Research Article
Expert Opinion on the use of Bisoprolol-Telmisartan Combination in Indian Patients with Hypertension
Manjula S*and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Corresponding author: Manjula S, Department of Medical Services, Micro Labs Limited, 31 Race Course Road, Bangalore, Karnataka, India- 560001 Email Id:drmanjulas@gmail.com
Copyright: ©2024 Manjula S, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 20/12/2023; Accepted: 16/01/2024; Published: 19/01/2024
Abstract
Background:The combination of bisoprolol and telmisartan has been recognized as a viable treatment option for hypertension management in India. However, there was a dearth of information available on the preference of antihypertensives in the actual clinical practice among clinicians.
Objective:To assess the prescription pattern of antihypertensive medications and evaluate the real-world practice of bisoprolol + telmisartan combination therapy for hypertension management in the Indian context.
Methodology: A cross-sectional, multiple-response questionnaire-based survey was conducted among clinicians with expertise in treating hypertension. The survey consisted of 25 items and focused on the prescription practices of antihypertensive medications, as well as the utilization of bisoprolol + telmisartan combination therapy for hypertension treatment. Descriptive statistics were used to analyze the data, and categorical variables were represented as percentages.
Results: The study analyzed the responses of 647 participants. It was found that 47% of the respondents followed the American Hypertension Guidelines for hypertension management. Telmisartan was the preferred choice of angiotensin receptor blocker for approximately 95% of the respondents. Among the participants, 73% favored bisoprolol as the beta-blocker of choice for newly diagnosed hypertension patients, and 57% preferred a dosage of 5 mg for patients at risk for cardiovascular disease. Furthermore, 44% of the respondents believed that 20-40% of hypertension patients required a dual antihypertensive drug combination. Nearly 70% of the participants reported improvements in organ function, specifically in target organs affected by hypertension such as the heart, kidneys, and blood vessels, when using the bisoprolol + telmisartan combination.
Conclusion: It was observed that telmisartan was the preferred choice as an angiotensin receptor blocker, while bisoprolol was favored as the beta-blocker for newly diagnosed hypertension patients. The combination of bisoprolol + telmisartan has been shown to be effective in managing hypertension, reducing cardiovascular risk, and improving organ function
Objective:To assess the prescription pattern of antihypertensive medications and evaluate the real-world practice of bisoprolol + telmisartan combination therapy for hypertension management in the Indian context.
Methodology: A cross-sectional, multiple-response questionnaire-based survey was conducted among clinicians with expertise in treating hypertension. The survey consisted of 25 items and focused on the prescription practices of antihypertensive medications, as well as the utilization of bisoprolol + telmisartan combination therapy for hypertension treatment. Descriptive statistics were used to analyze the data, and categorical variables were represented as percentages.
Results: The study analyzed the responses of 647 participants. It was found that 47% of the respondents followed the American Hypertension Guidelines for hypertension management. Telmisartan was the preferred choice of angiotensin receptor blocker for approximately 95% of the respondents. Among the participants, 73% favored bisoprolol as the beta-blocker of choice for newly diagnosed hypertension patients, and 57% preferred a dosage of 5 mg for patients at risk for cardiovascular disease. Furthermore, 44% of the respondents believed that 20-40% of hypertension patients required a dual antihypertensive drug combination. Nearly 70% of the participants reported improvements in organ function, specifically in target organs affected by hypertension such as the heart, kidneys, and blood vessels, when using the bisoprolol + telmisartan combination.
Conclusion: It was observed that telmisartan was the preferred choice as an angiotensin receptor blocker, while bisoprolol was favored as the beta-blocker for newly diagnosed hypertension patients. The combination of bisoprolol + telmisartan has been shown to be effective in managing hypertension, reducing cardiovascular risk, and improving organ function
Keywords:Bisoprolol; Telmisartan; Hypertension; Blood Pressure; Antihypertensive Treatment
Introduction
Of the 1.28 billion people with hypertension worldwide, twothirds
are from low- and middle-income countries and they range
in age from 30 to 79. The reduction of hypertension prevalence by
33% between 2010 and 2030 is one of the global targets for noncommunicable
diseases [1]. Office blood pressure (BP) values of at
least 130 mm Hg systolic and 80 mm Hg diastolic were considered to
be indicative of hypertension, while 24-hour ambulatory BP readings
were 125 mm Hg systolic and 75 mm Hg, respectively [2].For the
optimal management of patients over 65 years of age, the most recent
European and US Guidelines recommend targeting systolic blood
pressure (SBP) between 120 and 130 mmHg, and diastolic blood
pressure (DBP) between 70 and 80 mmHg [2]. Around 46% of adults
with hypertension were unaware of their condition, indicating a lack
of awareness. Additionally, less than half (42%) of adults diagnosed
with hypertension received appropriate diagnosis and treatment.
Moreover, approximately 1 in 5 adults (21%) with hypertension
successfully managed to keep their BP under control [1].
According to Indian guidelines on hypertension-IV, the
diagnosis of hypertension in India was based on office BP reaching
140/90 mm Hg, and ambulatory BP exceeding 130/80 mm Hg [3].
It was undiagnosed or untreated hypertension that increases the risk
of death or lifelong disability and it was a stand-alone risk factor for
myocardial infarction, stroke, chronic renal disease, and coronary
heart disease [4]. However, hypertension remained a modifiable
risk factor, and both non-pharmacological and pharmaceutical
interventions can effectively reduce the associated risks. Therefore,
regular monitoring of BP was crucial for the diagnosis and
management of hypertension [5]. Ambulatory BP monitoring
(ABPM) enabled automatic measurement of the diurnal variation in
BP as well as continuous therapy efficacy assessment [6].The longterm
prognosis was improved by ABPM’s accurate prediction of
cardiovascular (CV) risk and ability to manage BP during the times
of increased risk [7].
Beta-blockers, angiotensin II receptor blockers (ARBs),
angiotensin-converting enzyme inhibitors (ACEi), calcium channel
blockers, and diuretics (including thiazides and thiazide-like
diuretics) are the five medication classes currently used for the
management of hypertension [8]. Studies have revealed that up to
75% of patients treated with a single antihypertensive medication
experience inadequate BP management [9].Fixed-dose combination
was recommended by the majority of hypertension management
guidelines, as it helps to improve patient compliance and convenience
while achieving better BP control [10-12].The combination therapy of
bisoprolol + telmisartan has been recognized as a viable treatment
option for hypertension management in India. Bisoprolol, a betablocker,
and telmisartan, an angiotensin II receptor blocker, have
complementary mechanisms of action that can effectively lower
BP. Bisoprolol acts by reducing heart rate and contractility, whereas
telmisartan works by blocking the effects of angiotensin II, resulting
in vasodilation and decreased fluid retention. By combining these two
medications, clinicians can target multiple pathways involved in BP
regulation, leading to improved control of hypertension [13].
The present study was intended to evaluate the prescription
pattern of antihypertensive medications and the real-world practice
of bisoprolol + telmisartan combination therapy for hypertension
management in the Indian context.
Methodology
A cross sectional, questionnaire based survey was carried out
among clinicians with expertise in treating hypertension in the major
Indian cities from June 2022 to December 2022.
Questionnaire:
The questionnaire booklet titled HEART (The Experts Opinion
on HypertEnsion And its TReatmenT) study was sent to the
physicians who were interested to participate in the study. The
HEART study questionnaire included questions on the current
practices, preferences, clinical observations, and experiences related
to the use of antihypertensives in routine settings, particularly
bisoprolol + telmisartan for the management of hypertension. The
study was conducted after receiving approval from Bangalore Ethics,
an Independent Ethics Committee which was recognized by the
Indian Regulatory Authority, Drug Controller General of India.Participants:
An invitation was sent to leading clinicians in managing
hypertension in the month of March 2022 for participation in this
Indian survey. 647 doctors from major cities of all Indian states
representing the geographical distribution shared their willingness
to participate and provide necessary data. Physicians were asked to
complete the questionnaire without discussing with peers. A written
informed consent was obtained from each physician prior initiation
of the study.Statistical Analysis:
The data were analyzed using descriptive statistics and percentage
was used to represent categorical variables. In order to represent
each variable’s distribution, we used a frequency distribution and a
percentage distribution. Using Excel 2013 (16.0.13901.20400), pie
and bar charts were made.Results
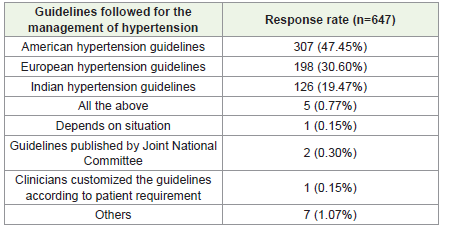
The study analyzed the responses of 647 participants. Analysis of
data on clinicians’ compliance with guidelines for the management
of hypertension revealed that 47% of the respondents followed the
American Hypertension Guidelines, while 31% of the respondents
adhered to the European Hypertension Guidelines. Indian
Hypertension Guidelines were followed by 19% of the respondents.
Combining recommendations from multiple sources or considering
the overall consensus (0.77%) was performed by a small proportion
of clinicians[Table 1].
Diabetes was the most common comorbid condition noted in
newly diagnosed hypertensive subjects, as reported by 52% of the
participants. While 32% of the respondents reported dyslipidemia
as a commonly noted comorbid condition, 9% of them observed
chronic kidney disease and only 5.5% highlighted hypothyroidism.
Furthermore, the majority of respondents (87.32%) agreed that aortic
stiffness and pulse wave velocity are newer indices that can be used to
assess uncontrolled hypertension and CV risk but 5% of them denied
it and 6% of physicians require more data to support it.
Majority of respondents (71.40%) preferred the prescription of
once-daily anti-hypertensive medications in the morning. On the
other hand, approximately 25% of the clinicians preferred prescribing
the medication in the evening. Regarding the use of dual combination
antihypertensive medications, a significant percentage of respondents
(44.2%) noted that 20-40% of hypertensive patients would require
such a combination. Nearly 40% of the respondents estimated that 10-
20% of hypertensive patients would benefit from a dual combination,
while approximately 13% believed that <10% of hypertensive patients
would require this type of combination therapy. Around 47% of the
respondents believed that 25-50% of newly diagnosed hypertensive
patients achieve BP control within the first year of treatment using
monotherapy, while 41% of the respondents noted only <25% and
8.34% of them observed 50-75% reduction in BP.
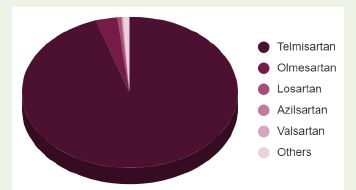
The findings on the commonly preferred angiotensin receptor
blockers (ARBs) showed that around 95% of the respondents
expressed a preference for telmisartan as the ARB of choice. A
small percentage of respondents (3.24%) indicated a preference for
olmesartan as the ARB alternative [Figure 1].
Approximately 73% expressed a preference for bisoprolol as the
beta-blocker of choice for newly diagnosed hypertensive patients,
while 21% indicated a preference for metoprolol. A small percentage
of respondents (5.10%) preferred carvedilol as the beta-blocker for
newly diagnosed hypertensive patients [Table 12].
Out of 647 respondents, 72% identified the high beta-1 selectivity
of bisoprolol as one of its advantages. Approximately 16% recognized
that bisoprolol’s ability to reduce heart rate and cardiac output
contributes to its antihypertensive properties and 6% of clinicians
observed all such effects. A smaller proportion of respondents
(3.70%) indicated that bisoprolol has a minimal impact on libido.
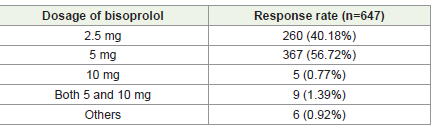
Around 57% of the clinicians selected 5 mg as the preferred dosage for
bisoprolol in hypertensive patients with CV risk, while 40% indicated
that a dosage of 2.5 mg of bisoprolol might be appropriate [Table 3].
A major proportion of respondents (71%) indicated that they
encounter patients who have both hypertension and CV disease,
whereas 16% reported encountering patients with uncontrolled
hypertension and nearly 6% of them preferred in younger patients
with hypertension. Approximately 55% noted that patients between
the ages of 40 and 50 years are typically diagnosed with hypertension.
While around 32% reported encountering patients under the age
of 40 with newly diagnosed hypertension. A smaller percentage of

respondents (10.97%) reported managing patients between the ages
of 50 and 60 years.
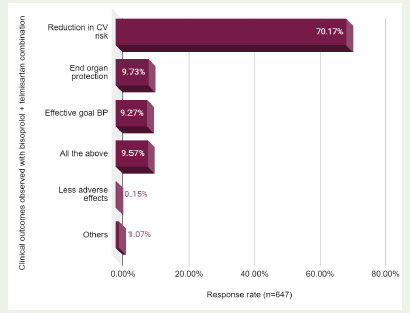
Approximately 70% reported a reduction in CV risk in patients
receiving the bisoprolol + telmisartan combination. Additionally,
10% observed that the treatment confers end-organ protection,
particularly in target organs affected by hypertension such as the
heart, kidneys, and blood vessels. Furthermore, 9% of respondents
reported achieving effective BP control in patients treated with the
bisoprolol + telmisartan combination. Lastly, 10% indicated that they
observed multiple positive outcomes with the bisoprolol + telmisartan
combination including a reduction in CV risk, end-organ protection,
and effective goal BP control [Figure 2].
Discussion
The current study emphasized the importance of medication
adherence as a critical factor in achieving successful therapeutic
outcomes for hypertensive patients. By providing individualized
treatment options, it was possible to maximize the therapeutic effects
and improve patient satisfaction in controlling hypertension. To
enhance adherence and maximize treatment effectiveness, simplifying
treatment algorithms and favoring single-pill combinations can be
employed to attain BP goals [13]. The most recent revision of the
European Society of Cardiology/European Society of Hypertension
guidelines for the diagnosis and treatment of hypertension
recommend streamlined drug treatment algorithms. The preferred
approach involves using an ACEi or ARB combined with a calcium channel
blocker and/or a thiazide/thiazide-like diuretic as the core
treatment strategy for most patients. This strategy was based on
evidence demonstrating the ability of these medication classes to
reduce CV events and improve patients’ prognoses [9].
The current data also highlighted the diversity in guideline
adherence among clinicians participating in the study, with a
significant number following either the American or European
Hypertension Guidelines. The inclusion of the Indian Hypertension
Guidelines as another notable reference demonstrated the global
variation in hypertension management practices. The presence of a
small proportion combining recommendations from multiple sources
indicated potential flexibility and open-mindedness in incorporating
different guidelines.
The European Society of Cardiology/European Society of
Hypertension Guidelines and the American Heart Association/
American College of Cardiology 2017 guidelines emphasized the
important role of beta-blockers in the management of hypertension
[2]. The majority of respondents in the current study expressed
a preference for bisoprolol as the beta-blocker of choice for newly
diagnosed hypertensive patients, while a significant percentage
indicated a preference for metoprolol. The recommended dosages
of bisoprolol identified by the respondents were 5 mg and 2.5 mg,
which are considered appropriate for hypertensive patients with CV
risk. Bisoprolol’s selectivity for beta-1 adrenergic receptors, primarily
found in the heart, was believed to contribute to its effectiveness in
reducing heart rate and blood pressure. This selectivity allowed it to
target specific receptors, potentially leading to better outcomes [14].
The respondents also recognized the effectiveness of bisoprolol
in reducing heart rate and cardiac output, which contributes to
its antihypertensive properties [15]. Carvedilol, a non-selective
beta-blocker with additional alpha-blocking properties, was often
prescribed for specific indications such as heart failure. It was worth
noting that other beta-blockers, including metoprolol and bisoprolol,
were widely used in various European countries and were considered
safe during pregnancy [16]. A significant percentage of the current
respondents indicated that 20-40% of hypertensive patients require
a dual combination of antihypertensive medications. The percentage
of patients requiring dual combination therapy can vary based on
several factors. Disease severity, the presence of comorbidities,
individual patient characteristics, and treatment guidelines all play
a role in determining the appropriate treatment approach. Many
hypertension management guidelines recommended initiating
antihypertensive therapy with a medication combination, preferably
in the form of a fixed-dose combination. This approach offered
several advantages, including convenience for patients and improved
medication adherence [9,12].
In the current study, the majority of the respondents favored
telmisartan as the preferred ARB in the management of hypertension.
Telmisartan has been shown to have several advantages compared to
other antihypertensive drugs. It has greater tolerability and fewer
side effects, making it a favorable choice for many patients [17].
The findings from the another trial further support the efficacy of
telmisartan in controlling the morning increase in blood pressure,
which was a significant concern for hypertensive individuals [18].
Additionally, Gosse et al. demonstrated that telmisartan 80 mg was
superior to ramipril 10 mg in lowering early morning mean systolic
and diastolic blood pressure compared to baseline measurements[19].
This suggested that telmisartan can effectively reduce blood pressure
levels, especially during critical periods such as the early morning.
One notable aspect contributing to the superiority of telmisartan was
its longer half-life of approximately 24 hours. This extended duration
of action allows for sustained blood pressure control throughout the
day, enhancing its effectiveness compared to other drugs with shorter
half-lives[20].
Despite the widespread preference for telmisartan, a small
percentage of respondents in the study expressed a preference
for olmesartan as an alternative ARB. Nakayama et al. found that
olmesartan significantly reduced mean systolic and diastolic blood
pressure compared to telmisartan after 8 weeks of treatment [21]. The
preference for olmesartan by a subset of respondents indicated the
need for individualized treatment approaches and consideration of
alternative ARBs based on patient-specific factors.
As per the recent updates on hypertension management, the
combination of the beta blocker, bisoprolol and the ARB, telmisartan
has garnered attention. According to the majority of respondents
in the current study, the bisoprolol + telmisartan combination
demonstrated a reduction in CV risk [22,23]. Furthermore, a notable
percentage of respondents reported observing end-organ protection,
indicating that the combination therapy preserved and improved
organ function, especially in target organs affected by hypertension,
such as the heart, kidneys, and blood vessels. Additionally, a small
proportion of respondents mentioned achieving effective BP control
with the bisoprolol + telmisartan combination, indicating its efficacy
in helping patients reach their target BP levels.
Sawhney et al. conducted a study in Indian settings and
highlighted the combination of bisoprolol + telmisartan as a valuable
treatment approach for patients with concomitant hypertension[23].
The authors observed that the use of bisoprolol had significant clinical
implications in various patient populations, including those with left
ventricular dysfunction post myocardial infarction, coronary artery
disease, hemodialysis, and heart failure. Bisoprolol demonstrated its
effectiveness by modulating resting heart rate in these conditions.
On the other hand, telmisartan was found to provide a distinct
pharmacological approach to the management of hypertension.
Its unique properties made it a valuable tool for controlling blood
pressure and addressing hypertension-related issues[23].
The multicentric, double-blind, parallel-group, comparative,
prospective, phase-III clinical study established the efficacy,
tolerability, and safety of the fixed dose combination tablet of
Telmisartan 40 mg + Bisoprolol 5mg tablets for the management
of stage 1 and stage 2 hypertension[24]. The mean change in SeSBP
and SeDBP at weeks 2/6/12 as compared to the prior visit was
statistically significant (p<0.001) in all cases (i.e., baseline to week 2,
week 2 to week 6, and week 6 to week 12) in both test and control
arms. The mean difference in SeSBP from baseline to study end was
significantly higher in Telmisartan 40 mg + Bisoprolol 5mg than the
Telmisartan 40 mg + Metoprolol Succinate ER 50 mg (p = 0.029).
Rated as ‘excellent’ by 93.75% subjects in test arm and 91.40%
subjects in control arm. This study showed that Telmisartan 40 mg +
Bisoprolol 5mg combination was non-inferior to Telmisartan 40 mg
+ Metoprolol Succinate ER 50 mg and was significantly superior with
respect to a few end points [24].
Telmisartan’s long-lasting blood pressure-lowering effects and
cardioprotective properties is due to its strongest AT1 receptor
antagonistic ability and corresponding slower dissociation from the
receptor. Several Landmark trials (ONTARGET, TRANSCEND,
DETAIL, AMADEO, VIVALDI etc.) have shown the effectiveness of
Telmisartan in the management of Hypertension. The 2019 Indian
hypertension-IV guideline recommends telmisartan as one of
the drugs of choice to treat hypertension [25]. The BRIGHT study
has shown the effectiveness of Bisoprolol in Indian patients with
Hypertension [26]. The BISOCAD study [27], CREATIVE study [28] have shown that Bisoprolol is superior in dynamic HR reduction and
BP reduction than Metoprolol.
Further to the Phase III study, the present study offers valuable
expert opinions on the clinical use of this combination therapy.
This contributes to the existing body of knowledge supporting
the effectiveness of bisoprolol + telmisartan in helping patients
manage their hypertension and achieve their BP targets. The study’s
strength and significance in the field of hypertension research and
clinical practice are further enhanced by its rigorous methodology,
providing reliable and accurate insights. Moreover, the emphasis on
individualized therapy in the study adds value by recognizing the
importance of tailoring treatment approaches to meet the specific
needs of patients.
One major drawback of the current study was its small sample
size, which may limit the generalizability of the findings to a
larger population of hypertensive individuals. A larger and more
representative sample would provide a more accurate understanding
of the topic. Additionally, the study’s reliance on expert judgment
introduces the possibility of bias, as various perspectives and
preferences might have influenced the reported results. It was
important to consider these limitations when interpreting the
findings and to conduct further research to confirm and expand upon
the conclusions.
Conclusion
It was found that telmisartan was the preferred ARB and bisoprolol
was the favored beta-blocker for newly diagnosed hypertension
patients. Combining bisoprolol + telmisartan has demonstrated
effectiveness in the management of hypertension, along with benefits
such as reducing cardiovascular risk and improving organ function.
Acknowledgement
We would like to thank all the clinicians who were participated
in this study.
References
Citation
Manjula S, Krishna Kumar M. Expert Opinion on the use of Bisoprolol-Telmisartan Combination in Indian Patients with Hypertension. Indian J Cardio Biol Clin Sci. 2024;7(1): 113.