Research Article
Qualitative and Quantitative Differentiation between Benign and Malignant Vertebral Lesions Using Diffusion Weighted MRI: A Prospective Study
Sriram R*, Kashikar R and Desai S B
Jaslok Hospital and Research Centre Cumballa Hill, Peddar Road, Mumbai, India
*Corresponding author: Sriram R, Jaslok Hospital and Research Centre Cumballa Hill, Peddar Road, Mumbai, India Email: drrithikasriram@gmail.com
Copyright: © 2023 Kaviya V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Submission: 22/02/2023; Accepted: 18/04/2023; Published: 24/04/2023
Abstract
Objectives: To differentiate benign from malignant vertebral lesions using Diffusion Weighted MRI Images (DWI) and Apparent Diffusion Coefficient (ADC) values.
Background: In elderly individuals, with no or minimal history of trauma, it is important to diagnose and differentiate benign and malignant lesions affecting the vertebrae. Conventional MRI cannot reliably differentiate benign from malignant vertebral lesions. DWI with ADC is a relatively novel and fast sequence which characterizes lesions based on their cellularity. Our hypothesis is that malignant lesions will show lower ADC values compared to benign by virtue of hypercellularity.
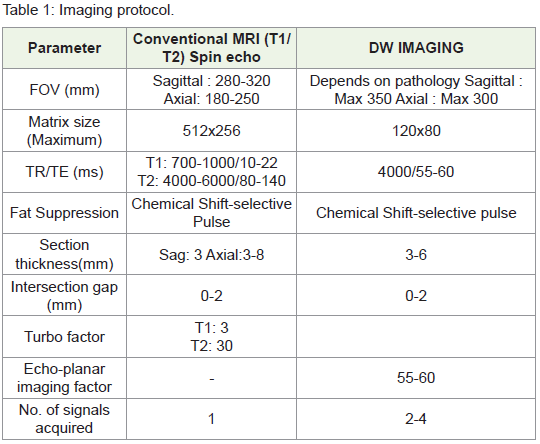
Materials and Methods: A hospital based prospective observational study was conducted with the guidelines of the ethical committee of the hospital. 46 patients with known vertebral lesions and who fulfilled the inclusion criteria were included in this study. Images were acquired on our 3T Philips Ingenia MRI machine and individual ADC values were obtained.
Results: Among 23 benign and 23 malignant vertebral lesions, malignant pathologies showed lower ADC values (0.62 x 10-3mm2/s) compared to benign lesions (1.08 x 10-3mm2/s). Cut-off ADC to distinguish benign from malignant lesions was found to be 0.73 ×10-3 mm2/s with a sensitivity and specificity
of 95.7% and 82.6% respectively. There was overlap between ADC values for TB (Tuberculosis) and malignancy.
Keywords: ADC; Osteoporosis; TB; Metastases
Introduction
Osteoporosis and osteopenia have affected nearly 50 million
people in India and 15-20% of the urban population aged over 50 years
show evidence of at least one vertebral fracture 1. The differential
diagnosis for a collapsed vertebra includes trauma, osteoporosis,
infections, primary bone tumors, metastasis and multiple myeloma.
In elderly individuals, with no or minimal history of trauma,
it is important to diagnose and differentiate benign and malignant
lesions affecting the vertebrae. The imaging investigation of
choice is conventional MRI which is sensitive but not specific in
differentiating among the various possible causes.
In recent years, investigators have studied Diffusion Weighted MRI (DW MRI) and its usefulness in lesions of the spine. Since DWMRI depends on cellularity of tissue, it can differentiate an acute benign collapse from metastases as malignant tissues are more cellular and show diffusion restriction.
The quantitative assessment of diffusion in DW MRI is done using
Apparent Diffusion Coefficient (ADC). Normal vertebra shows low
ADC value due to increased marrow fat which is responsible for water
movement restriction. In diseased vertebrae there will be increased
ADC values compared to normal vertebra, likely due to increased
water content.
In most studies, the ADC value in malignancy was found to be
significantly lower than in a benign process, possibly explained by
increased cellularity and hence further restricted diffusion.
Most studies however do not standardize the data processing and
ROI (region of Interest) calculation on ADC maps. Data on sensitivity
and specificity of ADC values in differentiating between infection
and malignancy is scarce. Fewer studies have been performed on the
diagnostic accuracy of ADC to differentiate tuberculous spondylitis
and metastases of the vertebrae, which is a necessity among the Indian
patient population.
In our study, we strive to prove the diagnostic accuracy of ADC
values in differentiating between benign and malignant lesions of
the vertebrae as well as among individual pathologies. We have
standardized the ROI in all patients.
Aim
Materials & Methods
Results
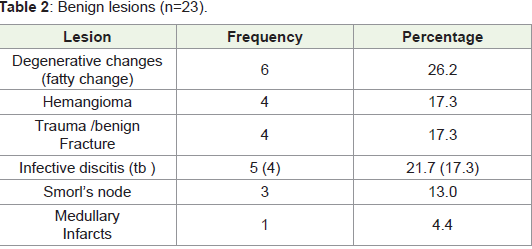
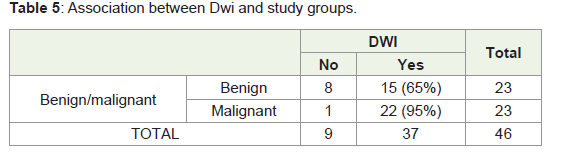
There were 23 benign and 23 malignant vertebral lesions in this
study Table 2-5 .
DWI restriction was defined as increased signal of the lesion
compared to adjacent marrow signal.
Independent t-test was done for testing the hypothesis, which
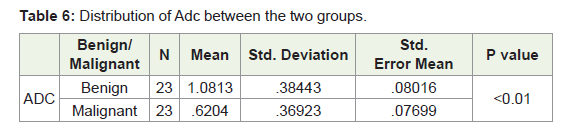
found that ADC scores can be used to distinguish between benign
and malignant cases (p <0.01).
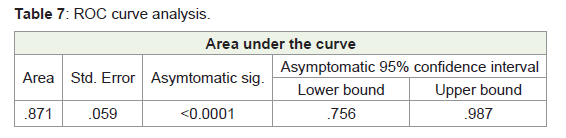
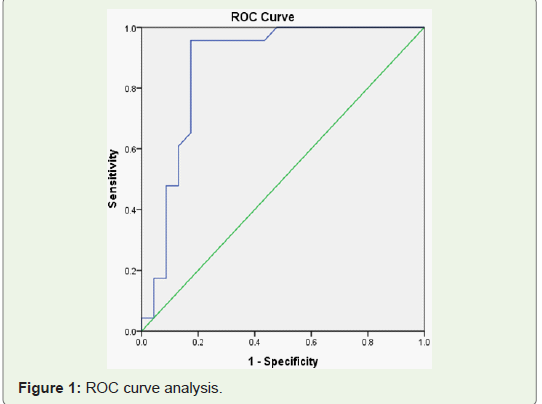
The area under the curve was found to be .871 (>0.5), which
indicates ADC have a significant association in determining whether
lesion is benign or malignant.
The cut-off ADC (x10 13) was found to be (×10-3 mm2/s) to
distinguish benign from malignant was 0.73 with a sensitivity and
specificity of 95.7% and 82.6% respectively.
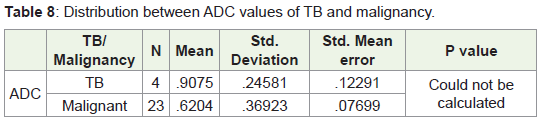
Since the number of TB cases in our study was only 4, statistically
significant comparison between ADC values of TB and malignancy
could not be obtained.
Discussion
Diffusion weighted imaging is an MRI technique which can be
readily incorporated into routine non contrast MR imaging protocol
with little additional scanning time 2. It offers useful information
about the cellularity of the lesion under study.
Spinal DWI is a relatively novel technique to assess vertebral
pathologies.
Lesions of the vertebra indicate bone marrow invasion. Normal
bone marrow contains significant fat which restricts the movement of
water molecules and hence shows diffusion restriction and low ADC
value. This is unlike in any other part of the body where the background
shows low ADC values. Hence any pathology (Benign or Malignant)
which infiltrates the marrow and displaces fat, shows less diffusion
restriction and more ADC values than the normal vertebra 3.
Our present study included 46 patients, out of which 23 patients
had benign lesions and 23; had malignant lesions of the vertebra.
The most common benign vertebral pathology was degenerative
change of the vertebral endplate, followed by infection, trauma and
hemangioma.
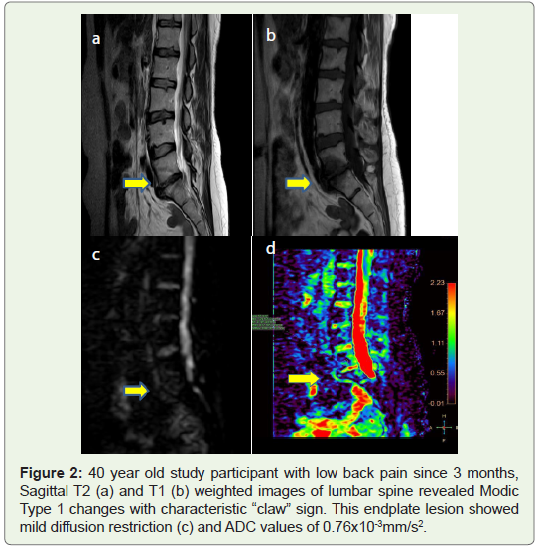
4 out of 6 patients showed fatty changes or Modic type 2 changes
at the vertebral endplate which appeared as widened disc space on fat
suppressed DW images. In Modic type 1 change, “claw” of diffusion
restriction was seen at the advancing border of proliferative process.
This finding is similar to study conducted by K.B Patil et al 4, in
which the “claw sign “on DWI was highly suggestive of degeneration
while diffuse DWI signal at the endplates with absence of claw sign ,
was suggestive of infection Figure 4.
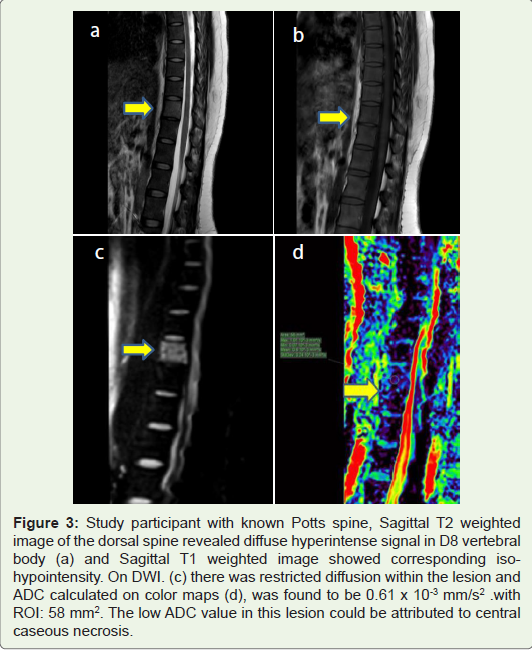
Among the infections, Tuberculosis (TB) was the most common.
ADC values for TB ranged from 0.65 to 1.2 x10-3 mm2/s. There was
overlap between ADC values obtained in TB and malignancy. This
finding is in accordance with studies conducted by Palle et al and
Balliau et al 5,6. According to Palle et al, false negative results can be
obtained when there is dense solid caseation within the vertebrae, and
in this situation overlap with ADC values of malignant lesions may
be seen. There were only 4 TB cases in our study hence, statistically
significant comparison between ADC values of malignancy and TB
could not be obtained Figure 3.
There were 4 cases of post traumatic vertebral fractures in our
study. The mean ADC value of these lesions was found to be 1.34 x
10-3mm2/s. This high ADC could be attributed to T2 hyperintense
edema associated with benign fractures as described in a study by
Masayuki et al. 7
The most common benign osseous tumor of the spine is
hemangioma. These tumors contain both fat and water and depending
on the predominant constituent, exhibit hyperintensity on T1 and T2
weighted images. In a study by Winfield et al8, the mean ADC value
of a typical vertebral hemangioma was found to be 1.085 x 10-3 mm2/s.
In our study, the mean ADC among hemangiomas was found to be 0.9
x 10-3mm2/s and is higher than that of malignant lesions. This finding
is in accordance with most studies where the ADC value of vertebral
hemangioma is higher than that of malignant vertebral lesions.
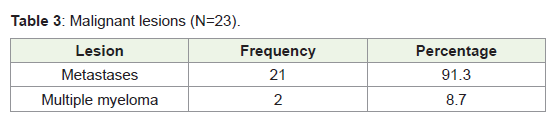
Among the malignant vertebral lesions, most common was
metastases. There were 2 cases of multiple myeloma in our study.
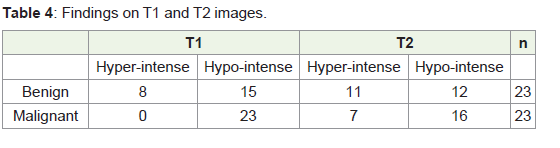
22 out of 23 malignant and 15 out of 23 benign lesions showed
hyperintense signal or diffusion restriction on DWI. Our statistical
analysis revealed Positive Predictive Value of 59.4 % and Negative
Predictive Value of 88% for malignant lesions.
This finding is in accordance with studies by Baur et al. 9,
who found that all but a few cases of metastatic fracture showed
hyperintensity relative to normal bone marrow. In fact Bauer et al.
found 100% accuracy in the diagnosis of malignant compression
fractures using DWI. Although more than 50% benign lesions were
hyperintense on DWI, the PPV for this finding was low (40.5%).
In the study by Masayuki Maeda et al 7, qualitative analysis
by DWI did not reveal a significant difference between benign and
malignant compression fractures. Qualitative analysis has a number
of theoretical disadvantages. One problem is that qualitative analysis
cannot completely eliminate the T2 shine-through effect. Another
problem is that the fraction of fatty marrow in normal vertebrae can
vary from patient to patient and vertebrae with a larger fraction of
fatty marrow would show DWI hyperintensity.
More promising results have been obtained by the quantitative
differentiation of benign and malignant lesions using ADC.
There was a statistically significant difference in ADC values
among benign and malignant vertebral lesions in our study. Mean
ADC of malignant lesions was found to be lower than that of benign
lesions. A cut of 0.73 x 10-3 mm2/s was found with sensitivity of 95.7%
and specificity of 85.2 % to distinguish between benign and malignant
lesions.
Our findings are in accordance with studies conducted by
Dietrrich et al where ADC values of malignant fractures or lesions
were typically between 0.7 and 1.3 × 10-3 mm2 /s and that these lesions
had lower ADC values compared to benign etiologies 10.
Recent study by Ajit Mahale et al also concluded that the mean
ADC of malignant lesions was lower than that of benign. Studies by
Shazia Naaz and E Balliu et al also had similar findings 11.
Among malignant lesions in our study, 2 patients had multiple
myeloma. The mean ADC of these lesions was 0.49 x10-3mm2/s.
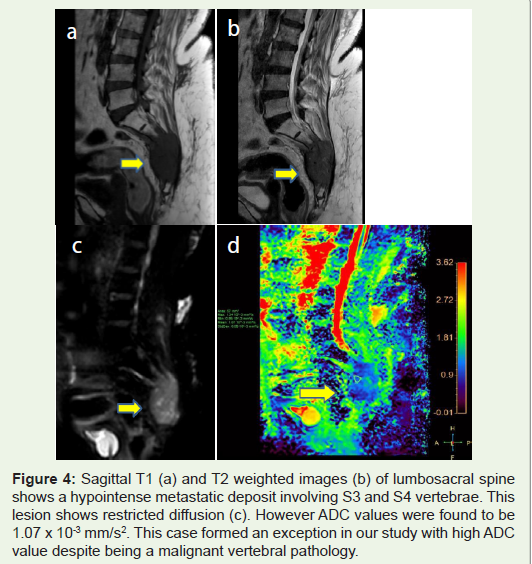
We had three false negative cases of high ADC value among
malignant pathologies, one was metastasis from renal cell carcinoma,
one from carcinoma lung and from vaginal carcinoma. In these
three cases conventional imaging and history were suggestive of
pathological collapse, but ADC values were on the higher side
(1.83,1.27 and 1.0×10-3 mm2/s). So conventional imaging is a must
and DWI should be an add-on sequence Figure 4.
Ours is the first study to standardize the area of ROI to achieve
accurate comparison between ADC values. Despite the false negative
cases, the sensitivity of 95.7 % of ADC to distinguish benign vertebral
pathologies from malignant pathology is promising.
Conclusion
Limitation
There were only 4 cases of TB spine in our study, thus statistically
significant comparison could not be obtained.
Our study included patients with known malignant lesions of the
spine and this represents a selection bias.
Recommendation
DWI is a rapid sequence with very little additional scanning
time and should be included in routine imaging of the spine.
ADC should be calculated in all patients with vertebral lesions
with standard post processing techniques.
Management of patients with TB and malignancy is different.
Hence additional studies to differentiate these entities via imaging
are the need of the hour.
References
Citation
Citation: Sriram R, Kashikar R, Desai SB. Qualitative and Quantitative Differentiation between Benign and Malignant Vertebral Lesions Using Diffusion Weighted MRI: A Prospective Study. Indian J Appl Radiol. 2023;9(1): 181.