Review Article
Potential Future Therapies of Myocardial Ischemia Reperfusion Injury
Rachana Somaiya, Hima Patel, and Mukesh Nandave*
SPP School of Pharmacy & Technology Management, SVKM’s NMIMS, Vile Parle (W), Mumbai- 400056
*Corresponding author: Dr. Mukesh Nandave, SPP School of Pharmacy & Technology Management, SVKM’s NMIMS,
Vile Parle (W), Mumbai- 400056, India
Article Information: Submission: 05/03/2015; Accepted: 17/04/2015; Published: 22/04/2015
Abstract
Cardiovascular diseases are one of the leading causes of death in the world. Angioplasty, heart transplantation, thrombolysis, and
coronary bypass are general treatment approaches of cardiovascular diseases. All of these approaches can cause myocardial ischemia
reperfusion (MIR) injury that is known to occur on return of blood flow after myocardial infarction (MI). MIR injury fundamentally consists
of inflammation-related events and oxidative stress. Many anti-inflammatory and antioxidants are suggested for the treatment of injury.
However, despite a better understanding of pathophysiology of MIR injury, the majority of the clinical trials to prevent it have been
disappointing. Therefore, this review article provides a brief overview of the potential future natural and synthetic therapies recently
published in the research science for the treatment of MIR injury.
Introduction
Although recently there are many advances in the treatment of
ischemic heart diseases, Acute Myocardial Infarction is the leading
cause of mortality in developed countries [1]. Blood flow restoration
to earlier ischemic myocardium leads to Myocardial Ischemia
Reperfusion (MIR) Injury [2]. MIR injury appears during invasive
treatments for example, angioplasty [3], heart transplantation [4],
thrombolysis [5], and coronary by-pass [6]. Our objective is to review
new therapeutic strategies presently under research for preventing
MIR injury, as there is still no promising therapy for it. An intriguing
research area for MIR injury therapy shows potential in Therapeutic
hypothermia and Hydrogen sulfide treatment. However clinical
application for them is still nebulous. We have concentrated basically
on the research science that has been published within the past 24
months and shows potential for treatment of MIR injury.
Pathophysiology
The pathophysiology of MIR injury is multifactorial [7]. The
reactive oxygen species (ROS) is produced just after an ischemia
and plays an important role in MIR injury [8]. These oxygen species
are highly reactive having an unpaired electron and attacks to all cell biomolecules [7]. These highly reactive species can cause MIRinduced
lipid peroxidation, cardiac dysfunction, inhibition of Na+-K+
ATP-ase activity of Na membrane channels and mitochondrial
electron transport chain [9]. Antioxidant treatments including
enzymatic pathways and non-enzymatic pathways can reduce
infarct size induced by MIR; improve revival of the heart contractile
function, activities of ion transport and ATP content [10,11,]. After
reperfusion of infarcted myocardium, which is the conventional
choice of treatment for acute myocardial infarction, an inflammatory
reaction develops in tissue. The inflammation is essential for tissue
healing after MIR-induced injury [12]. Conversely, the blood flow
restoration to ischemic tissue leads to an extension of ischemiaassociated
tissue damage [9]. Neutrophils are main compounds of
this response [13]. The activated neutrophils also release mediators
such as, platelet activating factor, ROS, leukotrienes andthromboxane
thereby leading to tissue damage [14,15]. The other factor that plays
a role in MIR injury is complement system [16]. The myocardial cell
necrosis leads to release of constituents of subcellular membrane,
which are found abundant in mitochondria and are ableto trigger
complement cascade [17]. In addition to these factors, sometimes
although the reperfusion is supplied, blood flow cannot be provided
to myocardial tissue. This is known as ‘no-reflow phenomenon’ [9].
Potential Future Treatments For Mir Injury
Embelin administration [18]:
It has been observed that systemic ischemia-reperfusion injury
occurring after the cardiac arrest (CA) is a main factor that causes
problems [19]. Neutrophil extravasation and endothelial activation
following ischemia-reperfusion injury stimulates activation of
inflammatory cascade, ultimately triggering systemic inflammatory
response syndrome and leading to myocardial dysfunction with
multiple organ failure [20]. The previous studies support that antiinflammatory
activity is beneficial for MIR injury after resuscitation
[21]. Embelin is naturally occurring plant that has been used as antiinflammatory
to relieve fever and rheumatism [22]. It also reportedly
possesses antidiabetic [23], hepatoprotective [24], antioxidant [25],
antibacterial [26] and anti-inflammatory activities in other organs
[27-29]. However, as embelin was not been tested for its antiinflammatory
activity on MIR injury after CA, recently a study was
been formed to test its activity in a rabbit model [30]. It was observed
that embelin reverts Interleukin-1 beta (IL-1β), Interleukin 6 (IL-
6) and Tumor necrosis factor alpha (TNF-α) to basal levels and
reduces levels of cardiac troponin I (cTnI) in serum, apoptotic index
(AI), nuclear factor-kappa B (NF-κB) p65 and the necrosis ratio.
Furthermore, it was seen to improve myocardial and hemodynamics
function and myocardial morphology. Therefore, embelin shows
potential to protect the heart against the MIR injury following CA by
its anti inflammatory abilities.Mechanical Tissue Resuscitation [30]:
Negative pressure wound treatment increases cell preservation
by decreasing tissue edema, inflammation and enhancing blood flow
within areas that border a region of permanent cell death [31-33].
This resuscitation of tissue may lessen the final magnitude of cell
death within tissue positioned at risk for additional injury during
reperfusion. Mechanical tissue resuscitation (MTR) while using
a bioabsorbable matrix could be either placed using a marginally
invasive method following percutaneous revascularization process
or used at the period of open revascularization surgery. MTR is an
effective treatment for burns [33], traumatic brain injury [34] and
acute myocardial infarction [35]. Early cell death as well as delayed
programmed cell death, which is seen after MIR, decreases with
MTR treatment during reperfusion. This cardioprotective treatment
is, furthermore, related with increased blood flow and a significant
reduction in interstitial water. MTR with a resorbable device is
an efficient and straightforward mechanical strategy for reducing
cardiac muscle cell loss after myocardial infarction as an added
treatment to surgical revascularization.Protocatechuic Acid [36]:
Protocatechuic acid (PCA), a phenolic compound, is plentiful
in edible vegetables and fruits. PCA is well absorbed by humans and
animals and is one of the chief metabolites of complex polyphenols
such as procyanidins and anthocyanins, which arereportedto be
closely related to reductions of mortalities in neurodegeneration,
coronary heart disease and cancer [37,38]. PCA has beneficial effects
on treatments of neurodegenerative disease [39], inflammation
disease [40,41] and cancer [42,43]. However, in a recent study, PCA significantly reduced serum TNF- α level, infarct size and platelet
aggregation in in vivo rat model of MIR injury [36]. Experimental data
collected in a primary neonatal rat cardiomyocyte model of hypoxia/
reoxygenation injury indicated that in response to PCA, there was an
upregulated expression of phosphorylated Akt in the cardiomyocytes
subjected to hypoxia/reoxygenation injury and significant inhibition
of the expression of cleaved caspase-3and the apoptotic rate.
Therefore, PCA can give noteworthy protection against MIR injury
that may be at least moderately due to its inhibitions against MIR
injury including the platelet aggregation, cardiomyocytes apoptosis
and inflammatory response.Naloxone Post conditioning [44]:
Ischemic post conditioningis confirmed to protect brain and
heart, however has been found problematic to conduct clinically
[45-47]. As an exogenous intervention, the pharmacological
postconditioning presents similar endogenous protective mechanism
as Ischemic postconditioning. Pharmacological postconditioning
has confirmed many advantages such as controllability, convenient
operation, predictability and safety, proposing that it can be used
to prevent MIR injury [48-50]. Naloxone, an antagonist of opioid
receptors, can specifically antagonize the opioids and endogenous
opioids, enkephalins and endorphins. It is responsible for many
basic researches on antagonism of opioid receptors because of its
great affinity to opioid receptor [51]. Additionally, naloxone can
break and reverse the toxicity of the endogenous opioid receptors.
It also plays a substantial protective function in brain and renal
ischemia-reperfusion injury [52,53]. Naloxone is also able to protect
the reperfused cardiac muscle by inhibition of lipid peroxidation and
release of the inflammatory mediators and improvement of energetic
metabolism [54,55]. In a recent study, cell apoptosis andp-c-Jun
NH2-terminal kinase (p-JNK) was observed to be significantly lower
in the ischemia-reperfusion myocardial tissues after the naloxone
treatment as compared to ischemia-reperfusion group in Sprague
Dawley rats [44]. Furthermore, naloxone postconditioning is able
to significantly improve pathological injury of the ischemia cardiac
muscle. Naloxone has less side effects and low price and therefore,
may produce huge social and economic benefit if used extensively for
prevention of MIR injury.Betulinic Acid [56]:
Betulinic acid, a triterpene, has many botanical sources and is one
of the constituents chemically derived from botulin. This substance
is found in abundant quantity in outer bark of white birch trees
[57,58]. It has been found to possess activities like anti-inflammatory
[59,60] and antitumor [61-63]. Recent studies have established the
evidence of betulinic acid protecting against renal [58] and cerebral
ischemia reperfusion injuries [64]. In a recent study performed in an
open-chest anesthetized rat model, it was observed that pretreatment
with betulinic acid improves cardiac function and attenuates lactate
dehydrogenase (LDH) and creatine kinase (CK) activities compared
with ischemia-reperfusion rat group [56]. Therefore, betulinic acid
may moderate the release of CK and LDH, prevent cardiomyocytes
apoptosis and in turn alleviating the extent of the MIR injury.Aliskiren [65]:
Aliskiren, which is a renin inhibitor escalates the levels of
bradykinin and kallikrein in the cardiac tissue. In this research study,
female Sprague-Dawley rats were treated for 4 weeks prior to MIR
injury with drugs such asaliskiren and valsartan (angiotensin II
receptor antagonist)either alone or in combination, co-administered
with AT2 receptor antagonist PD123319 (30 mg/kg per day) or B2
receptor antagonist icatibant (0.5 mg/kg per day). It was found that aliskiren decreases valsartan-induced increases in angiotensin
II levels and increases levels of cardiac bradykinin. Angiotensin
AT1 receptor blockers and Angiotensin-converting enzyme (ACE)
inhibitors lessen MIR injury mediated via bradykinin B2 receptorand
angiotensin AT2 receptor mechanisms.Baicalein [66]:
12/15-Lipoxygenase (LOX), a catalyst involved in the
transformation of arachidonic acid to hydroxy-eicosatetraenoic acids (HETEs). Its levels are increased within the brain, myocardium
and endothelial cells in response to ischemia or hypoxia. Baicalein
(5,6,7-trihydroxyflavone) is a flavone, isolated from roots of
Scutellariabaicalensis (Lamiaceae) and also reported to be present in
Oroxylumindicum (Bignoniaceae). Being a specific LOX inhibitor,
Baicaleinprotects the kidney, heart and the brain against ischemia
reperfusion injury .On studying the mouse model, it was observed
that the 12/15-LOX was unregulated in a significant number in
the peri-infarct area which surrounded the primary infarction.
Inhibition of 12/15-LOX by Baicaleinblocks effects such as cardiac
injury, TUNEL positive cardiomyocytes, inflammatory responses
and oxidative stress. Baicalein also suppresses apoptosis as well asthe
activity of Caspase 3 in cultured myocteswhen an MIR injury is
simulated. Associated mechanisms are the activation of AKT pathway
and ERK1/2 and inhibition of activation of JNK1/2, p38 MAPK and
NF-kB/p65.Baicalein is a novel therapeutic drug for MIR injury.VitaePro [67]:
VitaePro is a mixture of antioxidants such as lutein, zeaxanthin
and astaxanthin in oil of safflower (Carthamustinctorius L.,
Compositae). The main function of antioxidants is that they act as
cardioprotective compounds.Lutein, a xanthophil pigment, has
been demonstrated to prevent peroxidation of lipids in cortex in a
diabetic rat cerebral cortex, induced by streptozocin. Zeaxanthin,
a major carotenoid pigment present in the retina of eye has been
demonstrated to decrease oxidative stress and end-stage liver disease.
Astaxanthin is a carotenoid pigment that protects the epithelial
cells of human lens against UV-B insults and possesses anticancer
activity. On comparison study between VitaePro and Vitamin E in
their cardioprotective activity in an ex vivo rat model of MIR injury,
it was found that VitaePro is a better cardioprotectant on the basis
of increased left ventricular functional revival, enhanced aortic flow,
decrease in the infarct size and decrease in the levels of thiobarbituric
acid reactive substances. VitaePro can be taken orally and decreases
the MIR injury by decreasing apoptosis and oxidative stress. However
to make its use in clinical application, the in vivo activity of VitaePro
is still to be established.α- lipoic acid (αLA) [68]:
αLA, a thiol antioxidant is present in food such as spinach,
tomatoes, and broccoli or is synthesized by the human liver. It is
a cofactor for various metabolic enzymes, which include α-ketoglutarate
dehydrogenase and puryvate dehydrogenase. It is currently
clinically used for treating conditions like lipid abnormality, diabetic
polyneuropathy and stroke. αLA and dihydrolipoic acid (its reduced
form) are ideal antioxidants as they have a low redox potential which
scavenge reactive oxidative species and help to regenerate Vitamin
E and C which are endogenous antioxidants. Hence, it can be put
to use in treating oxidative MIR injury. In an in vivo study carried
out on Adult male Sprague-Dawley rats, the administration of αLA
significantly reduced the levels of necrotic cell death markers which
include creatinine kinase and lactate dehydrogenase in the serum,
partially preserved the function of the left ventricle, decreased
the apoptosis and necrosis of cardiomyocytes, a reduction in the
myocardial infarct size, inhibition of TNF-α level and accumulation
of neutrophils which leads to reduction in the inflammation. The possible mechanism of action is the activation of PI3K/Akt pathway
(which mediates a protecting effect), prevention of stimulation of
iNOS gene expression, increased Nrf2 Nuclear Translocation (this up
regulates expression of a group of oxidative enzymes which include
NADPH-regenerating enzymes, HO-1, superoxide dismutase and
glutathione S-transferase, these help to fight against the oxidative
stress), inhibition of JNK1/2 and activation of ERK1/2. In in vitro
studies, it is reported to slacken the MIR injury.Mesenchymal Stromal Cells (MCS) [69]:
MCS are embryonic connective tissues cells, which are derived
from the mesoderm of adult muscle, umbilical cord, corneal stroma,
adipose tissue, etc. These multipotent cells have the ability to
differentiate into an array of cell types. A large number of experiments
are designed to investigate its use in acute kidney injury. Many
preclinical models have also been set up to test its efficacy in diseases
of lungs, liver and intestine. It has been shown that there is an
enhancement in the recruitment of MSC via CXCR7- and CXCR4-
dependent pathway and SDF-1 to the injured organ in response to
hypoxia. MCS are able to readily transmigrate into an inflamed tissue
and get incorporated into the endothelial layer. They possess the ability
to release mediators, which are locally generated in an inflammatory
response such as IL-6, IL-10, NO, TGF-b, IDO and prostaglandin
E2 (PGE2). They have the ability to release growth factors such as
hepatocyte growth factor (HGF), monocyte chemoattractant protein-
1 (MCP-1), fibroblast growth factor (FGF), insulin-like growth factor
(IGF), stromal cell- derived factor- 1(SDF-1), vascular endothelial
growth factor (VEGF) and also can stimulate angiogenesis and
proliferation which are categorized under cellular repair programs
and hence, benefitting the treatment of MIR injury. The induction of
T-cell expansion by MCS can prevent against allograft rejection and
hence indirectly protect against MIR injury. The pre-clinical study
using rat and porcine model has shown effects such as improved
cardiac functioning, suppress oxidative stress, reduction in the size
of an infarct, hindrance of fibrosis, increased angiogenesis and tissue
repair. On intravenous treatment of the analogue MSC- conditioned
media in rats the outcome was a surge in the capillary density, which
supports the cardiac function. Administering the same analogue
to pigs, the therapeutic effects included a reduction in infarct size,
improved cardiac repair and early protection of myocardium against
ischemia. There is an increase in the number of clinical trials for its
forthcoming clinical applications.Fusion of Glucagon-like peptide-1 (GLP-1) with domain antibody to serum albumin [70]:
In reaction to nutrient ingestion, an incretin hormone known
as GLP-1 is secreted by intestinal L-cells. It is responsible for
regulation of glucose homeostasis by stimulating insulin secretion
inhibiting glucagon secretion, promoting satiety and delaying gastric
emptying.GLP-1 receptors are expressed in both coronary and heart
vasculature. The receptor activation of GLP-1 by agonists leads to
arange of cardiovascular outcomes including cardioprotectionagainst
MIR injury both in vivo [71-76] and ex vivo [77-79]. The activated
GLP-1 holds extremely short half-life of 2 min after administrating
exogenously because it is quickly cleaved as well as inactivated due
to protease dipeptidyl peptidase-IV [80,81]. Such a short half-life is a limitation to its use as a therapeutic agent as determined by the
fact that studies with exogenously administered GLP-1 are reserved
to continuous infusion dosing procedure. Many of GLP-1 receptor
agonists have been recognized showing a long plasma half-life.
Exendin-4 is a 39 amino acid peptide. It is derived from the saliva of gila
monster.It possesses insulinomimetic and insulinotropic properties
through activation of GLP-1 receptors. But although having extended
plasma half-life (60 mins) than native GLP-1, exendin-4 needs twice
daily injection to attain anti-diabetic effects. Alternative strategy is to
createGAlbudAb (GLP-1 is genetically fused with DOM7h-14, which
is a domain antibody, dAb) with replacement of alanine at position
8 by glycine to give peptide dipeptidyl peptidase-IV resistant leading
to extended half-life. In a recent research study performed on male
Sprague-Dawley rats, there was comparison between long acting
GAlbudAb and exendin-4 (GLP-1 agonist having short half-life) for
infarct sizefollowing MIR injury. It was observed that exendin-4 and
GAlbudAb decrease the infarct size by 23% and 28% respectively
compared to vehicle after MIR injury. Furthermore, it was observed
that both exendin-4 and GAlbudAb improve post-ischemic cardiac
contractile role. However, cardioprotection provided by GAlbudAb
is better than that provided by exendin-4 as it is more sustained
in duration. Moreover, extremely low plasma concentration of
exendin-4 fails to protect heart from MIR injury, signifying that
sustained activation of GLP-1 receptor plays a main role in offering
cardioprotection in the setting of MIR injury. Long-acting GLP-1
agonists like GAlbudAb may demand additional evaluation as unique
therapy to reduce MIR injury.Suberoylanilidehydroxamic acid (SAHA) [82]:
SAHA, a histone deacetylase inhibitor that interferes with the
function of deacetylase, is approved for the treatment of cancer. The
classical uses of histone deacetylase inhibitor are in neurology and in
psychiatry, where they are used as anti-epileptics and mood stabilizers
and also used in treating cancer. They are currently under investigation
for the treatment of parasitic diseases, HIV, inflammatory diseases
and heart ailments. In the in vitro model using rabbit, it was observed
that the SAHA partially salvaged the systolic function, decreased the
infarct size and SAHA pretreatment in rat ventricular cardiomyocytes
reduced the cell death. It induces the autophagic flux, which leads to
recycling of cellular components. Therefore, it proves to be a novel
therepy for MIR injury and demands for further clinical studies.Chemerin15 [83]:
To prevent complications that are associated with extreme
inflammatory responses, it is important to control neutrophil
activation and neutrophil adhesion. ChemR23 that is expressed
in neutrophil granules is rapidly upregulated upon activation of
neutrophil.Chemerin15 (C15) is a 15-aa peptide that is derived from
chemerin (a chemoattractant protein). It promotes phagocytosis
of the cells that are apoptotic, through receptor ChemR23. It also
stops pro-inflammatory mediator production by macrophages. It
is observed that in vitro studies, C15 reduces neutrophil adhesion
andchemotaxis and inhibits the integrin’s activation and its
clustering. It is also seen to modulate neutrophil physiology, thereby
inducing detachment of adherent cell from inflamed endothelium,
while also reducing recruitment of neutrophil and cardiac damage in a murine myocardial infarction model. ChemR23 mediates all these
effects. Consequently, pathway of C15/ChemR23 is identified to be a
new regulator and therefore curative target in pathologies driven by
neutrophil.Thymoquinone [84]:
Thymoquinone is a volatile oil constituent, which is derived from
seeds of Nigella sativa. It is an antioxidant and has anticonvulsant
and analgesic effects, also showing potential anti-cancer effect.
Thymoquinone reduces ROS generation, apoptosis and infarct size in
an ex vivo study performed on rat heart. It also enhanced ventricular
function and coronary flow of ischemic hearts. It attenuates the
ischemia reperfusion-induced up-regulation of Stress-activated
protein kinase/c-Jun NH(2)-terminal kinase (SAPK/JNK),P38-
MAPK expression and Tumor necrosis factor alpha (TNF-α) and
increases ratio of Bcl-2/Bax. As there is inhibition of ROS generated-
NF-kappaB induction, itleads to inhibition of pro-inflammatory
cytokines. Therefore, this natural compound can be employed as one
of the therapies in treating MIR injury.Cyclosporine [85]:
The detrimental effects of reperfusion occur in a form of
mitochondrial dysfunction, which has been considered as
permeability transition. The membrane potential collapses because
of the opening of nonspecific high-conductance channel in the
inner mitochondrial membrane. This leads to cardiomyocyte death.
Cyclosporine, along with being immunosuppressive, also inhibits
mitochondrial permeability transition. It reduces the infarct size
in patients having acute myocardial infarction. It is hypothesized
that cyclosporine causes inhibition of mitochondrial permeability
transition by preventing interaction of cyclophilin D with pore
component, that is induced by calcium.Although this mechanism
is uncertain for reducing the infarct size since cyclosporine is not
seen to specific for cyclophilin D, it has some other intracellular
effects too. In a rabbit model, it was observed that NIM811 (a
cyclosporine nonimmunosuppressive derivative) binds to matrix
cyclophilin D, and causes significant reduction of infarct size when
being administered at the time of reperfusion. Although long-time
use of cyclosporine has many detrimental effects like hepatic and
renal toxicity, cyclosporine is a good candidate to use at the time of
reperfusion as it is related with reduction in infarct size. However,
further detailed study in larger clinical trial has been suggested for
the confirmation.Conclusion
ROS produced after an ischemia plays a main role in MIR injury
by causing lipid peroxidation, cardiac dysfunction, inhibition of
Na+-K+ ATP-ase activity of Na membrane channels and mitochondrial
electron transport chain. Along with ROS, an extensive inflammatory
reaction having neutrophil as the main component, complement
system and no-reflow phenomenon can lead to MIR injury. Acute
Myocardial Infarction is the leading cause of mortality in developed
countries and yet there is no promising therapy for the treatment of
MIR injury. The new therapies discussed in this review article are
studied in animal models or in vitro studies and have shown to be
efficient by offering several advantages such as improving myocardial and hemodynamics function and myocardial morphology, giving
anti-inflammatory response, decreasing apoptosis and oxidative
stress and low price with less side effects. Thus, these potential
treatments can decrease the magnitude of impact caused by MIR
injury. Therefore, much work still remains to be done and these new
methods are suggested to be studied in clinical trials as well to make it
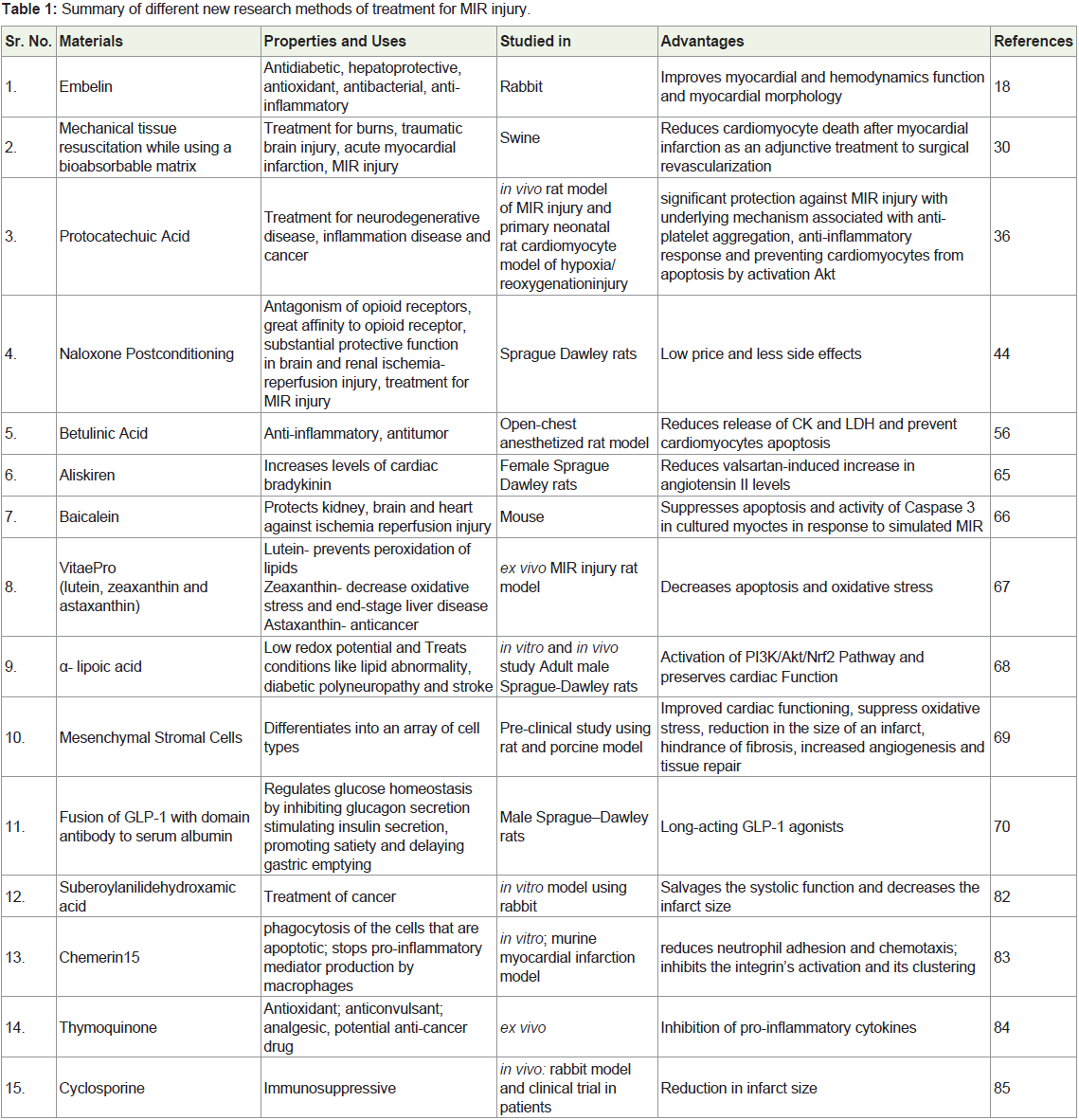
routine way of treatment for MIR injury (Table 1).
References
Citation
Somaiya R, Patel H, Nandave M. Potential Future Therapies of Myocardial Ischemia Reperfusion Injury. Indian J Cardio Biol Clin Sci. 2015;2(1): 105.