Enzyme Linked Immunosorbent Assay (ELISA) and rapid tests which include immunoconcentration/ dot blot assay (vertical flow), agglutination assay, immunochromatographic assay (lateral flow), dipstick and comb assay based on Enzyme Immune Assay (EIA).
To conclude, spreading awareness, strengthening the IEC (Information, Education, Communication) and early detection and treatment of HIV are the need of the hour towards making the nation disease-free.
This study was being undertaken with a view to understand the socio-demographic profile and risk behaviour of attendees of an Integrated Counselling and Testing Centre in a tertiary care hospital in Gujarat.
Aim
To study the socio-demographic characteristics of people attending the ICTC of a tertiary care hospital in Vadodara, Gujarat.
Objectives
Materials and Methods
This is an observational retrospective study undertaken at ICTC, Dhiraj Hospital, Sumandeep Vidyapeeth University, Vadodara. The approval had been taken from the institutional ethics committee. Data of all patients attending ICTC over a period of 5 years from April 2013 to March 2018 was collected. There were no specific exclusion criteria. Data was collected in the form of proforma and was analysed by descriptive statistical analysis using percentage and proportion. Chi square test was used wherever applicable.
Results
Data was analysed by descriptive statistical analysis using percentage and proportion. Chi square test was applied.
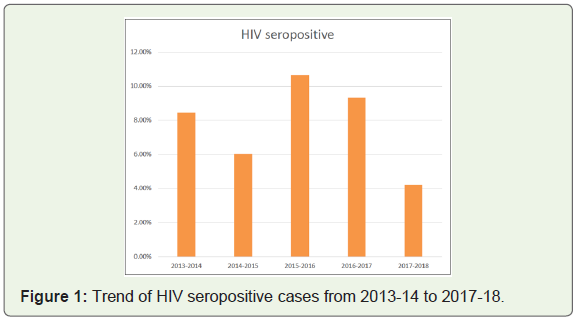
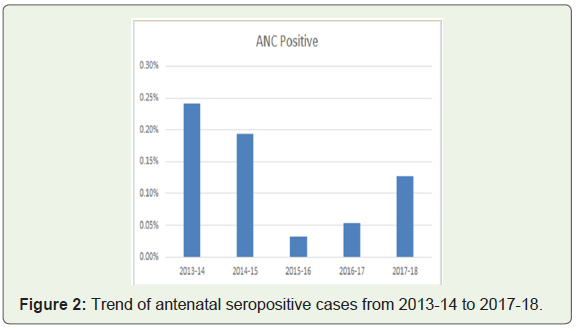
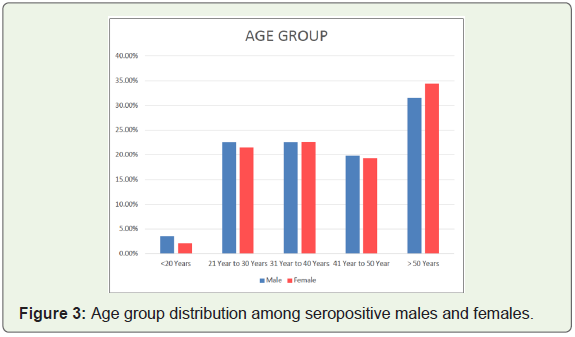
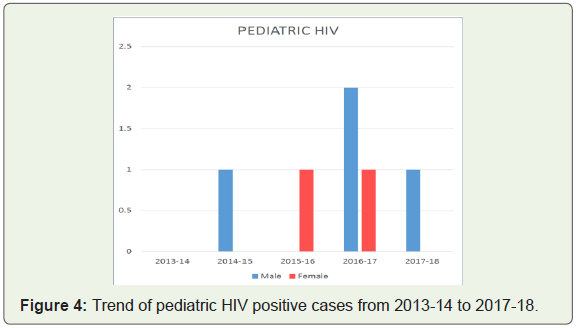
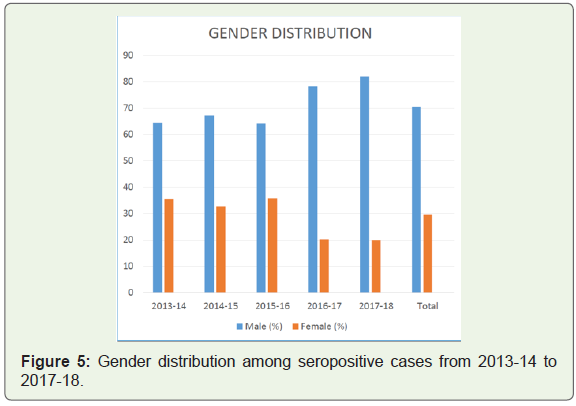
Total seropositive cases newly detected for HIV showed an increase from 3.16% (62/1961) in the year 2013-14 to 4.67% (81/1736) in the year 2015-16 and again underwent a decline to 2.72% (50/1839) in the year 2017-18 (Figure 1). Antenatal cases newly detected positive for HIV decreased from 0.24% (2/ 828) in 2013-14 to 0.13% (2/ 1576) in 2017-18 (Figure 2). Most (32.38%) of the HIV seropositive patients were above 50 yrs. of age (102/ 315), 31.53% (70/ 222) males and 34.41% (32/ 93) females (Figure 3). Among the pediatric age group, cases positive for HIV were none in the year 2013-14, 1 male was positive in 2014-15, 1 female in 2015-16, while in the year 2016-2017, 2 males and 1 female were HIV seropositive and 1 male was positive in the year 2017-18 (Figure 4). Males outnumbered the females among the seropositive cases persistently. Total number of seropositive males increased from 64.52% (40/ 62) in 2013-14 to 82.0% (41/ 50) in 2017-18 (Figure 5).
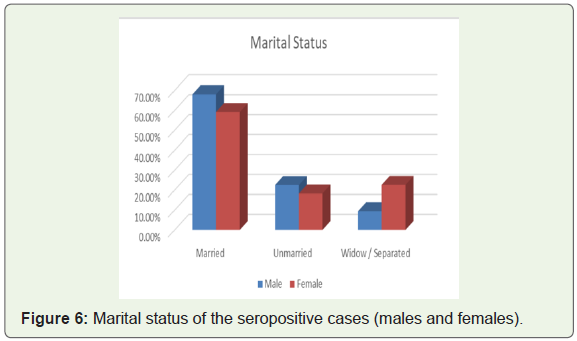
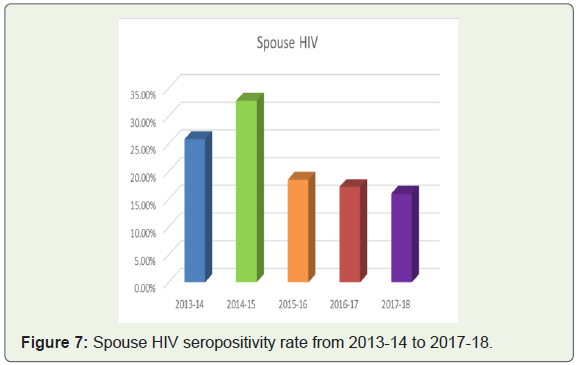
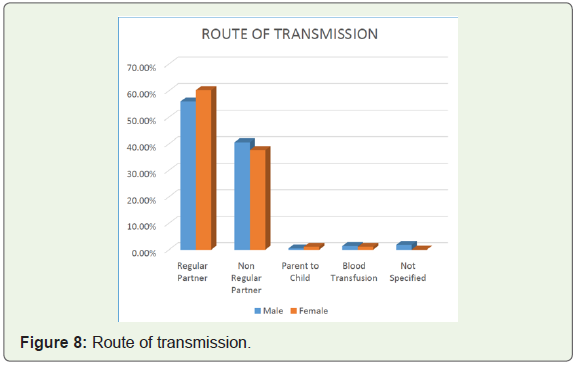
The social characteristics studied were marital status, route of transmission and sexual orientation of the patients. Most (65.40%) of the HIV seropositive patients were married (206/ 315) - 68.02% (151/ 222) males and 59.14% (55/ 93) females (Figure 6). Most of the patients were serodiscordant with their spouses. The spouse HIV seropositivity rate decreased from 35.5% (16/ 45) in the year 2013-14 to 20.5% (8/ 39) in the year 2017-18 (Figure 7). Heterosexual route was the most common route of transmission. Most patients reported regular sexual partner (57.14%), 39.68% admitted having non-regular partner, parent to child transmission rate was 0.63% and infection through blood transfusion was 1.27% (Figure 8).
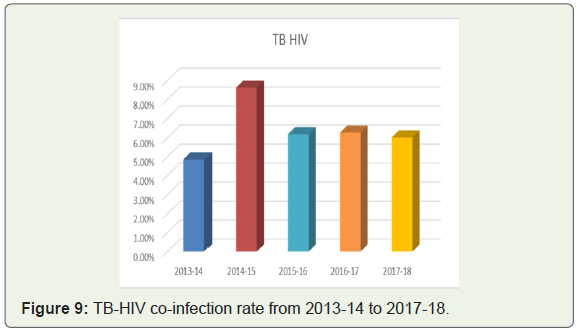
TB-HIV co-infection increased from 4.84% (3/ 62) in the year 2013-14 to 6.0% (3/ 50) in the year 2017-18 (Figure 9).
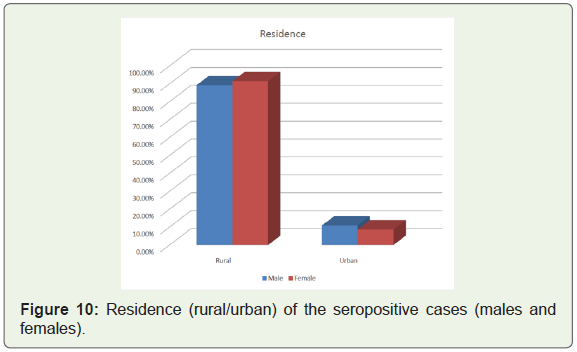
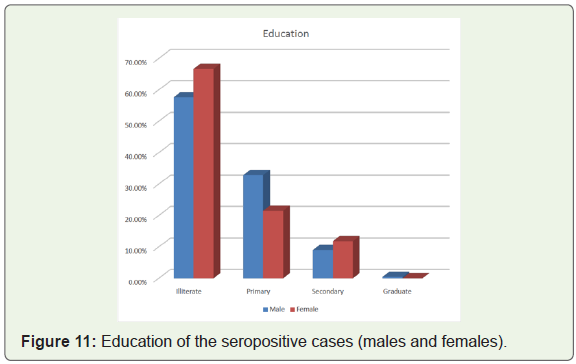
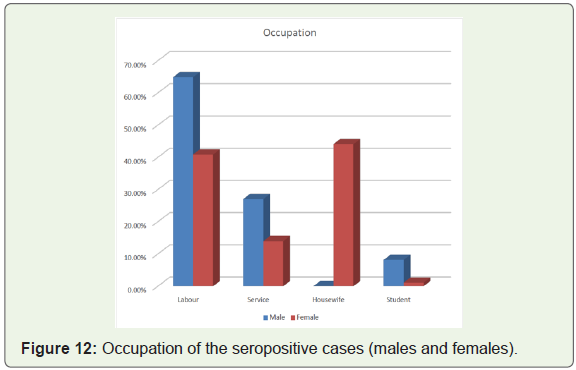
Majority of the seropositive patients (89.84%) were belonging to rural areas (283/ 315) - 89.19% (198/ 222) males and 91.40% (85/ 93) females (Figure 10). Majority (60.32%) were illiterate (190/ 315) - 57.66% (128/ 222) males and 66.67% (62/ 93) females (Figure 11). Most (64.86%) males were labourers by occupation (144/ 222) and most (44.09%) females were housewives (41/ 93) (Figure 12).
Marital Status and Occupation were found to have significant p value (< 0.05) with respect to HIV positive serostatus.
Discussion
HIV infection is one of the major infectious diseases in India, and since it has a chronic and lifelong course, its impact is huge as compared to the other infectious diseases.
Total newly detected HIV seropositive cases in our study decreased from 8.45% (62/ 734) to 4.23% (50/ 1182) from the year 2013-14 to 2017-18. This trend was similar to the national data. As per the India HIV estimations 2017, adult HIV prevalence (15-49 years) in Gujarat was 0.19%, with new HIV infections being 4518. There was a 41% decline in the new HIV infections rate from the year 2010 to 2017 [6].
The antenatal cases newly detected positive for HIV in our study decreased from 0.24% (2/ 828) to 0.13% (2/ 1576) from the year 2013-14 to 2017-18 while it was found to be 28% in a study by Dutt R, et al. [5].
Detection of antenatal HIV cases is necessary to prevent parent to child transmission.
The most common age group in our study was above 50 yrs of age. A study by Singh A et al showed similar results to our study with most common age group being affected between 41-60 years [7]. According to a comparison between UNAIDS 2013 estimates of HIV prevalence among the people aged 50 years and above and a survey data by Mahy, M et al. there was a constant increase in the number of people living with HIV aged 50 years and older between the year 1995 and 2013. Since 1995, there has been an increase by more than two-fold globally [8]. However, most common age group was 35-49 years in a study by Sanjiv Ahuja, et al. conducted in Uttar Pradesh [9].
Out of the HIV seropositive cases in our study, 1.91% was among the pediatric age group while the seropositivity rate among the pediatric age group was 8.77% in a study by Dutt R, et al. [5].
Majority (70.48%) of the HIV seropositive patients were males in our study. Similar results were found in studies by Haider, et al. [10], Deshpande, et al. [11], Sonani, et al. [12], Toshniwal, et al. [13], Kumari et al. [14].
96.83% patients had heterosexual route as the most common route of transmission. Similar results were seen in studies by Toshniwal, et al. [13], Nayak UB, et al. [15], Vaseem BN, et al. [16].
Most (65.4%) HIV positive patients in our study were married, results being similar in studies by Haider, et al. [10], Deshpande, et al. [11], Sonani, et al. [12], Toshniwal, et al. [13], Vaseem BN, et al. [16].
In our study, most of the spouses were serodiscordant with their seropositive partners (66.5%). Similar observations were made by Dutt R, et al. where 60.9% patients had seronegative spouses [5]. While spouse HIV seropositivity rate was 63.19% in a study by Singh A, et al. and 62.94% in a study by Joge, et al. which showed that most patients were seroconcordant with their spouses in these studies [7,17].
TB HIV co-infection was seen in 6.35% of the patients in our study while it was 29.82% in Dutt R, et al. [5]. Tuberculosis was found to be the most common opportunistic infection (62%) in a study by Deshpande, et al. [11]. Pulmonary tuberculosis was the most common opportunistic infection and was present in 19.7% of patients on ART in a study by Kumari, et al. [14].
There was a predominance of patients from rural locations (89.84%) in our study. Similar results were noted in studies by Singh A, et al. and Deshpande, et al. [7,11].
In our study, 60.32% patients were illiterate, 29.52% patients were educated up to primary school level, 9.84% studied up to secondary school level while only 0.32% patients were graduate. Similar results had been observed in a study by Dulhani et al where majority of the patients belonged to illiterate class (38.30%), 30.50% were educated up to primary school, 21.35% had received secondary education, while 9.8% had attended college [18].
Majority of the seropositive patients were labourers by occupation (64.86%) in our study. Similar results were observed in studies by Dutt R, et al. [5], Singh A, et al. [7], Kumar R, et al. [19].
Conclusion
People with high risk behavior and the spouse of the affected couple need to be educated for primary and secondary prevention of the disease.
ICTC being the first interface between person willing to get tested and the public health system bridges the gap between the vulnerable population and the health services.
Most of the seropositive patients were males implying that males tend to seek health care more frequently than females. Since most of them were married, they serve as a link between high risk groups and general population. Females are likely to acquire infection from their husbands.
There are quite a number of potential reasons for an increase in the HIV positive population aged 50 years and older. Increased coverage of Antiretroviral Therapy (ART) has allowed people to live well beyond the age of 50 years. This, in conjunction with the declining rates of new HIV infections among younger adults, has reduced the proportion of people living with HIV in the younger adult age groups. Whether HIV incidence is also increasing among the older age group requires additional research [8].
Most patients belonged to rural areas, were illiterate and labourers by occupation, hence the need to spread awareness and improve literacy rate among them. Most common route of transmission was the sexual route, hence the need to emphasize on barrier methods and strengthen Information, Education, Communication (IEC) and Behaviour Change Communication (BCC).
References
- Dash M, Padhi S, Sahu S, Mohanty I, Panda P, et al. (2013) HIV counseling and testing in a tertiary care hospital in Ganjam district, Odisha, India. J Postgrad Med 59: 110-114.
- Sacchidanand S, Oberai C, Inamadar AC (2015) IADVL Textbook of Dermatology (4th edn.). Bhalani Publishing House, chapter 92, pp: 2945-2961.
- Kumawat S, Kochar A, Sirohi P, Garhwal J (2016) Socio-demographic and clinical profile of HIV/AIDS patients in HAART era at a tertiary care hospital in North-West Rajasthan, India. Int J Community Med Public Health 3: 2088-2093.
- (2018) HIV Facts & Figures [Internet]. National AIDS Control Organization.
- Dutt R, Chaudhuri S, Goswami S (2017) Profile of HIV positive clients: an ICTC record based retrospective study. Int J Community Med Public Health 4: 3018-3021.
- (2017) India HIV Estimations 2017 fact sheets. GOI/NACO/MES/HIV Estimations 2017/100818.
- Singh A, Mahajan S, Singh T, Deepti SS (2018) Socio-demographic and clinical profile of HIV/AIDS patients attending the ART centre of Amritsar, Punjab. Int J Community Med Public Health 5: 2059-2065.
- Mahy M, Autenrieth CS, Stanecki K, Wynd S (2014) Increasing trends in HIV prevalence among people aged 50 years and older: evidence from estimates and survey data. AIDS 28: S453-S459.
- Ahuja S, Pandey A, Vishkarma R, Madan M (2016) Profile of HIV positive clients attending an integrated counselling and testing centre of a tertiary care hospital in Meerut, Uttar Pradesh, India. Int J Curr Microbiol App Sci 5: 384-391.
- Haider S, Kumar V, Singh SB, Sunderam S (2015) A study on socio-demographic profile and CD4 count of HIV infected patients attending ART centre RIMS, Ranchi. Heal J 6: 12-17.
- Deshpande JD, Giri PA, Phalke DB (2012) Clinico-epidemiological profile of HIV patients attending ART centre in rural Western Maharashtra, India. South East Asia J Public Health 2: 16-21.
- Sonani HP, Undhad AM, Savani GT (2011) Clinical and socio-demographic profile of patients registered at ART centre, Smimer, Surat. Natl J Community Med 2: 130-132.
- Toshniwal H, Modi K, Talsania N, Shevkani M, Shah V, Sengal V, et al. (2013) Clinico-epidemiological and socio-demographic profile of HIV positive patients, visiting clinic in Ahmedabad, Gujarat, India. Int J Health Sci Res 3: 77-84.
- Kumari R, Kumar M, Mohapatra SC (2017) Clinico-demographic profile of HIV patients at ART centre of a tertiary care referral hospital in North India. Int J Community Med Public Health 4: 3166- 3173.
- Nayak UB, Lenka S, Achappa B (2015) Clinical and Socio demographic profile of attendees at ART centre in a tertiary care hospital in Mangalore, India. Asia J Med Sci 6: 61-65.
- Vaseem BN, Madhusudan S, Bhardwaj AK, Rathore M, Kasyap A (2012) A study on socio-demographic profile and risk factors present in HIV infected patients attending art centre in tertiary care hospital in Rajasthan, India. Natl J Community Med 3: 339-343.
- Joge US, Deo DS, Lakde RN, Choudhari SG, Malkar VR, et al. (2012) Sociodemographic and clinical profile of HIV/AIDS patients visiting to ART Centre at a rural tertiary care hospital in Maharashtra state of India. Int J Biol Med Res 3: 1568-1572.
- Dulhani NK, Khan Y (2018) Sociodemographic and immunological profile of human immunodeficiency virus patients in tribal population. J Integr Health Sci 6:14-17.
- Kumar R, Rao DN (2013) Clinico-epidemiological profile of HIV positive patients on anti retroviral treatment at VIMS, Bellary, Karnataka. J Evol Med Dent Sci 2: 23-28.