Review Article
Genetic Aspect of Clopidogrel Resistance: An Indian Scenario
Kavita Shalia1*, Sunila Raju1 and VK Shah2
Corresponding author:Kavita K. Shalia, Sr. Scientist, Sir H.N. Medical Research Society, Sir H.N. Hospital and Research Centre, Court House, L. T. Road, Mumbai 400 002, India, E-mail: kavita.shalia@rfhospital.org
Citation: Sunila Raju. Genetic Aspect of Clopidogrel Resistance: An Indian Scenario Indian J Cardio Biol Clin Sci. 2016;3(1): 107.
Copyright © 2015 Sunila Raju, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Cardio Biology & Clinical Sciences | Volume: 3, Issue: 1
Submission: 17/09/2016; Accepted: 06/10/2016; Published: 15/10/2016
Abstract
Clopidogrel is an oral, thienopyridine class anti-platelet agent used to inhibit blood clots and is one of the most widely used in patients with coronary artery disease, peripheral vascular diseases, and cerebrovascular disease to prevent myocardial infarction and stroke.However, it has been reported that anti-platelet drugs such as Clopidogrel do not prevent the risk of ischemic events completely leadingto a number of reoccurring ischemic events. This non responsiveness is referred as Clopidogrel resistance wherein less than 30% inhibition of the platelet aggregation in response to Clopidogrel is considered as low or weak-response, while less than 10% is termed as Clopidogrel resistance. The variation in response to Clopidogrel from subject to subject has been attributed to several factors such as non-adherence to treatment, poor bioavailability, accelerated platelet turnover, drug interactions; as well as on certain genetic factors. Here we review the variations in the genetic components associated with its transport, activation and target of action in Indian population.
Keywords: Cardiovascular disease; Single nucleotide polymorphism; Genetic testing
Introduction
Action of drug is dependent on various processes that include absorption, activation, metabolism and excretion which in turnare dependent on individual’s metabolic machinery consisting of enzymes, receptors, transporters etc. And efficacy of later depends on their corresponding genetic component from which they descend. In this field of pharmacogenomics which is able to predict variability in drug response, a highly prescribed anti-platelet agent, Clopidogrel, has found its place.
Clopidogrel
Clopidogrel alone or combined with aspirin is routinely used to treat patients with a variety of vascular disorder. It is an oral, thienopyridine class anti-platelet agent used to inhibit blood clots and is one of the most widely used in patients with coronary artery disease, peripheral vascular diseases, and cerebrovascular disease to prevent MI and stroke [1]. Clopidogrel is a pro-drug which requires hepatic bio-activation involving 2 steps, which is regulated by cytochrome CYP4502C19 (CYP2C19). This active metabolite of the drug then binds irreversibly to the platelet adenosine diphosphate (ADP) receptor P2Y12, which inhibits platelet degranulation, glycoprotein IIb, IIIa (GP IIbIIIa) receptor activation and thus platelet aggregation [2].
Clopidogrel Resistance
“Resistance” or “non-responsiveness” to an anti-platelet drugis a pharmacodynamic phenomenon where there is no significant (clinically important) change in platelet function after treatment as compared to the baseline. The response towards Clopidogrel is mainly studied by determining the difference in the platelet aggregation by an agonist adenosine diphosphate (ADP) in vitro before and after drug administration by light transmittance aggregometry [3]. The difference in the platelet aggregation is the degree of inhibition of platelet activation. A change in maximal aggregation of less than or equal to 30% from baseline in response to Clopidogrel therapy, is defined as ‘weak-response’ and less than 10% inhibition of the platelet aggregation is considered as ‘resistance’ [4]. The response of platelets to Clopidogrel varies between different individuals as well as in different ethnic groups. In spite of the significant benefits of dual antiplatelet treatment proven in various studies, adverse ischemic events, including stent thrombosis, do occur [5]. Variation in Clopidogrel response have been confirmed by many studies wherein the incidence of non- responsiveness range from 4% to 40% [3].
The mechanisms underlying Clopidogrel resistance have been attributed to non-adherence to treatment, poor bioavailability, accelerated platelet turnover, drug interactions as well as to certain genetic factors. Variations of Multidrug Resistance Protein-1(MDR-1), Cytochrome P450 2C19 (CYP2C19), and P2Y12 genes are proposed which influence the response to Clopidogrel [6,7]. Some polymorphisms may lead to increased expression of the gene or decreased expression of the gene. Thus, any polymorphism in these genes causing phenotypic variations will alter the function ofClopidogrel.
Genes associated with Clopidogrel response
MDR-1: This gene encodes a drug efflux transporter called as MDR-1 or P - glycoprotein-1 (P-gp) also known as ATP- binding cassette subfamily B member-1 (ABCB-1) or cluster of differentiation 243 (CD243) which is an ATP-dependent drug efflux pump of the cell membrane that pumps many foreign substances out of the cell. It is extensively distributed and expressed in intestinal epithelium where it pumps xenobiotic back into the intestinal lumen. It has broad substrate specificity responsible for decreased drug accumulation in multidrug resistant cells. Variations in its expression may either accumulate the drug causing drug toxicity or increased excretion may not allow any pharmacologic response [8].
Cytochrome P450 2C19 (CYP2C19): This gene encodesCYP2C19 enzyme that acts on 10-15% of drugs in current clinical usesuch as proton pump inhibitors, antiepileptic drugs etc. For the antiplatelet Clopidogrel, CYP2C19 activates it by carrying out 45% of thefirst step in biotransformation of its pro-drug [9]. Hence, expression and function of CYP2C19 gene plays a pivotal role in Clopidogrel metabolism. Any polymorphism in this gene will modify the activity of the enzyme leading to reduced or increased concentration of active metabolite.
P2Y12: P2Y12 is found mainly but not exclusively on the surface of blood platelet. It belongs to the Gi class of a group of G protein coupled (GPCR) purinergic receptor and is a chemoreceptor for ADP and strongly associated with an increase in ADP-induced platelet aggregation. It is a potential target for treatment of clotting disorders [10]. Genetic variations within these receptor may alter the effect of the treatment.
Polymorphism in MDR-1 gene
The MDR-1 gene is located on the long arm of chromosome 7 and consists of a core promoter region and 28 exons. It is polymorphicwith single nucleotide polymorphisms (SNPs) in noncoding region such as in introns and wobble position [11]. A functional SNP resulting in transition of C→T at 3435 has been most studiedpolymorphism in MDR-1 gene wherein as compared to C3435 allele, T3435 is associated with decreased expression and has been shown to hinder with the intestinal absorption of Clopidogrel, thereby reducing its antiplatelet activity [12].
Table 1 depicts study on prevalence of C3435T genotypes in Indian population. Balram et al. have demonstrated total 82% of individuals with carriers of T3435 allele (C3435T or T3435T) andfrequency of the T3435 allele 0.62 in the Indian population residing inSingapore [13]. In another study from Western India, the frequency of T3435 allele of MDR-1 has been shown 0.61 with 88% of their study population with T3435 allele [14]. Near to this in Western Indian population, our study has reported T3435 allele frequency 0.52 and 73.5% of the population with T3435 allele [15]. Recently, in a study by Sridharan et al. among healthy subjects from Mumbai, T3435 allele frequency was calculated to be 0.64 with 85.5% of study population carriers of T3435 allele [16]. Thus in our population the carriers of variant allele of MDR-1 (T3435) associated with decreased Clopidogrel response are more than 70%. Therefore, identification of these different variants may be useful in optimizing therapy with this drug and others which are substrate of MDR-1.
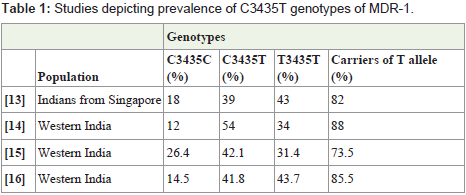
Table 1: Studies depicting prevalence of C3435T genotypes of MDR-1.
Polymorphism in CYP2C19 gene
Genetic variations of CYP2C19 are CYP2C19*1 wild type, CYP2C19*2, [G681A] with splicing defect, and CYP2C19*3 [G636A] with stop codon. CYP2C19*2 and CYP2C19*3 comprises about 95% of the poor metabolizer type [17-19]. CYP2C19*2 is the most common among the various reduced function genes studied and is the prime indicator of Clopidogrel low responsiveness [20]. Other alleles such as CYP2C19*3, CYP2C19*4, CYP2C19*5, CYP2C19*6, CYP2C19*7 and CYP2C19*8 may also affect Clopidogrel metabolism in similar manner as CYP2C19*2, but their frequency in the general population is negligible as compared to CYP2C19*2 [21]. In studies conducted by Scott et al. and Price et al. another allelic variant of CYP2C19 i.e. CYP2C19*17 (C806T; 50-flanking region of the gene), which is associated with increased enzyme activity is shown to have higher platelet inhibition as compared to the wild type variant [22,23]. Several studies conducted proposed the influence of polymorphism in CYP2C19 on Clopidogrel response [6].
Studies from different ethnic groups from different regions have been depicted in Table 2 demonstrating distribution of CYP2C19 variants. Among these CYP2C19*2 loss of function allele is very common in Indian population as compared to the other worldwide populations. In north Indians, Lamba et al. have reported frequencyof CYP2C19*2 to be 0.297 [24]. Adithan et al. for the Tamilian population have reported 0.379 while Mizutani et al. have reported CYP2C9*2 allele frequency to vary from 0.3-0.35 amongst Asianpopulations [25,26]. Similar to this, our study from western region of India has demonstrated allelic frequency of CYP2C19*2 to be 0.352 [15]. However, in a population from Kerala, Mahadevan et al. have reported high prevalence of CYP2C19*2 allele; 0.66 which is two times higher as compared to the frequency in the other regions of the country [27].
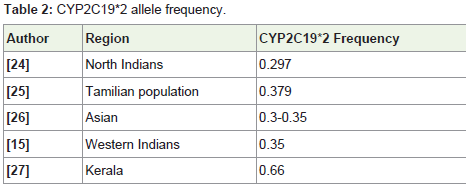
Table 2: CYP2C19*2 allele frequency.
CYP2C19*3 is another variant which is associated with thepoor metabolizer allele. Although it was reported to be 2.2% inTamilian population by Adithan et al. other studies by Lamba et al.and by Shetkar et al. in North region and including ours in Westernregion have not reported any prevalence of CYP2C19*3 variant[5,15,24,25]. Unlike the above variants of CYP2C19, other rare loss of function alleles such as CYP2C19*4 and CYP2C19*5 have not been well studied in Indian population and are very rare in other worldwide populations [22]. In a meta-analysis by Mega et al. it has been reported that the carriers of either CYP2C19*2 or CYP2C19*3;reduced function allele have a relative reduction of 32.4% of the activemetabolite of Clopidogrel in their plasma as compared to the noncarriers[28]. Further they have reported 55-76% increase in relative cardiovascular death, myocardial infarction or stroke as well as 2.6- 4.0 fold increase in risk of stent thrombosis in patients with decreased Clopidogrel response due to presence of “Poor Metabolizer” variants of CYP2C19.
In contrast to the “Poor Metabolizer” variants of CYP2C19, another variant CYP2C19*17 which is termed as “Rapid Metabolizer” leading to its increased enzyme function is also reported in certain studies [29]. This rapid metabolizer variant which leads to increased enzyme function may increase risk of bleeding in the carriers of CYP2C19*17 [30]. There is a large disparity among the Indian population for CYP2C19*17 allele. In the western region population of India, we have reported CYP2C19*17 frequency to be 10.2% while in a study on South India Tamilian Population by Anichavezhi et al. have reported its frequency to be almost double i.e. 19.2% [15,31]. This difference is attributed to different ethnic population with varied genetic pool among the studied groups [5].
Polymorphism in P2Y12 gene
P2Y12 has 2 functional haplotypes designated as H1 and H2 tagged by 4 SNPs in absolute linkage disequilibrium i.e. i-C139T, iT744C, i-ins 801A, G52T. Where H1 haplotype has a ‘C’ in position 139 of intron 1, a ‘T’ in position 744 of intron 1 and absence of i-ins 801A in intron 1 and 52 G of exon 2. H2 haplotype comprise 139T, 744C as well as presence of i-ins 801 A in intron 1 and 52 T of exon 2. Out of these two haplotypes, H2 is associated with enhanced platelet reactivity in response to ADP [32]. However, Malek et al. have reported that carrier of i-744C allele without variant allele of CYP2C19*2 did not have significantly decreased platelet response to ADP [33]. From Western Zone of India, our study has reported prevalence of genotypes H1/H1, H1/H2 and H2/H2 as 85.7%, 11.8% and 2.94% respectively with frequency of P2Y12 (i-744C) allele associated with enhanced platelet reactivity calculated as 0.088 [15]. In a recent study conducted by Sridharan et al, the frequency of wild type haplotype (H1/H1) of P2Y12 was reported to be 89.5% while 10.5% were shown to have (H1/H2) haplotype and in their study none of them showed the H2/H2 haplotype with allele frequency of i-744C as 0.052 [16]. In our study 19.2% (5/26) of the subjects with combination of variant genotypes CYP2C9*2 and P2Y12 (iT744C) demonstrated decreased platelet inhibition as compared with their wild type genotype which1 was also reported by Sridharan et al. and by Satam et al. [15,16,34]. In their studies nearly 60% and 52% of the study participant respectively were found to be poor responder to Clopidogrel [16,34].
Conclusion
There are few studies available on our population, but havedemonstrated presence of the variant allele of MDR-1, CYP2C19 andP2Y12 reported to be associated with decreased Clopidogrel response at a considerable frequency. Need of the hour first is larger studies, involving many ethnic groups to analyse the prevalence of variants. Second most important is to analyse other factors in association with genetic variation influencing resistance to Clopidogrel and then arrive at algorithm for appropriate dose calculation. It will be worthwhile to do genetic testing to determine individualised anti-platelet treatment and to decide adequate dose of Clopidogrel in resistant or moderate responder in patients undergoing Clopidogrel treatment. Moreover, this pharmacogenetic testing will be required in near future since the inclusion of “black box” warning by FDA recommending genetic testing prior to prescription of Clopidogrel [35].
Acknowledgements
The authors would like to acknowledge Rajawadi MunicipalHospital and Sir H.N. Hospital and Research Centre for recruitment of patients and Sir H.N. Medical Research Society for financial support for the corresponding original study carried out.
References
- Patrono C, Rocca B (2008) Aspirin: promise and resistance in the new millennium. Arterioscler Thromb Vasc Biol 28: s25-s32.
- King SB, Smith SC Jr, Hirshfeld JW Jr, Jacobs AK, Morrison DA et al. (2008) 2007 Focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association task force on practice guidelines: 2007 writing group to review new evidence and update the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention, writing on behalf of the 2005 Writing Committee. Circulation 117: 261-295.
- Papathanasiou A, Goudevenos J, Tselepis AD (2007) Resistance to aspirin and Clopidogrel: possible mechanisms, laboratory investigation, and clinical significance. Hellenic J Cardiol 48: 352-363.
- Yin T, Miyata T (2011) Pharmacogenomics of Clopidogrel: evidence and perspectives. Thromb Res 128: 307-316.
- Shetkar SS, Ramakrishnan S, SethS, Chandna P, Verma SK, et al. (2014) CYP 450 2C19 polymorphisms in Indian patients with coronary artery disease. Indian Heart J 66: 16-24.
- Nguyen TA, Diodati JG, Pharand C (2005) Resistance to Clopidogrel: a review of the evidence. J Am Coll Cardiol 45:1157-1164.
- Wiviott SD, Antman EM (2004) Clopidogrel resistance: a new chapter in a fast-moving story. Circulation 109: 3064-3067.
- Taubert D, von Beckerath N, Grimberg G, Lazar A, Jung N, et al. (2006) Impact of P-glycoprotein on Clopidogrel absorption. Clin Pharmacol Ther 80: 486-501.
- Kazui M, Nishiya Y, Ishizuka T, Hagihara K, Farid NA, et al. (2010) Identification of the human cytochrome P450 enzymes involved in the two oxidative steps in the bioactivation of Clopidogrel to its pharmacologically active metabolite. Drug Metab Dispos 38:92-99.
- Hollopeter G, Jantzen HM, Vincent D, Li G, England L, Ramakrishnan V, et al. (2001) Identification of the platelet ADP receptor targeted by antithrombotic drugs. Nature 409: 202-207.
- Tang K, Wong LP, Lee EJ, Chong SS, Lee CG (2004) Genomic evidence for recent positive selection at the human MDR-1 gene locus. Hum Mol Genet 13: 783-797.
- Fung KL, Gottesman MM (2009) A synonymous polymorphism in a common MDR-1 (ABCB1) haplotype shapes protein function. Biochim Biophys Acta 1794: 860-871.
- Balram C, Sharma A, Sivathasan C, Lee EJ (2003) Frequency of C3435T single nucleotide MDR-1 genetic polymorphism in an Asian population: phenotypicegenotypic correlates. Br J Clin Pharmacol. 56: 78-83.
- Ashavaid T, Raje H, Shalia K, Shah B (2010) Effect of gene polymorphisms on the levels of calcineurin inhibitors in Indian renal transplant recipients. Indian J Nephrol 20: 146-151.
- Shalia KK, Shah VK, Pawar P, Divekar SS, Payannavar S (2013) Polymorphisms of MDR-1, CYP2C19 and P2Y12 genes in Indian population: effects on clopidogrel response. Indian Heart J 65: 158-67.
- Sridharan K, Kataria R, Tolani D, Bendkhale S, Gogtay NJ, et al. (2016) Evaluation of CYP2C19, P2Y12, and ABCB1 polymorphisms and phenotypic response to Clopidogrel in healthy Indian adults. Indian J Pharmacol 48: 350-354.
- de Morais SM, Wilkinson GR, Blaisdell J, Nakamura K, Meyer UA, et al. (1994) The major genetic defect responsible for the polymorphism of S-mephenytoin metabolism in humans. J Biol Chem 269: 15419-15422.
- Hulot JS, Bura A, Villard E, Azizi M, Remones V, et al. (2006) Cytochrome P450 2C19 loss of- function polymorphism is a major determinant of Clopidogrel responsiveness in healthy subjects. Blood 108: 2244-2247.
- Brandt JT, Close SL, Iturria SJ, Payne CD, Farid NA, et al. (2007) Common polymorphisms of CYP2C19 and CYP2C9 affect the pharmacokinetic and pharmacodynamic response to Clopidogrel but not prasugrel. J Thromb Haemost. 5: 2429-2436.
- Shuldiner AR, O'Connell JR, Bliden KP, Gandhi A, Ryan K etal. (2009) Association of cytochrome P450 2C19 genotype with the anti-platelet effect and clinical efficacy of Clopidogrel therapy. JAMA 302: 849-857.
- Gladding P, Webster M, Zeng I, Farrell H, Stewart J, et al. (2008) The pharmacogenetics and pharmacodynamics of Clopidogrel response: an analysis from the PRINC (Plavix Response in Coronary Intervention) trial. JACC Cardiovasc Interv 1: 620-627.
- Scott SA, Sangkuhl K, Gardner EE, Stein CM, Hulot JS et al. (2011) Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and Clopidogrel therapy. Clin Pharmacol Ther 90: 328-332.
- Price MJ, Tantry US, Gurbel PA (2011) The influence of CYP2C19 polymorphisms on the pharmacokinetics, pharmacodynamics, and clinical effectiveness of P2Y12 inhibitors. Rev Cardiovasc Med 12: 1-12.
- Lamba JK, Dhiman RK, Kohli KK (2000) CYP2C19 genetic mutations in North Indians. Clin Pharmacol Ther 68: 328-335.
- Adithan C, Gerard N, Vasu S, Rosemary J, Shashindran CH, et al. (2003) Allele and genotype frequency of CYP2C19 in a Tamilian population. Br J Clin Pharmacol 56: 331-333.
- Mizutani T. (2003) PM frequencies of major CYPs in Asians and Caucasians. Drug Metab Rev 35: 99-106.
- Mahadevan L, Yesudas A, Sajesh PK, Revu S, Kumar P, et al. (2014) Prevalence of genetic variants associated with cardiovascular disease risk and drug response in the Southern Indian population of Kerala. Indian J Hum Genet 20: 175-184.
- Mega JL, Simon T, Collet JP, Anderson JL, Antman EM, et al. (2010) Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with Clopidogrel predominantly for PCI: a meta-analysis. JAMA 304: 1821-1830.
- Sim SC, Risinger C, Dahl ML, Aklillu E, Christensen M, et al. (2006) A common novel CYP2C19 gene variant causes ultrarapid drug metabolism relevant for the drug response to proton pump inhibitors and antidepressants. Clin Pharmacol Ther 79: 103-113.
- Rath P, Chidambaram S, Rath P, Dikshit B, Naik S, et al. (2015) A study on the impact of CYP2C19 genotype and platelet reactivity assay on patients undergoing PCI. Indian Heart J 67: 114-121.
- Anichavezhi D, Chakradhara Rao US, Shewade DG, Krishnamoorthy R, Adithan C (2012) Distribution of CYP2C19*17 allele and genotypes in an Indian population. J Clin Pharm Ther 37: 313-318.
- Fontana P, Dupont A, Gandrille S, Bachelot-Loza C, Reny JL, et al. (2003) Adenosine diphosphate-induced platelet aggregation is associated with P2Y12 gene sequence variations in healthy subjects. Circulation 108: 989-995.
- Malek LA, Kisiel B, Spiewak M, Grabowski M, Filipiak KJ, et al. (2008) Coexisting polymorphisms of P2Y12 and CYP2C19 genes as a risk factor for persistent platelet activation with Clopidogrel. Circ J 72: 1165-1169.
- Satam S, Pokharkar O, Thapar A, Zalawadia A (2016) Association of genetic polymorphism of CYP2C19, P2Y12 and response to Clopidogrel in healthy participants. Biolife 4: 1-12.
- Ellis KJ, Souffer GA, McLeod HL, Lee CR (2009) Clopidogrel pharmacogenomics and risk of inadequate platelet inhibition: US FDA recommendations. Pharmacogenomics 10: 1799-1817.