Review Article
Non HDL-C as the Primary Target for Lipid-Lowering Therapy: Moving beyond LDLCentric Management
Kapil Dev1 and Manish Bansal2*
Corresponding author:Dr. Manish Bansal MD, DNB Cardiology, FASE, FISCU, Senior Consultant Cardiology, Medanta- The Medicity, Sector 38, Gurgaon, Haryana- 122001, India, Ph: +91-124-4141414, Fax: +91-124-4834111,; E-mail: manishaiims@hotmail.com
Citation: Dev K, Bansal M. Non HDL-C as the Primary Target for Lipid-Lowering Therapy: Moving beyond LDL-Centric Management. Indian J Cardio Biol Clin Sci. 2015;2(1): 104.
Copyright © 2015 Manish Bansal et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Cardio Biology & Clinical Sciences | Volume: 2, Issue: 1
Submission: 06/01/2015; Accepted: 24/02/2015; Published: 28/02/2015
Abstract
The value of lowering low-density lipoprotein cholesterol (LDL-C) is widely known with a large number of studies demonstrating benefit of LDL-C lowering in a wide range of patient populations. Accordingly, LDL-C has been the focus of lipid lowering therapy for a long period.However, recent data suggest that non-high density lipoprotein cholesterol (non-HDL-C) may be a better target for lipid management than LDL-C. Unlike LDL-C, non-HDL-C includes all atherogenic particles present in blood and therefore provides more complete estimation of cardiovascular risk, esp. in patients with atherogenic dyslipidemia or those already on statin therapy. Further, measurement of non-HDL-C is simple, no extra blood test is required and there is no need for fasting sampling.
Introduction
Worldwide, cardiovascular disease (CVD) is one of the leading causes of death and it is anticipated that in the next decade its contribution to disease burden will further rise sharply [1,2]. The challenge is even greater for low- and middle-income countries that face the double jeopardy of rising CVD incidence and prevalence as well as still widely prevalent communicable diseases.
CVD, fortunately, is a largely preventable disease with ample evidence showing reduction in its incidence and prevalence through aggressive control of risk factors. In this context, dyslipidemia has great relevance, not only because it contributes to a large proportion of CVD but also because effective non-pharmacological and pharmacological means are available to correct it.
Over the past few decades, understanding of the role of lipoprotein metabolism in the pathogenesis of CVD has grown immensely. Numerous population-based observational and interventional studies have demonstrated that low-density lipoprotein cholesterol (LDL-C) is an important prognostic marker of CVD [3,4], and also that lowering of LDL-C through lifestyle measures as well as drugs such as statins results in profound reduction in CV risk [5-8]. Based on this evidence, all the current guidelines emphasize on LDL-C as the primary target for lipid-lowering therapy in the management as well as prevention of CVD [9,10].
However, epidemiological and interventional studies have also shown that individuals reaching their LDL-C target may still be at significant residual risk of CVD, despite aggressive use of statins [11,12]. Further, it has been reported that nearly half of all patients having ‘normal’ cholesterol levels may suffer recurrent acute coronaryevents [13]. Therefore, it is becoming increasingly obvious that although LDL-C is a well founded target for lipid-lowering, it is not the only atherogenic lipid molecule in the blood and therefore not the ‘complete’ measure of CVD risk [14,15]. Very low density lipoprotein (VLDL), intermediate density lipoprotein (IDL) and chylomicrons also play an important role in the pathogenesis and progression of atherosclerosis which needs to be accounted for [9]. Non-high density lipoprotein cholesterol (non-HDL-C), which is an aggregate measure of all the atherogenic lipoproteins present in blood, has thereforeemerged as a superior predictor of CVD risk than LDL-C (12) in awide range of patient populations [14,16-18].
What is non-HDL-C?
Non HDL-C represents the sum of the cholesterol content of all the lipid particles in blood, except HDL (Figure 1). Since all lipid particles other than HDL [i.e. VLDL, IDL, LDL, lipoprotein (a)] are atherogenic, non-HDL-C actually represents cholesterol content of all the atherogenic lipid particles in blood. Measurement of non-HDL-C does not require any additional test as it can be easily calculated by subtracting HDL-C from total cholesterol, available as part of a routine lipid profile (non HDL-C= total cholesterol – HDL-C).
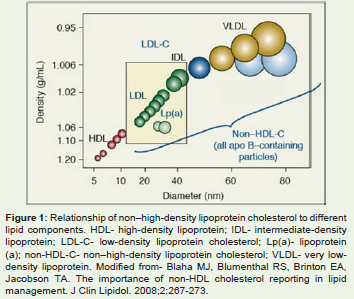
Figure 1: Relationship of non–high-density lipoprotein cholesterol to differentlipid components. HDL- high-density lipoprotein; IDL- intermediate-densitylipoprotein; LDL-C- low-density lipoprotein cholesterol; Lp(a)- lipoprotein(a); non-HDL-C- non–high-density lipoprotein cholesterol; VLDL- very lowdensitylipoprotein. Modified from- Blaha MJ, Blumenthal RS, Brinton EA,Jacobson TA. The importance of non-HDL cholesterol reporting in lipidmanagement. J Clin Lipidol. 2008;2:267-273.
Non HDL-C is a robust lipid measurement and has distinct advantages over LDL-C (Table 1). First, unlike LDL-C, measurement of non-HDL-C does not necessarily require fasting sample as both total cholesterol and HDL-C are not acutely affected by feeding. In contrast, LDL-C, which is often calculated from Freidwald equation instead of direct measurement, requires a fasting sample. As per Freidwald equation, LDL-C is estimated as-
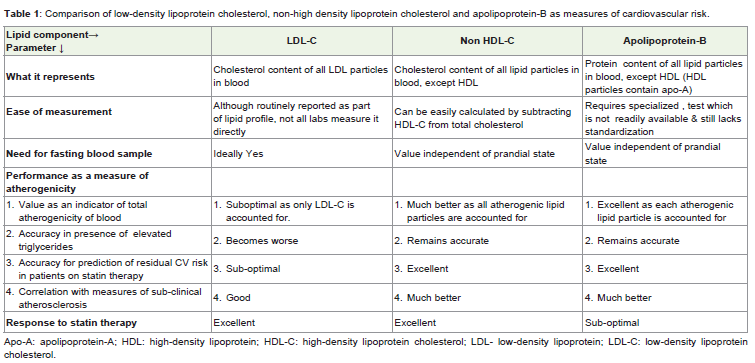
Table 1: Comparison of low-density lipoprotein cholesterol, non-high density lipoprotein cholesterol and apolipoprotein-B as measures of cardiovascular risk.
LDL-C = Total cholesterol – HDL-C – (serumtriglycerides/5)
Since serum triglyceride level is acutely elevated by feeding, a non-fasting sample will underestimate LDL-C by this method.
Second, as discussed below, non-HDL-C, by including all the different atherogenic lipid molecules in blood, has been shown to be a more complete measure of atherogenicity and a much stronger predictor of CVD risk. For these reasons, non-HDL-C has already been included as a secondary target of therapy in several guidelines on lipid management [9]. It is recommended that the non-HDL-C level should not exceed LDL-C by more than 30 mg/dl at any point.
The rationale behind this recommendation is that non-HDL-C primarily reflects the sum total of LDL-C and VLDL-C and 30 mg/ dl cholesterol in VLDL-C would correspond to serum triglyceride level of 150 mg/dl, which is the acceptable upper limit of normal for triglycerides [9].
Dynamic relationship between atherogenic lipoproteinsand apolipoproteins
Each lipid molecule in the blood contains at least one molecule of an apolipoprotein. The apolipoprotein in LDL, IDL, VLDL, lipoprotein (a) and chylomicrons is apolipoprotein-B (Apo-B) whereas it is Apo-A in HDL molecules. The Apo-B concentration in blood is therefore directly proportional to the number of atherogenic lipid particles present and thus reflects the total atherogenic potential. For this reason, Apo-B levels have been shown to be an excellent predictor of CV risk, far superior to LDL-C [19-21]. As non-HDL-C measures cholesterol content of all the Apo-B containing particles, it correlates closely with Apo-B levels. In contrast, the relationship between LDL-C and Apo-B is quite variable. Under normal conditions, almost 90% of all the Apo-B in the blood is carried by LDL particles and therefore LDL-C levels tend to correlate with Apo-B levels. However, this concordant relationship between Apo-B and LDL-C is diminished in patients who have elevated triglycerides. When the levels of IDL and VLDL increase as in hypertriglyceridemia, the contribution of these particles to total Apo-B pool increases and the relationship between LDL-C and Apo-B weakens [22,23]. In addition, higher VLDL levels are also associated with greater proportion of small-dense LDL particles, which further weakens this relationship. Excess triglyceride in VLDL particles is exchanged for the cholesterol present within the LDL particles. Subsequent hydrolysis of triglycerides transferred to LDL renders the LDL particles smaller, denser and more atherogenic. As the proportion of small-dense LDL particles increases, more number of LDL particles are now available for the same amount of cholesterol. As a result, LDL-C alone will underestimate the total atherogenic burden whereas non-HDL-C, by incorporating information about VLDL and IDL, still remains more accurate and shows better correlation with serum Apo-B levels. The clinical recognition of this phenomenon has become increasingly important now with the rising prevalence of obesity, metabolic syndrome and diabetes mellitus. These are the conditions characterized by disproportionately elevated triglycerides, low HDL-C, increased proportion of small-dense LDL and normal or near-normal LDL-C levels [24]- the typical setting in which non- HDL-C becomes a superior risk marker than LDL-C.
Non-HDL-C as a measure of atherosclerosis risk
Non HDL-C and CV risk prediction: As stated earlier, the atherogenic lipoprotein paradigm suggests that for determination of CV risk, total number of atherogenic particles is more important than the conventional lipid parameters such as LDL-C. Being an aggregate measure of all atherogenic lipoproteins, non-HDL-C is therefore expected to be a more accurate predictor of CV risk as compared to LDL-C. This hypothesis has been proven in a number of studies that have shown better prediction of CV risk by non HDL-C, than LDL-C, with an accuracy comparable to that of Apo-B [14,18,25-27].
In the Lipid Research Clinics Program, 4462 middle agedindividuals who were free from CVD were followed up for an average of 19 years. It was found that non-HDL-C was a much stronger predictor of all cause and CV mortality as compared to LDL-C (chi square 24.3 for non-HDL-C and 5.0 for LDL-C) [14]. A 30 mg/dl increase in non-HDL-C resulted in 19% increase in mortality in men and 11% increase in women compared to 15% and 8% respectively for LDL-C. In 2003, Lu et al studied 4549 diabetic patients in the Strong Heart Study and compared the ability of various lipid measures for prediction of CV risk [22]. In both men and women, the hazard ratio for the upper tertile of non-HDL-C was found to be higher than the same for LDL-C and triglycerides. The greater predictive accuracy ofnon-HDL-C than LDL-C in diabetics was further established in a posthoc analysis of 4 large prospective studies-The Framingham Cohort Study, The Framingham off spring study, The Lipid Research Clinics Program follow up study and Multiple Risk factor intervention trial25. A total of 19381 individuals who were above 30 years of age and were free from CVD were included in this post-hoc analysis. This analysis demonstrated that compared to non-diabetics, the diabetic subjects had significantly higher non-HDL-C levels (176.7 and 194.1mg/dl respectively, p< 0.001) but almost identical LDL-C levels (148.0 and 148.6 mg/dl respectively, p=0.68). On multivariate analysis, CVD risk in diabetics increased with increase in non-HDL-C but not LDL-C.
The predictive accuracy of various lipid measures in a secondary prevention setting was evaluated in the BARI trial (Bypass Angioplasty Revascularization Investigation) [26], which was primarily conducted to compare coronary bypass surgery with angioplasty in patients with multi-vessel coronary artery disease. A total of 1514 patients were included and followed up for 5 years. Once again, non-HDL-C was found to be a significant independent predictor of non-fatal myocardial infarction and angina whereas LDL-C did not predict either of these end-points.
Non-HDL-C and CV risk in relation to serum triglycerides levels: Since elevated non-HDL-C, when out of proportion to LDL-C levels, suggests increased concentration of triglyceride rich lipoproteins such as VLDL, it becomes imperative to determine whether the increased CV risk associated with non-HDL-C is attributed to increased serum triglyceride levels. Several studies have demonstrated that non- HDL-C is a strong predictor of CV risk independent of triglyceride levels [23,28]. Non-HDL-C was found to maintain its predictive value for CV events in patients with triglycerides levels< 200mg/dl as in the EPIC-Norfolk (European Prospective Investigation into Cancer and nutrition-Norfolk) study [28], and also at triglyceride levels > 400mg/dl as in the SHEP (Systolic Hypertension in the Elderly Program) study [23]. In contrast, LDL-C lost its predictive value when triglyceride levels exceeded 400mg/dl [23].
Non-HDL-C in comparison to Apo-B: Since non-HDL-C servesas a surrogate for Apo-B, the two have also been compared for their ability to predict CV risk. In the Health Professionals Follow-up study involving 18225 men, 40 to 75 years of age, non-HDL-C was found to be an inferior predictor of CV events as compared to Apo-B [21]. However, in another study done in 15632 healthy women aged 45 years and above (The Women Heart study), the highest quintile of non-HDL-C had similar relative risk for major CV events as the highest quintile of Apo-B [27]. It is noteworthy that in both these studies, non-HDL-C performed much better than LDL-C.
Non-HDL-C and correlation with measure of subclinicalatherosclerosis: Orakzai et al studied asymptomatic individualsundergoing coronary artery calcium (CAC) screening and foundstatistically significant association between non HDL-C and presence of CAC [29]. In yet another study, Kowamoto et al evaluated the relationship between non-HDL-C and carotid atherosclerosis as assessed on carotid duplex imaging. The study showed similar results, with non HDL-C being a better predictor of carotid atherosclerosis than LDL-C [30]. The PDAY (Pathological Determinance of Atherosclerosis in Youth) study [31] provided further evidence about the relationship between non-HDL-C and subclinical atherosclerosis. The study correlated autopsy findings with various lipid parameters in young individuals who had died of external causes. It found that non-HDL-C was significantly associated with presence of fatty streaks at the site of examination (i.e. thoracic and abdominal aorta and right coronary artery) but no significant association was found between Apo-B and fatty streaks.
Lipid lowering therapy and residual CV risk: Several patients who are on statins and who succeed in achieving the “target” LDL-C levels may still suffer from CV events [11]. These patients bear the brunt of having residual CV risk, not identified by traditional lipid markers. It has been shown that ‘on treatment’ LDL-C levels in patients on lipid lowering therapy do not very accurately reflect the residual CV risk whereas non-HDL-C and Apo-B continue to remain relatively accurate predictors of CV events even in this setting [12,32]. A combined analysis of the TNT (Treating to new Targets) and IDEAL (Incremental Decrease in Endpoints through Aggressive Lipid Lowering) studies involving 18018 patients clearly demonstrated a much stronger relationship between the risk of CV events and the‘on-treatment’ levels of non-HDL-C and Apo-B, as compared to LDL-C [12]. Yet another combined analysis of 8 trials showed that in statin-treated patients, though the levels of LDL-C, non–HDL-C, and Apo B were each associated with the risk of future major adverse CV events, the strength of this association was greater for non–HDL-C than for LDL-C (p=0.002) and Apo B (p=0.02) [32].
Treating elevated non-HDL-C
Since LDL-C is the main component of non-HDL-C, the initial treatment approach for elevated non-HDL-C is same as that for LDL-C [9]. Thus, aggressive life-style measures and statins form the mainstay of treatment. If non-HDL-C remains elevated despite adequate LDL-C lowering, further intensification of life-style measures and increase in the statin dose, if not already on maximum tolerated dose, should be tried. Weight reduction, smoking cessation and abstinence from alcohol are all quite effective in lowering triglycerides (and thus non-HDL-C) and should be actively pursued.In addition, at the same time, one should also diligently look for and correct any secondary causes of hypertriglyceridemia if present, such as uncontrolled diabetes, nephrotic syndrome, chronic renal failure, certain drugs (e.g. corticosteroids, protease inhibitors for human immunodeficiency virus infection, beta blockers, estrogens) etc [9].
If the non-HDL-C level still remains high in spite of abovemeasures, addition of a fibrate is a useful option. Although the most recent American College of Cardiology/ American Heart Association guidelines have discounted the role of non-statin drugs in the current management of dyslipidemia [10], there is reasonable evidence to suggest that fibrates may provide incremental CV risk reduction in patients with elevated triglyceride levels [33-35]. For example, in the ACCORD (Action to Control Cardiovascular Risk in Diabetes) Lipid study, when fenofibrate was added to the background statin therapy, it significantly reduced the incidence of CV events in patients who had atherogenic dyslipidemia [33]. This is consistent with the data from older studies comparing gemfibrozil and bezafibrate with placebo, which showed significant CV risk reduction with these agents, with more marked effects seen in those with elevated triglyceride levels [34,36-38].
Implications for clinical practice
Enough evidence has accumulated over the last decade to suggest that non-HDL-C may be a better predictor of CV risk than LDL-C in different patient populations. Basis these studies, many investigators have suggested to elevate the role of non-HDL-C as the primary target of lipid lowering therapy instead of LDL-C. The value of non-HDL-C in routine clinical practice was underscored by the recent consensus report from the American Diabetes Association and the American Heart Association that stated “routine calculation and use of non- HDL-C constitute a better index than LDL-C for identifying high risk patients and that calculation of non-HDL-C should be provided in all laboratory reports’’[24].
An additional advantage of using non-HDL-C as the primarytarget for therapy is that it does not involve any deviation from the current practice and does not attempt to undermine the significance of LDL-C [9]. As already mentioned above, the initial treatment strategy for elevated non-HDL-C is same as that for elevated LDL-C, irrespective of whether LDL-C is the primary target for therapy or non-HDL-C. However, using non-HDL-C as the main target of therapy ensures appropriate corrective measures in patients who continue to have elevated non-HDL-C levels despite having achievedLDL-C target. Although this too is included in the current guidelines as the secondary target for therapy, it often gets overlooked because of continued overemphasis on LDL-C alone.
Though Apo-B has been shown to be a better predictor of CVrisk than non HDL-C or LDL-C, its application in routine clinical practice is difficult. Measurement of Apo-B requires a special assay which is expensive, time-consuming, not readily available and is still not standardized. Moreover, there is yet to be a consensus on optimum target levels of Apo-B in different patient populations [24,39,40]. Given these practical limitations, non-HDL-C remains the best alternative for regular clinical use.
Conclusions
Although there is no ambiguity that LDL-C is a strong predictor of CV risk in a wide range of patient populations and also that lowering of LDL-C through various measures results in concomitant reduction in the risk of CV events, there is now enough evidence to justify much greater importance to non HDL-C also, both as a marker of CV risk and as a target for therapy.
Many patients who meet their LDL-C goals fall short of their non-HDL-C goals. Under-reporting or non-reporting of non- HDL-C levels may therefore result in failure by the treating physician to recognize this and target elevated non-HDL-C, thereby leading to residual CV risk despite being on statin therapy. Non-HDL-C levels should therefore be routinely reported in all lipid profiles. It can be easily calculated without the need for any additional testing, does not require fasting sampling and is already a recommended target for therapy, though not a primary one. Routine report of non-HDL-C will be one valuable step towards improved patient outcomes through better prediction of CV risk, esp. the residual CV risk in patients already on lipid lowering therapy.
References
- Yusuf S, Reddy S, Ounpuu S, Anand S (2001) Global burden of cardiovascular diseases: Part I: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 104: 2746-2753.
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012) Disability-adjusted life years (dalys) for 291 diseases and injuries in 21 regions, 1990-2010: A systematic analysis for the global burden of disease study 2010. Lancet 380: 2197-2223.
- Kannel WB, Dawber TR, Thomas HE, Jr., McNamara PM (1965) Comparison of serum lipids in the prediction of coronary heart disease. Framingham study indicates that cholesterol level and blood pressure are major factors in coronary heart disease; effect of obesity and cigarette smoking also noted. R I Med J 48: 243-250.
- Gotto AM, Whitney E, Stein EA, Shapiro DR, Clearfield M, et al. (2000) Relation between baseline and on-treatment lipid parameters and first acute major coronary events in the air force/texas coronary atherosclerosis prevention study (AFCAPS/TexCAPS). Circulation 101: 477-484.
- Pedersen TR, Kjekshus J, Berg K, Haghfelt T, Faergeman O (1994) Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: The scandinavian simvastatin survival study (4s). Lancet 344: 1383-1389.
- (1998) Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The long-term intervention with pravastatin in ischaemic disease (lipid) study group. N Engl J Med 339:1349-1357.
- (2002) Mrc/bhf heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 360: 7-22.
- Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, et al. (1996) The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and recurrent events trial investigators. N Engl J Med 335: 1001-1009.
- (2002) Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel iii) final report. Circulation 106: 3143-3421.
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, et al. (2014) 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the american college of cardiology/american heart association task force on practice guidelines. Circulation 129: S1-45.
- Davidson MH (2005) Reducing residual risk for patients on statin therapy: The potential role of combination therapy. Am J Cardiol 96: 3K-13K.
- Kastelein JJ, van der Steeg WA, Holme I, Gaffney M, Cater NB, et al. (2008) Lipids, apolipoproteins, and their ratios in relation to cardiovascular events with statin treatment. Circulation 117: 3002-3009.
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. (2010) Executive summary: Heart disease and stroke statistics--2010 update: A report from the american heart association. Circulation 121: 948-954.
- Cui Y, Blumenthal RS, Flaws JA, Whiteman MK, Langenberg P, et al. (2001) Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med 161: 1413-1419.
- Hoenig MR (2008) Implications of the obesity epidemic for lipid-lowering therapy: Non-hdl cholesterol should replace ldl cholesterol as the primary therapeutic target. Vasc Health Risk Manag 4: 143-156.
- Blaha MJ, Blumenthal RS, Brinton EA, Jacobson TA (2008) The importance of non-hdl cholesterol reporting in lipid management. J Clin Lipidol 2: 267-273.
- Ramjee V, Sperling LS, Jacobson TA (2011) Non-high-density lipoprotein cholesterol versus apolipoprotein b in cardiovascular risk stratification: Do the math. J Am Coll Cardiol 58: 457-463.
- Liu J, Sempos CT, Donahue RP, Dorn J, Trevisan M, et al. (2006) Non-high-density lipoprotein and very-low-density lipoprotein cholesterol and their risk predictive values in coronary heart disease. Am J Cardiol 98: 1363-1368.
- Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, et al. (2001) High apolipoprotein b, low apolipoprotein a-I, and improvement in the prediction of fatal myocardial infarction (amoris study): A prospective study. Lancet 358: 2026-2033.
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, et al. (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the interheart study): Case-control study. Lancet 364: 937-952.
- Pischon T, Girman CJ, Sacks FM, Rifai N, Stampfer MJ, et al. (2005) Non-high-density lipoprotein cholesterol and apolipoprotein b in the prediction of coronary heart disease in men. Circulation 112: 3375-3383.
- Lu W, Resnick HE, Jablonski KA, Jones KL, Jain AK, et al. (2003) Non-hdl cholesterol as a predictor of cardiovascular disease in type 2 diabetes: The strong heart study. Diabetes Care 26: 16-23.
- Frost PH, Davis BR, Burlando AJ, Curb JD, Guthrie GP Jr, et al. (1996) Serum lipids and incidence of coronary heart disease. Findings from the systolic hypertension in the elderly program (shep). Circulation 94: 2381-2388.
- Brunzell JD, Davidson M, Furberg CD, Goldberg RB, Howard BV, et al. (2008) Lipoprotein management in patients with cardiometabolic risk: Consensus conference report from the american diabetes association and the american college of cardiology foundation. J Am Coll Cardiol 51: 1512-1524.
- Liu J, Sempos C, Donahue RP, Dorn J, Trevisan M, et al. (2005) Joint distribution of non-hdl and ldl cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care 28: 1916-1921.
- Bittner V, Hardison R, Kelsey SF, Weiner BH, Jacobs AK, et al. (2002) Non-high-density lipoprotein cholesterol levels predict five-year outcome in the bypass angioplasty revascularization investigation (bari). Circulation 106: 2537-2542.
- Ridker PM, Rifai N, Cook NR, Bradwin G, Buring JE (2005) Non-hdl cholesterol, apolipoproteins a-I and b100, standard lipid measures, lipid ratios, and crp as risk factors for cardiovascular disease in women. JAMA 294: 326-333.
- Arsenault BJ, Rana JS, Stroes ESG, Després JP, Shah PK, et al. (2009) Beyond low-density lipoprotein cholesterol: Respective contributions of non-high-density lipoprotein cholesterol levels, triglycerides, and the total cholesterol/high-density lipoprotein cholesterol ratio to coronary heart disease risk in apparently healthy men and women. J Am Coll Cardiol 55: 35-41.
- Ndrepepa G, Orakzai SH, Nasir K, Blaha M, Blumenthal RS, Raggi P (2009) Non-hdl cholesterol is strongly associated with coronary artery calcification in asymptomatic individuals. Atherosclerosis 202: 289-295.
- Kawamoto R, Oka Y, Tomita H, Kodama A (2005) Non-hdl cholesterol as a predictor of carotid atherosclerosis in the elderly. J Atheroscler Thromb 12: 143-148.
- Rainwater DL, McMahan CA, Malcom GT, Scheer WD, Roheim PS, et al. (1999) Lipid and apolipoprotein predictors of atherosclerosis in youth: Apolipoprotein concentrations do not materially improve prediction of arterial lesions in pday subjects. The pday research group. Arterioscler Thromb Vasc Biol 19: 753-761.
- Boekholdt SM, Arsenault BJ, Mora S, Pedersen TR, LaRosa JC, et al. (2012)Association of ldl cholesterol, non-hdl cholesterol, and apolipoprotein b levels with risk of cardiovascular events among patients treated with statins: A meta-analysis. JAMA 307: 1302-1309.
- Ginsberg HN, Elam MB, Lovato LC, Crouse JR 3rd, Leiter LA, et al. (2010) Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med 362: 1563-1574.
- Sacks FM, Carey VJ, Fruchart JC (2010) Combination lipid therapy in type 2 diabetes. N Engl J Med 363: 692-694.
- Tenenbaum A, Fisman EZ (2012) Fibrates are an essential part of modern anti-dyslipidemic arsenal: Spotlight on atherogenic dyslipidemia and residual risk reduction. Cardiovasc Diabetol 11: 125.
- Frick MH, Elo O, Haapa K, Heinonen OP, Heinsalmi P, et al. (1987) Helsinki heart study: Primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med 317: 1237-1245.
- Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, et al. (1999) Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans affairs high-density lipoprotein cholesterol intervention trial study group. N Engl J Med 341: 410-418.
- Tenenbaum A, Motro M, Fisman EZ, Tanne D, Boyko V, et al. (2005) Bezafibrate for the secondary prevention of myocardial infarction in patients with metabolic syndrome. Arch Intern Med 165: 1154-1160.
- Genest J, McPherson R, Frohlich J, Anderson T, Campbell N et al. (2009) 2009 canadian cardiovascular society/canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol 25: 567-579.
- Contois JH, McConnell JP, Sethi AA, Csako G, Devaraj S, et al. (2009) Apolipoprotein B and cardiovascular disease risk: Position statement from the aacc lipoproteins and vascular diseases division working group on best practices. Clin Chem 55: 407-419.