Review Article
Pathophysiology of Coronary Microvascular Dysfunction
S.R. Mittal*
Corresponding author: S.R. Mittal, Department of Cardiology, Mittal Hospital & Research Centre, Pushkar Road, Ajmer(Raj.), India, Tel: 0145-2421988; E-mail: sarweshwarm@gmail.com
Citation: Mittal SR. Pathophysiology of Coronary Microvascular Dysfunction. Indian J Cardio Biol Clin Sci. 2014;1(1): 101.
Copyright © 2014 S.R. Mittal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Cardio Biology & Clinical Sciences | Volume: 1, Issue: 1
Submission: 22/03/2014; Accepted: 18/04/2014; Published: 20/04/2014
Reviewed & Approved by Dr. Satyen Parida, Associate Professor, Department of Anesthesiology & Critical Care, JIPMER, Puducherry, India
Abstract
Coronary microvascular dysfunction is a group of disorders with heterogenous pathophysiology. At present there are no methods to pinpoint the underlying structural and functional disorder in a given patient. Identification of exact pathophysiology is necessary to tailor correct diagnostic approach and therapeutic modality.
Keywords: Angina; Coronary Artery Disease; Ischemic Heart Disease; Microvasculature; Syndrome X
Introduction
Coronary microvascular dysfunction is considered when there is angina with normal coronary angiogram, coronary flow reserve is less than 2.5 on adenosine induced hyperemia and there is no spasm of epicardial coronaries on acetylcholine provocation. Possibility of primary coronary microvascular dysfunction can be considered only after excluding secondary causes like- Obstructive coronary artery disease by OCT / IVUS /PET- Myocardial diseases like HCM , DCM- Iatrogenic - Post PCI, Post CABGUnderlying pathophysiology is heterogenous. This is responsiblefor nonuniform response to different diagnostic tests and therapeuticapproaches.
(a) Gender Differences
Structural differences in microvasculature and coronary reactivity have been observed between two sexes [1]. It is not clear if there are any sex differences in pathophysiology and risk factors [2]. Pathogenesis of such differences and their clinical relevance in microvascular angina is not clear.
(b) Site of Lesion
Presently, all vessels not seen on coronary angiography are grouped as “microvesselsâ€. Anatomically these include epicardial prearterioles, intramyocardial arterioles and subendocardial capillaries [3]. Lesion at any site will increase microvascular resistance. Capillaries do not dilate in response to adenosine due to absence of smooth muscles. Therefore, they are the site of maximum microvascular resistance during hyperemia [4]. Further, problems at the level of interstitium or myocytes will also present as angina with normal coronary angiograms. Opherk et al. [5] found swelling of mitochondria on electron microscopy of left ventricular biopsy. Arterioles, metaarterioles, capillaries and venules were normal. Etiopathology, clinical and laboratory profile, response to different therapies and prognosis may differ according to site of lesion. Rinkevich et al. [6] compared myocardial contrast echocardiography in women with syndrome X and controls. They indirectly concluded that coronary resistance vessels are the site of microvascularabnormality. However at present, there are no methods that can pinpoint the site of lesion in vivo.
(c) Structural Alterations
Microvascular dysfunction could be due to several structuralalterations -(i) Rarefaction - Reduced number of arterioles and capillariesper unit of myocardium [7]. Myocardial infarction, hypertension,diabetes and end stage dilated cardiomyopathy are associated with reduced myocardial capillary density [8]. These conditions are,however, also associated with several other pathologies that canproduce angina.(ii) Interstitial infiltration [8](iii) Perivascular fibrosis [9](iv) Medial hypertrophy: On transarterial left ventricularendomyocardial biopsy, Opherk et al found occasional small arterieswith a media with more than two muscle cell layers [5].(v) Atherosclerosis [7](vi) Microembotization: Plaque and vessel wall constituentsincluding lipid, matrix, endothelial cells, fibrin and plateletthrombi can embolize following thrombolysis or intervention [10].Preexisting microvascular disease may reduce the adaptive capacityto embolization. Such reduction in adaptive capacity may be relatedto underlying disease eg diabetes or vasculitis. Genetic factors mayalso predispose an individual’s microcirculation to decreased capacityto accommodate particulate matter.(vii) Myocyte alterationStrategy for management may differ depending on pathology.Opherk et al. [5] found no evidence of small vessel disease ontransarterial left ventricular endomyocardial biopsy of patientswith syndrome X. Endomyocardial biopsy has been found to havelow sensitivity [5]. It could be due to patchy distribution of disease[11]. However, quantitative measurement of coronary artery sizewith adenosine, acetylcholine and nitroglycerine has revealed similarmeasurements in left anterior descending and circumflex arteriessuggesting a diffuse rather than localized pathology [12]. Lowyield of endomyocardial biopsy could also be due to the fact thatendomyocardial biopsy can study only endocardium and adjacentmyocardium. Pathology of epicardial prearterioles and myocardialarterioles are not evaluated. Vessels between 110-200 u are notaccessible to electrone microscopic examination [5]. It is also possible that structural alteration are not present in all cases. Microvascularangina may result from functional abnormalities without detectablestructural abnormality [13].
(d) Functional Alterations
Several distrubances of microvascular function can be involved ingenesis of microvascular angina.(i) Increased resting tone. In some patients it can be indirectlysuspected if there is abnormal cardiac adrenergic nerve function atrest [14] or there is slow flow phenomenon on coronary angiographywith reduced coronary sinus oxygen saturation [15]. This may bepresent even when symptoms are relatively quiescent and may betransient [16]. There is, however, no noninvasive method to suspectthis possibility. Clinical significance in microvascular angina is notclear.(ii) Hypercontractile response to various stimuli [15,17].Ergonovine injection, mental stress, cold pressor and hyperventilationhave been shown to cause constriction of coronary microcirculation.Exercise has also been shown to cause abnormal coronary vasomotion in patients with normal coronary arteries and reduced coronary flowreserve [18]. However, response to various stress stimuli in laboratorymay not correlate with events of daily life. It may result in falsepositive as well as false negative results.(iii) Transient spasm [19]. Transient diffuse microvascular spasmhas been proposed as an explanation for angina with ST segmentelevation in presence of normal epicardial coronary arteries duringintracoronary administration of acetylcholine. However most of thepatients are likely to have isolated or concomittant spasm of epicardialcoronaries. Literature on isolated coronary microvascular spasm isscanty and response to acetylcholine in catheterization laboratorymay not correctly represent events occurring outside the laboratory.(iv) Decreased capacity to dilate - endothelium dependent and/orendothelium independent [20].(v) Compression of intramyocardial vessels by theintramyocardial pressure.Several factors govern flow in microcirculation [21]Table 1.Abnormalities of some of these factors has been observed in someclinical studies [22-26]. Decreased coronary dilatory capacityhas been concluded by reduced coronary blood flow response tovarious pharmacological agents [5,20]. Response to acetylcholineis considered to represent reduced nitric oxide release fromendothelium. However acetylcholine also has direct vasoconstrictioneffect [27]. Further, it may not affect the metabolic pathway of nitricoxide in some cases [28]. Adensoine and dipyridomole produceendothelium independent vasodilation through relaxation of smoothmuscle cells. There could be several yet unknown factors. Responseto few pharmacological agents may not correctly represent responseto various stimuli of day to day life. Identification of exact functionalalteration and it’s cause will help in development of specific therapy.
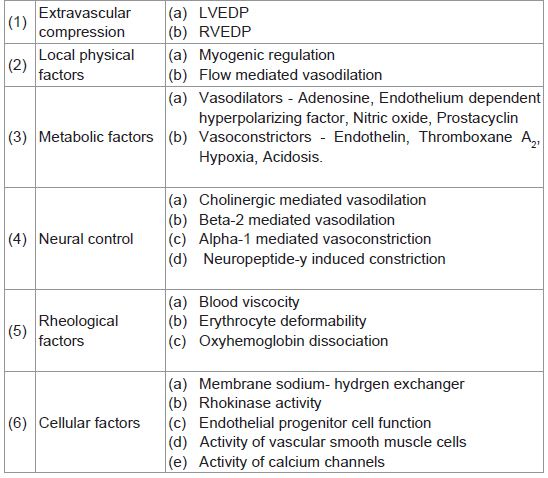
Table 1: Factors governing microcirculation.
(e) Rheological Disorders
As capillaries are the site of maximum resistance during hyperemia, factors that hamper blood flow through capillaries canalso contribute to microvascular angina. These include (i) Increased blood viscosity. Common causes are increasedhematocrit & lipids [29]. Rinkevich et al. [6], however, observedno difference in hematocrit between patients of syndrome X andcontrols.(ii) Erythrocyte diameter, charge and deformability [30].(iii) Defect of oxyhemoglobin dissociation
(f) Disorder of Cellular Mechanisms
Endothelial progenitor cells and circulating endothelial cells havethe potential for repair of endothelium [31]. Women with decreasedcoronary flow reserve have been shown to have lower number anddecreased function of CD 34 cells [31]. Further studies are needed todefine role of these cells in pathophysiology of microvascular angina.
Vascular smooth muscle cells play an important role in vascular reactivity [32] and their abnormality could be involved in increasing resting microvascular tone or decreasing vasodilatory response. Airway hyperresponsiveness [33] and esophageal motility disorder [34] have been observed in some cases of syndrome X. Diffuse disorder of smooth muscle responsiveness has been proposed. Further work is needed to find role of vascular smooth muscle cell hyperresponsiveness in microvascular angina.
(g) Association of Systemic Microvascular Dysfunction
Strain et al. [35] compared skin microvascular response to heating and ischemia among men with refractory angina and controls. Skin microvascular function was impaired in individuals with refractory angina. It is possible that microvascular angina is part of systemic microvascular dysfunction. Pathophysiological significance of this observation needs evaluation of microvasculature in different vascular territories in patients with documented microvascular angina.
Conclusion
Microvascular angina is a group of disorders with hetrogenous pathophysiology. At present, no specific investigations can be advised as multiple factors may exist in the same patient. Various groups of drugs are used to tackel this condition but no therapy is uniformly effective because of hetrogenous pathophysiology. Identification of exact pathophysiology will help in deciding correct diagnostic and therapeutic approach in a given patient. Future studiesshould be directed towards development of techniques to define pathophysiology in a given patient.
References
- Campbell DJ, Somaratne JB, Jenkins AJ, Prior DL, Yii M, et al. (2011) Differences in myocardial structure and coronary microvasculature between men and women with coronary artery disease. Hypertension 57: 186-192.
- Vaccarino V, Badimon L, Corti R, de Wit C, Dorobantu M , et al. (2011) Ischemic heart disease in women : are there sex differences in pathophysiology and risk factors ? Position paper from the working group on coronary pathophysiology and microcirculation of the European Society of Cardiology. Cardiovasc Res. 90: 9-17.
- Yilmaz A, Sechtem U (2012) Angina pectoris in patients with normal coronary angiograms : current pathophysiological concepts and therapeutic options. Heart 98: 1020-1029.
- Kaul S, Jayaweera AR (2008) Myocardial capillaries and coronary flow reserve. J Am Coll Cardiol 52: 1399-401.
- Opherk D, Zebe H, Weihe E , Mall G , Durr C, et al. (1981) Reduced coronary dilatory capacity and ultrastructural changes of the myocardium in patients with angina pectoris but normal coronary arteriograms. Circulation 63: 817- 825..
- Rinkevich D, Belcik T, Gupta NC, Cannard E, Alkayed NJ, et al. (2013) Coronary autoregulation is abnormal in syndrome X : insights using myocardial contrast echocardiography. J Am Soc Echocardiogr 26: 290-296.
- Camici PG, Crea F (2007) Coronary microvascular dysfunction. N Engl J Med 356: 830-840.
- Tsagalou EP , Anastasiou-Nana M , Agapitos E , Gika A , Drakos SG, et al. (2008) Depressed coronary flow reserve is associated with decreased myocardial capillary density in patients with heart failure due to idiopathic dilated cardiomyopathy. J Am Coll Cardiol 52: 1391-1398.
- Elliott PM, Kindler H, Shah JS , Sachdev B , Rimoldi OE, et al. (2006) Coronary microvascular dysfunction in male patients with Anderson - Fabry disease and the effect of treatment with alpha galactosidase A. Heart 92: 357-360.
- Topol EJ, Yadav JS (2000) Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation 101: 570-580.
- Maseri A, Crea F, Kaski JC, Crake T (1991) Mechanisms of angina pectoris in syndrome X. J Am Coll Cardiol 17: 499-506.
- Reis SE, Holubkov R, Lee JS, Sharaf B, Reichek N, et al. (1999) Coronary flow velocity response to adenosine characterizes coronary microvascular function in women with chest pain and no obstructive coronary disease . Results from the pilot phase of the Women’s Ischemia Syndrome Evaluation (WISE) study . J Am Coll Cardiol 33: 1469-1475.
- Herrmann J, Kaski JC, Lerman A (2012) Coronary microvascular dysfunction in the clinical setting : from mystery to reality. Eur Heart J 33: 2771-2782.
- Lanza GA, Giordano A, Pristipino C, Calcagni ML, Meduri G , et al. (1997) Abnormal cardiac adrenergic nerve function in patients with syndrome X detected by (123I)metaiodobenzylguanidine myocardial scintigraphy. Circulation 96: 821-826.
- Beltrame JF, Limaye SB, Wuttke RD, Horowitz JD (2003) Coronary hemodynamic and metabolic studies of the coronary slow flow phenomenon. Am Heart J 146: 84-90.
- Fragasso G, Chierchia SL, Arioli F, Carandente O, Gerosa S, et al. (2009) Coronary slow flow causing transient myocardial hypoperfusion in patients with cardiac syndrome X : long term clinical and functional prognosis. Int J Cardiol 137: 137-144.
- Chauhan A, Mullins PA, Taylor G, Petch MC, Schofield PM (1993) Effect of hyperventilation and mental stress on coronary blood flow in syndrome X. Br Heart J 69: 516-524.
- Bortone AS, Hess OM, Eberli FR, Nonogi H, Marolf AP, et al. (1989) Abnormal coronary vasomotion during exercise in patients with normal coronary arteries and reduced coronary flow reserve. Circulation 79: 516-527.
- Sun H, Mohri M, Shimokawa H, Usui M, Urakami L, et al. (2002) Coronary microvascular spasm causes myocardial ischemia in patients with vasospastic angina. J Am Coll Cardiol 39: 847-851.
- Chauhan A, Mullins PA, Taylor G, Petch MC, Schofield PM (1997) Both endothelium - dependent and endothelium - independent function is impaired in patients with angina pectoris and normal coronary angiograms. Eur Heart J 18: 60-68.
- Canty JM Jr. (2012) Coronary blood flow and myocardial ischemia .In Bonow RO, Mann DL, Zipes DP, Libby P (ed). Braunwalds Heart Disease. Saunders, Missouri: 1049-75.
- Clarke JG, Davies GJ, Kerwin R, Hackett D, Larkin S, et al. (1987) Coronary artery infusion of neuropeptide Y in patients with angina pectoris. Lancet 1: 1057-1059.
- Koren W, Koldanov R, Peleg E, Rabinowitz B, Rosenthal T (1997) Enhanced red cell sodium hydrogen exchange in microvascular angina. Eur Heart J 18: 1296-1299.
- Kaski JC, Cox ID, Crook JR, Salomone OA, Fredericks S, et al. (1998) Differential plasma endothelin levels in subgroups of patients with angina and angiographically normal coronary arteries. Am Heart J 136 : 412-417.
- Gulli G, Cemin R, Pancera P, Menegatti G, Vassanelli C, et al. (2001) Evidence of parasympathetic impairment in some patients with cardiac syndrome X. Cardiovasc Res 52: 208-216.
- Huang PH, Chen YH, Chen YL, Wu TC, Chen JW, et al. (2007) Vascular endothelial function and circulating endothelial progenitor cells in patients with cardiac syndrome X. Heart 93: 1064-1070.
- Lanza GA, Crea F (2010) Primary coronary microvascular dysfunction : clinical presentation, pathophysiology and management. Circulation 121: 2317-2325.
- Desideri G, Gaspardone A, Gentile M, Santucci A, Gioffre PA, et al. (2000) Endothelial activation in patients with cardiac syndrome X . Circulation 102: 2359-2364.
- Rim SJ, Leong - Poi H, Lindner JR, Wei K, Fisher NG, et al. (2001) Decrease in coronary blood flow reserve during hyperlipidemia is secondary to an increase in blood viscosity . Circulation 104: 2704-2709.
- Bin JP, Doctor A, Lindner J, Hendersen EM, Le DE, et al. (2006) Effects of nitroglycerin on erythrocyte rheology and oxyzen unloading : novel role of S-nitrosohemoglobin in relieving myocardial ischemia. Circulation 113: 2502-2508.
- Park KE, Pepine CJ (2011) Microvascular dysfunction : what have we learned from WISE ? Expert Rev Cardiovasc Ther 9: 1491-1494.
- Balcells M, Martorell J, Olive C, Santacana M, Chitalia V, et al. (2010) Smooth muscle cells orchestrate the endothelial cell response to flow and injury. Circulation 121: 2192 -2199.
- Cannon RO 3rd, Peden DB, Berkebile C, Schenke WH, Kaliner MA, et al. (1990) Airway hyperresponsiveness in patients with microvascular angina . Evidence for a diffuse disorder of smooth muscle responsiveness . Circulation 82: 2011-2017.
- Cannon RO 3rd, Cattau EL Jr, Yakshe PN , Maher K, Schenke WH, et al. (1990) Coronary flow reserve , esophageal motility and chest pain in patients with angiographically normal coronary arteries . Am J Med 88: 217-222.
- Strain WD, Hughes AO, Mayet J, Wright AR, Kooner J, et al. (2013) Attenuated systemic microvascular function in men with coronary artery disease is associated with angina but not explained by atherosclerosis. Microcirculation 20: 670-677.