Review Article
Integration of Emerging Technologies: Management of Cardiometabolic Diseases
Rao GH*
Lillehei Heart Institute, University of Minnesota, USA
Corresponding author: Rao GH, Laboratory Medicine and Pathology Director, Thrombosis Research, Lillehei Heart Institute, University of Minnesota, USA, E-mail: gundurao9@gmail.com
Citation: Rao GH. Integration of Emerging Technologies: Management of Cardiometabolic Diseases. Indian J Cardio Biol Clin Sci. 2018;5(1): 111.
Copyright © 2018 Rao GH. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Cardio Biology & Clinical Sciences | Volume: 5, Issue: 1
Submission: 26/11/2018; Accepted: 27/12/2018; Published: 29/12/2018
Abstract
Future of global healthcare depends heavily on the intelligent (smart), integration of emerging technologies, and development of seamless, diagnosis, management, and prevention capabilities. This dream will not come true, by allotting several billion dollars on a single project like, the “All of Us”, a Personalized Genome Project, of the National Institutes of Health, USA, or by providing millions of dollars, to top few Universities (Harvard, MIT, Oxford, Cambridge etc.,) of the world, or putting together several Noble laureates, on the Board (Elysium Health) of a company. It can come only, by developing well thought-out projects, with a team of talented, dedicated workers, with a multidisciplinary approach. Whenever a new scientific discovery is announced, it is usually followed by great hype, and lots of expectations, about the immediate benefits of such a discovery or innovation. Take for instance, the discovery and elucidation of the structure of DNA, announcement of gene therapy applications, tissue regeneration applications, contributions of big data, evolution of cloud technologies, revolutions in IT applications, and the promises that these innovations have made, in solving issues related to global health. Some of these applications have taken a top-down approach and have attained partial success (IBM-Watson Oncology), and some others, have failed after spending billions of dollars (NHS-Country level IT-enabled electronic health records system). All major discoveries, take time to develop to their full potential. Having said that, some innovations which took bottom-up approach, have been quite successful. Just to name a few biotechnology applications in the development of diagnostics and cellular and molecular therapeutics, have gained rapid success. If one studies the life, success and achievements of renowned scientist like, Stephen Hawking, one can realize, how the need-based research, can deliver unique applications, such as mind-computer interfaces, which helped him achieve the ability to communicate in a unique way. In this overview, we have not tried to solve all the problems, or provide unique solutions; we have made a humble attempt to illustrate, that one can develop novel diagnostic, management, predictive, and preventive platform, using existing data systems, and integrate emerging technologies to such platforms. We also recommend that such platforms, which use proprietary algorithms to develop clinical data, should develop evidence-based, independently validated clinical data, to support their claims, on risk assessment, management, and prevention.
Introduction
Metabolic disease such as hypertension, excess weight, childhood and adolescent obesity, type-2 diabetes, and vascular diseases have reached epidemic proportions worldwide [1-13]. In the last three decades, obesity has increased by two-fold and diabetes by four-fold [6-9]. During the same period (1980 to present) in China, diabetes has increased by 17-fold [14]. China and India, have the largest diabetic populations, whereas, the USA has highest prevalence of diabetes. This rapid increase in the incidence of diabetes in China is attributed to urbanization, altered lifestyle, sedentary life, and Western pattern diet [10]. Early signs leading to the development of future diabetes can be identified more than 20 years before the diagnosis of diabetes, according to a new research finding, presented at this year’s European Association for the Study of Diabetes (ESAD), Annual Meetings in Berlin, Germany (1-5 October, 2018). The researchers reported, that increase in fasting glucose levels, BMI, and insulin sensitivity, could detect probabilities of developing future diabetes, 10 years prior to the detection of prediabetic state. Since one can have prediabetic state for almost ten years, the researchers claim, that this new approach can detect the predisposal of individuals to diabetes, 20 years ahead of its occurrence. Similarly, new approaches are available to detect probability of developing overweight or obesity, even at the infancy. New data from the University of Colorado suggests, that evaluating the gut microbiota, which has a multitude of health condition and disease states, facilitates the prediction of future obesity [15].
It gives great pleasure for me, to write this invited review and express my view points, on this very important subject of public health interest, in the Journal of Cardio-biology and Clinical Sciences. It is very well recognized now, that all the metabolic diseases, have reached epidemic proportions worldwide. Having said that, it pains me to report, that no country has taken this warning seriously, and developed serious prevention strategies and action plans. As mentioned above, all the participating countries of the United Nations, have signed a declaration, to do their very best to stop these epidemics by 2030. However, according to global experts in this field, chances of stopping, reducing, or reversing these epidemics of chronic diseases by 2030, is very little. What can be done? It is a good question, however considering the rapidity with which these chronic diseases are increasing, we need to develop strategies to reduce, reverse or prevent these metabolic diseases now, not in the future.
I was invited by the Government of India, under a unique United Nation sponsored program called TOKTEN, which stands for Transfer of Knowledge through Expatriate Nationals. I visited India, three years in a row from 1990-93, and spent considerable amount of time in major Medical Institutions. Following these visits, I started a professional society, South Asian Society on Atherosclerosis and Thrombosis (SASAT), in 1993 at the University of Minnesota, USA. I organized conferences in India, every other year, and published several books on this topic of great public health interest [16,17]. Since my retirement, I am spending considerable time in India, trying to put together a non-invasive diagnostic platform, for early diagnosis of the risks for metabolic diseases, and for the effective management of the observed risks. In this review, we will discuss what diagnostic tools are available, what additional tools need to be developed, and how we can integrate these devices and emerging technologies, to improve the management of cardiometabolic diseases.
Medical innovations, advances in emerging technologies, revolution in smart application platforms, cloud computing, big data, artificial intelligence, and internet of things, are not just buzzwords any more. All of these novel approaches are fighting for their niche, in the trillion-dollar healthcare industry. What are these medical innovations; emerging technologies, and how integration of these innovations and technologies, will improve healthcare delivery? Every scientific discovery, advances in technology, has raised expectations about their collective contributions to the human welfare. Especially in the area of health care delivery, they have promised great opportunities for quick cures of fatal diseases, and easy solutions. Since the time, structure and function of the DNA was elucidated, and genetic code cracked by the scientists from Cambridge University and King’s College, London, six decades ago, there is great expectation, that these discoveries will ultimately provide the root cause for all inherited diseases, and help develop potential pathways for cures [18-20]. According to the scientific reports, George Church a pioneer in genome research, a professor at the Harvard Medical School, currently directs the Personal Genome Project (PGP), a longterm cohort study [21]. It is said, that in the near future, your health risks and medical problems may be investigated, and pieced together [21-27].
President Barack Obama announced in the State of the Union (2015) address, “Tonight, I am launching new Precision Medicine Initiative to bring closer to curing diseases like cancer and diabetes and to give all of us access, to the personalized information we need to keep ourselves and our families healthier”. Francis Collins, the Director, National Institutes of Health, USA, writes in his article in the NEJM, “We envisage assembling overtime a longitudinal “cohort” of 1 million or more Americans who have volunteered to participate in research [27-29]. Participants will be asked to give consent for extensive characterization of biologic specimens (cell populations, proteins, metabolites, RNA, and DNA including whole genome sequencing) and behavioral data, all linked to their electronic health records”. According to a report in the British Medical Journal (BMJ 2018:361), “All of Us” study has begun to sequence, and doi: https://doi.org/10.1136/bmj.k2001 follow a million Americans, as a part of a large long-term prospective study on May 6th in seven US cities. Francis Collins, NIH director, called it “a national adventure that is going to transform medical care”
There is great speculation, that Artificial Intelligence (AI), will radically change healthcare in the future [27,30-32]. Some claim, that it is already significantly changing healthcare. IBM-Watson Health, General Manager, Deborah DiSanzo provided an update, on the progress that IBM Watson, - the AI system, famous for beating Jeopardy, - TV-Game show and many Chess competitions worldwide, is making rapid progress in improving healthcare. Roughly 150,000 patients are now managed with the assistance of IBM Watson Care Manger. More than 155 hospitals and healthcare organizations are using IBM Watson Oncology, including the Manipal Hospital system in India. According to Di Sanzo IBM Watson for Oncology “agreed” with the health care systems’ multi-disciplinary tumour board recommended treatment approach, in 93% of 638 breast cancer patients. IBM Watson’s Clinical Trial Matching (CTM) system eliminates the need to manually compare clinical trial enrolment criteria, with patient medical data. Instead, it uses AI to read through all of this data, matching the right patient to the right clinical study. IBM Watson Health and Quest Diagnostics announced the launch of a new service that helps advance precision medicine, by combining cognitive computing with genomic tumour sequencing. The American Heart Association, IBM Watson, and Denver, Colorado based vendor Welltok, are teaming up on the creation of a workplace health solution to improve heart health.
The UK government chose on the other hand, the top-down, government approach: a “nationwide implementing of Electronic Health Records EHR’s, known as the NHS Care Records Services, was the cornerstone of the 12.7 billion national programme, for information technology. In order to bring the process of creating a system, that supports health IT for the entire nation, the UK with the help of four companies, including the US-based company, the Computer Science Corporation, began one of the largest and ambitious health IT projects, that the world had ever seen in early 2002. It was a project that would eliminate the challenges of interoperability, between various competitive EHR systems around the UK. This one of a kind national project came to an end in 2011. In a mini review like this, we do not want to discuss the reasons for the failure of this ambitious project. Instead, let us review what we can do with the available technology. We will begin our discussions with ambulatory diagnostic monitors.
Figure 1 shows a glucose profile of a patient with high HBA1c, whereas, the Figure 2 shows the glucose profile of two different patients with similar HBA1c values. Note that the sensor monitors interstitial glucose, every 15 minutes and computes the average values, and HBA1c values are derived from these glucose values, using proprietary software and analytics. Similar continuous glucose monitoring devices are available from Dexcom, a California based company. Dexcom G6 reads glucose levels every five minutes and special apps provide access to data whenever needed.
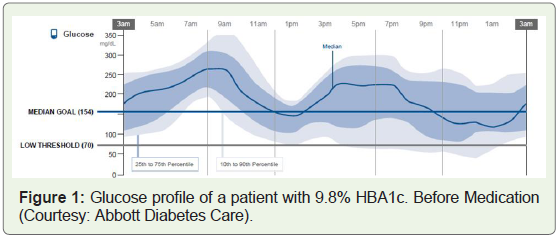
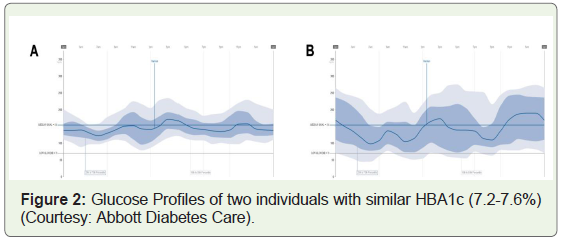
Figure 3 shows the tools used, for obtaining data on cardiometabolic risks and risk clusters. The devices used, provide basic physiological responses, and software analytics compute the risks, which are compared with the clinical data and the values correlated.
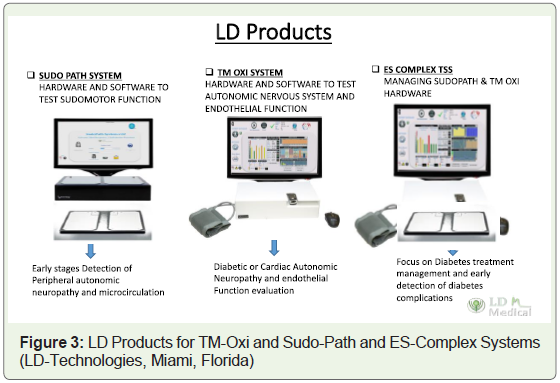
Figure 4 shows improved version of the LD products, which are updated with further improvements, from the older model (Figure 3). Improvements include, use of emerging technologies and superior sensors. The details of the methodology and results are provided in discussion section.

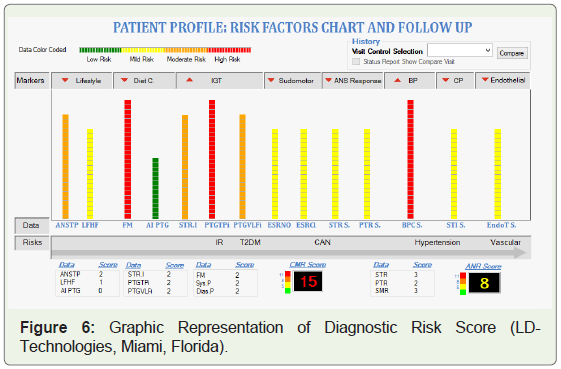
Figure 5 summarizes a typical patient data; individual risks are digitized, and color coded and final Cardiometabolic Risk Score (CMR), and Autonomous Nervous System (ANS), risk are computed from the data obtained by various tests.
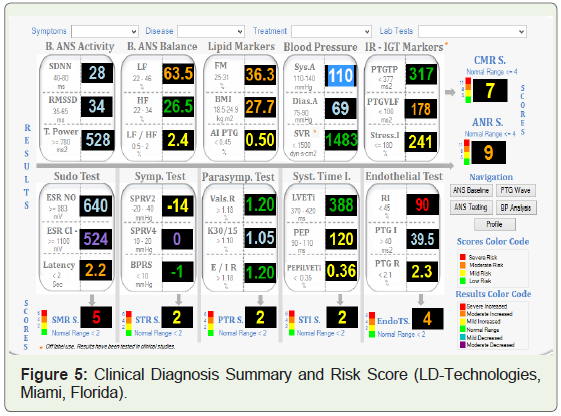
Figure 6 summarizes a typical patient data, and presents the risks in bar graphs. Like the previous summary, the data are color coded from green to red, representing graded risk from normal to high risk.
The device monitors pulse wave forms, and computes endothelial dysfunction, using sensitive pressure sensors. The University of Minnesota uses this device, for CVD risk profiling (Figure 7).
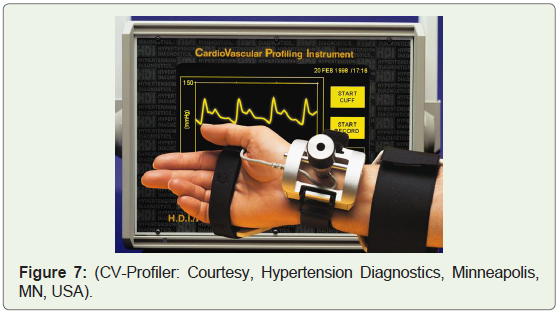
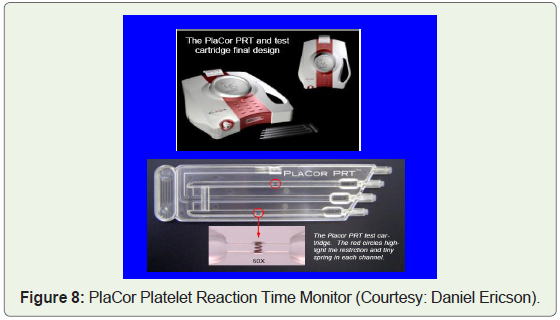
Figure 8 shows a set-up, used at the University of Minnesota, to monitor platelet reaction time, using uncoagulated fresh blood from a finger stick. Uses a disposable cassette to initiate flow, and generate the needed shear force, to promote clotting of the circulating blood.
Discussion
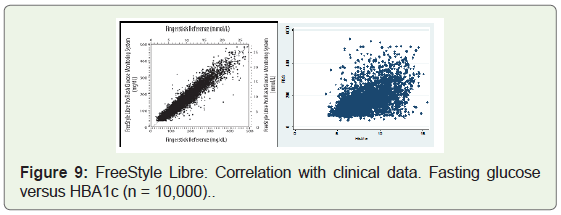
The US president Barack Obama announced the launch of an ambitious project on “Precision Medicine” during his State of the Union address in January of 2015 [27]. The initiative called “All of Us” envisages, assembling over time, a longitudinal “cohort” of 1 million Americans, who have volunteered, to participate in research. Participants will provide consent, for extensive characterization of biologic specimens (cell population, proteins, metabolites, RNA and DNA- including whole genome analysis). This effort, funded (over a Billion USD) by the National Institutes of Health (NIH), focuses on finding cures to Cancer and Diabetes. What we need to understand, when we think of cancer and diabetes is, that underlying causes for the progress of these diseases and their clinical complications, are very complex and no attempt to develop “one idea fits all” will work. Much simpler projects, other than the ambitious Personal Genome Project, are shaping up in view of the rapid progress in emerging technologies, and the evolution of smart wearable devices. Medical data company Cardiogram claims, that the Apple watch and other smart devices like Fitbit could be used to track signs of diabetes and other diseases. Fitbit has been chosen by the NIH, to be a part of a long-term study called “All of Us” that will examine how life style differences, can affect personal health. The Scripps Translational Science Institute (San Diego, USA), which runs part of the All of US project, will be handling out up to 10,000 Fitbit Charge 2 and Fitbit Alta HR devices, which will be used in the study (Figure 9). Note that, obstructive sleep apnea prevents restful sleep, and is associated with high blood pressure, arrhythmia, stroke, and heart failures. Emerging research highlights the complex interrelationships between sleepdisordered breathing, and cardiovascular disease, presenting clinical research opportunities as well as challenges [33].
When thinking of opportunities and challenges, in developing an integrated diagnostic, predictive, and preventive platform, our emphasis is on building around a well thought out existing noninvasive diagnostic platform. Let us call this Cardiometabolic Risk Profiler (CMRF). We could use the basic platform developed by Dr Albert Maarek of Miami, Florida, under the brand name LD-Products (Figures 4-6). Now let us figure out, how we can add information and develop a personal portal, which would provide, risk analysis, risk prediction and risk management capabilities, including a personal alert system, to provide connectivity between the clinician, diagnostic platform, and the fitness profile. When we think of cardiometabolic diseases, we limit our imagination to just a few known disease entities, such as hypertension, obesity, type-2 diabetes, and vascular diseases. There are many other metabolic risks, some known and some as yet unknown, that add to the list of these chronic metabolic risks. Just to mention a few, oxidative stress, low-grade chronic inflammation, hyper glycaemia, insulin resistance, altered blood flow dynamics, endothelial dysfunction, arterial stiffness (hardening of the arteries), subclinical atherosclerosis, plaque build up, narrowing of the arteries, and other causes that lead to prothrombotic state.
Let us start with the hypertension, as one of the early cardiometabolic risks. Ambulatory Blood Pressure Monitors (ABPM), are available for decades, yet they are not used routinely, even in an advance country like the USA. Hypertension is a major risk, for cardiovascular morbidity and mortality, especially in patients with diabetes. Use of AMBP to manage hypertension, is far superior than, one time check of BP in doctor’s office. Since ABPM has capability to collect, collate, and ‘sync’ data to a computer. This device can be easily integrated with other smart applications. Indeed LDtechnology diagnostic platforms have incorporated automated BP monitor in their data system. Next in the line of early diagnostics, is the ambulatory glucose monitor. Both Abbott Diabetes Care, as well as Dexcom G6 Continuous Glucose Monitoring (CGM) systems, can collect data and ‘sync’ the data to any smart platform such as smart phones, iPad’s or computers, similar to fitness tracking devices such as Apple watch and Fitbit. We emphasize hear, that in fine tuning hyperglycemia management, CGM’s come very handy and this technology like the ABMP, could be incorporated and integrated into existing diagnostic platforms.
A few years ago (2013-2015), the Indian Council of Medical Research (ICMR) funded a research project for developing prototypes of non-invasive glucometer using near-infrared sensors. The patent for this idea was shared by Mr. Anil Antony and I, and the product is under development in Singapore [34-36]. Both this particular device, as well as Abbott and Dexcom device uses sensors to detect glucose. We and others have developed software analytics to obtain values for HBA1c, based on the fasting glucose data. Of course, if we have large enough data on fasting glucose, we can develop a much better correlation, between fasting glucose and HBA1c values.
Karnataka Institute of Endocrinology and Research (KIER), has data on fasting glucose of over 1,00,000 subjects. We are trying to collaborate, with Dr M.A. Shekar the Director, KIER, to analyze this massive data. The data developed by AMBP as well as AGM device, can be sent to the common personal portals, for incorporation and fine tuning, the risk assessment algorithms.
LD-Technologies originally came up with TM Oxi, SudoPath and Es-Complex systems for data generation on various physiological responses. Beauty of this platform is, the ingenious way time-tested FDA approved devices, such as oximeter, blood pressure monitor, and galvanic skin response monitor, are used to generate physiological responses; that are collected, collated, and analyzed by proprietary software, to generate risk scores for cardiometabolic risk, as well as for computing clusters of risks, interpretation of the observed risks, and for offering management options. We have discussed the application of this methodology, for early diagnosis of cardiometabolic risks, and better management of observed risks, in our earlier publications [37-39]. The original system first developed by the LD-technologies, has been further fine- tuned and many more features added in the 2019 version (TM-Flow).
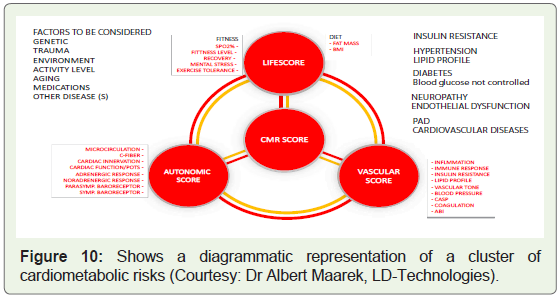
The advanced system presented in Figure 10 and Figure 11, use proprietary software to identify and compute individual risk factors, for cardiometabolic disease as well integrate these test results to develop disease clusters. Furthermore, as presented in Figure 10, show the interrelationship between the Autonomic Risk Score (ANS), Vascular Risk Score (VRS), and Cardiometabolic Risk Score (CMR), which contribute to the overall life score.
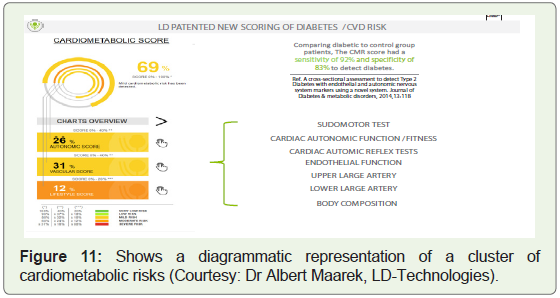
The new scoring system developed by the LD-patented scoring system, for diabetes and its clinical complications, include the test scores for SudoMotor Test, Cardiac Autonomic Function/fitness, Cardiac Autonomic Reflex tests, Endothelial function, Upper Large Artery, Lower Large Artery tests, and data on Body Composition. Based on the results of these tests, the collective Cardiometabolic score is computed (Figure 11). As depicted in Figure 11, the cardiometabolic score is the sum total of autonomic score, vascular score, and lifestyle fitness score. Since this platform already has a well-thought-out risk analysis capability, we have used this to illustrate the possibilities, for the development of a sophisticated integrated personal fitness portal. All of the devices we will discuss in this article, and any other new device available for diagnosis of various risks, can be integrated into such a platform, to fine tune the risk assessment, risk prediction and risk prevention.
Studies from the University of Minnesota, under the leadership of Professor Jay Cohn, a renowned cardiologist, has demonstrated that endothelial dysfunction, is the earliest detectable vascular dysfunction or altered function. We have discussed how the LD-technologies products perform, analyze, and incorporate tests, to determine the vascular dysfunction, in macro as well as micro circulation. We are interested in developing cost-effective, hand-held devices for monitoring altered flow dynamics. According to the manufacturers HD-technology, a low C2-small artery elasticity is an indication of endothelial dysfunction, subclinical atherosclerosis, vascular disease progression and a predictor of cardiovascular events. In spite of the fact, this device has been in use for decades at the University of Minnesota, and few other institutions, it is not used extensively worldwide. We at Bengaluru, India, with the Academia-Industry collaboration, are trying to develop hand-held devices, capable of generating information on blood flow dynamics, altered flow patterns, hardening of the arteries, and subclinical atherosclerosis, using modified ultrasound imaging and pulse waveform analysis technologies. Unlike the clinical devices, these low-cost hand-held devices would be useful for conducting population-based studies. Basically, we are proposing two different approaches, to follow alteration in the flow dynamics of circulating blood [40-47].
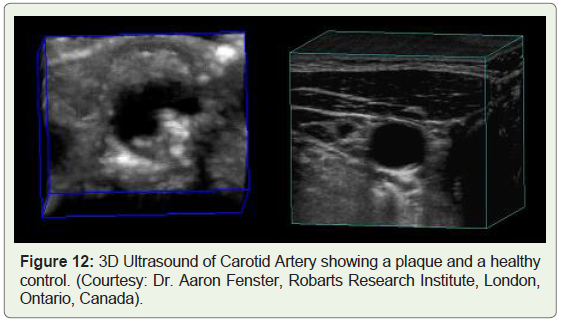
First approach is to use, conventional ultrasound imaging, and develop capabilities to monitor flow patterns in peripheral arteries and veins. The modifications proposed include, calibration of the echo signal, to scan peripheral macro and micro circulation. We also propose to develop software analysis, to convert the 2D images to 3D images (Figure 12), for better quantitation of area and volume of the plaques, or subclinical atherosclerosis. For instance, you can see the advantages of using 3D image as seen in the Figure 12. The images are of the carotid artery serial images, obtained by Dr Aaaron Fenster of the Robarts Research Laboratory, Ontario, Canada. The figure on the left side shows atherosclerotic plaques, as well as narrowing of the carotid artery. The figure on the right side shows, a healthy artery with no visible atherosclerosis. The software analytics will include marking of the area of interest, and calculations for area, as well as for volume determination. Such capabilities help diagnosis, progression, and regression of the atherosclerotic disease [48,49].
Another possibility we are considering, is the use of piezoelectric flexible sensors, to obtain pulse pressure waveforms, as we have demonstrated using LD-Products, wherein, we used Pulse Oximeter to obtain the pulse waveforms. These wave forms were further analyzed by photo plethysmography, to obtain information on macro and micro circulation dysfunctions [37].
When we talk about integration of emerging technologies, we are talking about the development of non-invasive diagnostic platforms, with multiple diagnostic capabilities. For instance, using the same approach as that of Dr. Albert Maarek’s TM-Oxi, and Sudo-Path Systems, and TM-Flow Data Systems (LD -Technologies), we can add to such integrated diagnostic platform, capabilities to monitor glucose, blood flow dynamics, sleeping patterns, alerts about malfunction of systems, and a variety of useful analytics. It will be like a computerized diagnostics system, of an automobile engine performance. For instance, studies are underway, to use sensors on implantable coronary stents, that can monitor changes in the blood flow. Researchers at the University of British Columbia have developed smart stents that can monitor hemodynamic changes in the artery, and warn clinicians of restenosis at its earliest stages. If such sensors on medical implants can relay the real-time data, to a smart platform, then we will know any malfunction of the system immediately. In the near future, technologies will be developed, to follow physiology and function of various organs and systems in realtime, thereby improving our diagnostic capabilities immensely. In a short overview, it is not possible to give details of all the possible applications related to the improvement of clinical studies and integration of emerging technologies for the development of better diagnostics and validation of therapeutic protocols.
Conclusion
In an earlier article, we discussed the importance of monitoring risks, for developing vascular disease. Framingham heart study developed information on the modifiable risks for the development of cardiovascular diseases. Based on the results of their studies, they developed The Framingham Risk Score, a gender-specific algorithm, used to estimate the 10-year cardiovascular risk of an individual. Since that time, researchers and healthcare providers have modified these risk calculators, to fine-tune risk prediction algorithms. In this overview, we have not made any attempts to mimic this or improve this risk assess platform. We have introduced a novel non-invasive diagnostic platform (LD-Products), which can identify a variety of cardiometabolic risks, cluster of risks, and score these risks in terms of the severity of risks. This risk scoring data system depends heavily on the test scores, developed by various sensors and proprietary algorithms, to collect, collate, and calculate the observed alteration in the signals, into clinical risk scores. Since this is an integrated non-invasive diagnostic platform, exclusively built for the diagnosis and management of cardiometabolic risks, we would like to take advantage of this availability, and extend its capability for the diagnosis of various metabolic risks, by adding other smart diagnostic tools with internet connectivity.
We have discussed ambulatory blood pressure monitors, ambulatory glucose monitors, fitness tracking devices, and other uses of sensors, that can be integrated to obtain information on the blood flow dynamics. We hope that the IT experts and device developers, could use these novel approaches, and start integrating emerging smart technologies, into already existing integrated diagnostic platforms, like the one that we have described. Once such capability is developed, then they can further develop “patient data portals”, which can provide useful information, to the patients so that they are empowered to self-manage these complex diseases. As we have seen in the case of Ambulatory Glucose Monitor, patients get highly motivated, when they can see the data on a real time basis on smart Apps and get the ability to manage the glucose levels by anti-glycaemic medications, healthy diet, and life style changes. Since the glucose value can be obtained at the tip of a finger, every five minutes (Dexcom G6), or at every fifteen minutes (Abbott AGM), one can even develop compliment nutritional therapies, by testing the benefits of Amla (Indian Gooseberry) products, Fenugreek products, or mulberry green tea, on postprandial glucose peaks. Since the time, I retired in 2012, I am trying to promote such ideas. India being the IT capital of the World, I hope we can develop such a novel integrated diagnostic platform. Those interested in working this area, can contact me, for further discussions, on this topic of great interest.
References
- Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, et al. (2017) Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990-2015. JAMA 317: 165-182.
- Van Gaal LF, Mertens IL, De Block CE (2006) Mechanisms linking obesity with cardiovascular disease. Nature 444: 875-880.
- GBD 2015 Risk Factors Collaborators (2016) Global, regional, and national comparative risk assessment of 79 behavioral, environmental and occupational, and metabolic risk or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Diseases Study 2015. Lancet 388: 1659-1724.
- Zheng X, Jin C, Liu Y, Zhang J, Zhu Y, et al. (2015) Arterial stiffness as a predictor of clinical hypertension. J Clin Hypertens (Greenwich) 17: 582-591.
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, et al. (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384: 766-781.
- Lu Y, Hajifathalian K, Ezzati M, Woodward M, Rimm EB, et al. (2014) Global Burden of Metabolic mediators of the Risk Factors for Chronic Diseases Collaborations (BMI Mediated Effects): Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis of 97 prospective cohorts with 1•8 million participants. Lancet 383: 970-983.
- Zimmet P, Magliano D, Matsuzawa Y, Alberti G, Shaw J (2005) The metabolic syndrome: a global public health problem and a new definition. J Atheroscler Thromb 12: 295-300.
- World Health Organization (2016) Global report on diabetes. pp: 88.
- NCD Risk Factor Collaboration (NCD-RisC) (2016) Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 387: 1513-1530.
- Mohan V, Rao GH (2007) Type-2 diabetes in South Asians: Epidemiology, Risk factors, and Prevention. JP Medical Publishers India pp: 400.
- Rao GH, VJ Kakkar (1999) Coronary Artery Disease in South Asians. JP Medical Publishers, New Delhi, India.
- Rao GH, Thanikachalam S (2005) Coronary Artery Disease. JP Medical Publishers India pp: 428.
- Rao GH (2016) Coronary Artery Disease. MacMillan Medical Communications/ Springer/Nature. New Delhi.
- Shen X, Vaidya A, Wu S, Gao X (2016) The diabetes epidemic in China: An integrated review of National Surveys. Endocr Pract 22: 1119-1129.
- Stanislawski MA, Dabelea D, Wagner BD, Iszatt N, Dahl C, et al. (2018) Gut microbiota in the first 2 years of life and the association with Body Mass Index at age 12 in a Norwegian Birth Cohort. mBio 9.
- Gundu Hirisave Rama Rao: Wikipedia.
- Rao GH (2016) Contributions of the South Asian Society on Atherosclerosis and Thrombosis and the Indian Society for Atherosclerosis Research, to our understanding of Atherosclerosis and Thrombosis. J Clin Prev Cardiol 5: 67-72.
- Watson JD, Crick FH (1953) Molecular structure of nucleic acids; a structure for deoxyribose nucleic acid. Nature 171: 737-738.
- Wilkins MH, Stokes AR, Wilson HR (1953) Molecular structure of Nucleic acids: Molecular structure of Deoxypentose nucleic acids. Nature 171: 738-740.
- Wilkins G (2013) DNA: Twin strands solved the structure. Nature 496: 434.
- Lunshof JE, Bobe J, Aach J, Angrist M, Thakuria JV, et al. (2010) Personal genomes in progress: from the human genome project to the personal genome project. Dialogues Clin Neurosci 12: 47-60.
- Khan S, Ullah MW, Siddique R, Nabi G, Manan S, et al. (2016) Role of recombinant DNA technology to improve life. Int J Genomics 2016: 2405954.
- Lomedico PT (1982) Use of recombinant DNA technology to program eukaryotic cells to synthesize rat proinsulin: a rapid expression assay for cloned gens. Proc Natl Acad Sci U S A 79: 5798-5802.
- Ginn SL, Alexander IE, Edelstein ML, Abedi MR, Wixon J (2013) Gene therapy clinical trials worldwide to 2012 - an update. J Gene Med 15: 65-77.
- Pennisi E (2013) The CRISPR craze. Science 341: 833-836.
- Misra A (2010) Challenges in delivery of therapeutic genomics and proteomics (1st edn.). Elsevier.
- Collins FS, Varmus H (2015) A new initiative on precision medicine. N Engl J Med 372: 793-795.
- Collins F, Gottileb S (2018) The next phase of human gene-therapy oversight. N Engl J Med 379: 1393-1395.
- Feero WG, Guttmacher AE, Collins FS (2010) Genomic medicine--An update primer. N Engl J Med 362: 2001-2011.
- Jiang F, Jiang Y, Zhi H, Dong Y, Li H, et al. Artificial intelligence in healthcare: past, present, and future. Stroke Vasc Neurol 2: 230-243.
- Murdoch TB, Detsky AS (2013) The inevitable application of big data to health care. JAMA 309: 1351-1352.
- Pearson T (2011) How to replicate Watson hardware and systems design for your own use in your basement.
- Drager LF, McEvoy RD, Barbe F, Lorenzi-Filho G, Redline S (2017) Sleep apnea and cardiovascular disease: Lessons from recent trials and need for team science. Circulation 136: 1840-1850.
- Antony Aneel Joseph and Gundu Hirisave Rama Rao: Patent Application. July 9, 2013. 2756/CHE/2012A. International classification A61B5/00.
- Rao GH (2014) Development of prototype of Non Invasive Glucometer using NIR Spectrometry. DOS 1-6-2013 to Dec 2014. Indian Council of Medical Research (ICMR).
- Chandrasekhara BG, Rao GH (2015) Wireless Smartphone-based Non-Invasive Glucometer. US Provisional Patent EFS ID: 22908511, Application #62195821, Confirmation Number 1654, 23rd July 2015.
- Gandhi PG, Rao GH (2014) The spectral analysis of photoplethysmography to evaluate an independent cardiovascular risk factor. Int J Gen Med 7: 539-547.
- Gandhi PG, Rao GH, Maarek A (2015) Detection of neuropathy using a sudomotor test in type 2 diabetes. Degener Neurol Neuromuscul Dis 5: 1-7.
- Maarek A, Gandhi PG, Rao GH (2015) Identifying autonomic neuropathy and endothelial dysfunction in Type II diabetic patients. EC Neurol 22: 63-78.
- Rao GH, Gandhi PG (2014) Need for a non-invasive diagnostic platform for early detection and management of cardiometabolic disorders. J Clin Prevent Cardiol 3: 93-98.
- Rao GH, Gandhi PG, Sharma V (2014) Clinical complications of Type-2 Diabetes Mellitus in South Asians and Chinese populations: An overview. J Diabetes Metab 5: 1-8.
- Rao GH, Gandhi PG (2014) Integrative Medicine: Global perspective. J Homeop Ayurv Med 3: 1-4.
- Rao GH (2015) Integrative approach to health: Challenges and Opportunities. J Ayurveda Integr Med 6: 215-219.
- Rao GH (2012) Prevention of vascular disease and development of affordable health care for all: Thinking out of box. View Point. J Clin Prevent Cardiol 1: 31-34.
- Rao GH (2015) Non-traditional approaches to diagnosis and management of type-2 diabetes mellitus: Point of View. J Diabetes Metab 6: 1-3.
- Rao GH (2018) Risk prediction, assessment, and management of type-2 diabetes. EC Endocrinol Metab Res 3: 30-41.
- Rao GH (2018) Risk scores for acute vascular events: Expectations and Limitations. J Cardiol 2: 1-9.
- Spence JD (2004) Ultrasound measurements of atherosclerosis. Stroke 35: e87-e88.
- Landry A, Spence JD, Fenster A (2004) Measurement of carotid plaque volume by 3-dimensional ultrasound. Stroke 35: 864-869.