Pictorial Essay
MDCT Evaluation of Coronary Artery Variants: Pictorial Essay
Kumar K*, Priyadarshini V, Dharan Venkatesh KA and Senthilnathan V
Department of Radio-diagnosis, Trichy SRM Medical college hospital & Research Centre. Irungalur, Trichy
*Corresponding author: Kumar K, Department of Radio-diagnosis, Trichy SRM Medical college hospital & Research
Centre, Irungalur, Trichy; E-mail: drmkrishnakumar@gmail.com
Copyright: © 2023 Kumar K, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 02/01/2023; Accepted: 07/03/2023; Published: 13/03/2023
Abstract
Objective: The purpose of this pictorial essay is to review the multi detector computed tomography (MDCT) coronary angiography appearance of
coronary artery variants [CAV]. Although CAV are relatively uncommon, familiarity with atypical anatomy and their clinical presentation may facilitate
appropriate diagnosis and management. This will be of immense help to the clinician planning interventional procedures like stenting, balloon dilatation, or
graft surgery particularly when there are secondary changes of calcification, plaque formation and stenosis.
Conclusion: Increasing the employment of MDCT in cardiac imaging may yield diagnostic information on congenital coronary artery variants not obtained
with invasive coronary angiography. Axial sections, multiplanar reconstructions, virtual angioscopy, and 3D volume-rendered images should aid within the
detection and improve the interpretation of such coronary variants, which might be of immense help to the clinician planning interventional procedures.
Keywords
Computed tomography coronary angiography; Coronary artery variants
Introduction
Coronary artery variants (CAV) are uncommon and most of
them are diagnosed incidentally during conventional coronary
angiography or MDCT coronary angiography performed for
other reasons and do not require any diagnostic workup, further
investigation or treatment..Although catheter angiography is an
efficient tool, it’s invasive and related to procedural morbidity (1.5%)
and mortality (0.15%) [1]. Because of its two dimensional nature,
catheter angiography has protection limitations and it cannot show
the link of aberrant vessels with the underlying cardiac structures [2].
The recent development of ECG gated MDCT coronary angiography
allows accurate and noninvasive depiction of coronary artery variants
of their origin, course, and termination.
Coronary Artery Variants
Illustrative Cases:
Case 1: 56 years old male with dominant Right coronary arterial
(RCA) system (Figure 1).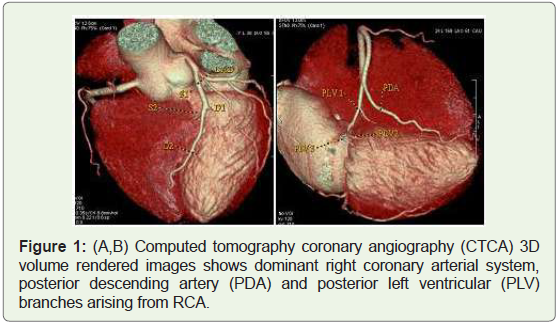
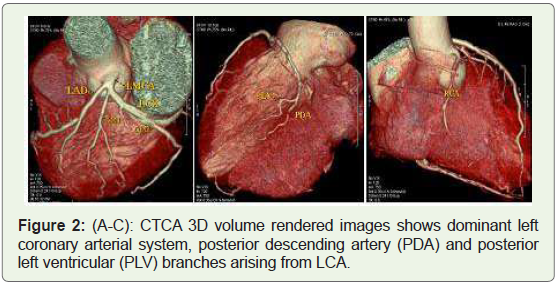
Case 2: 49 year’s old male with dominant Left coronary arterial
(LCA) system (Figure 2).
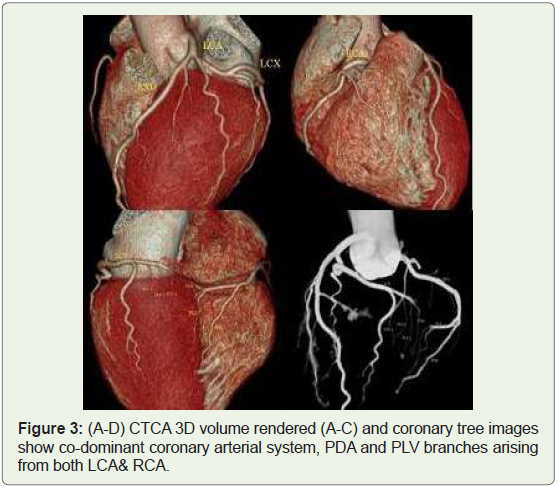
Case 3: 36 years old male with Co-dominant coronary arterial
system (Figure 3).
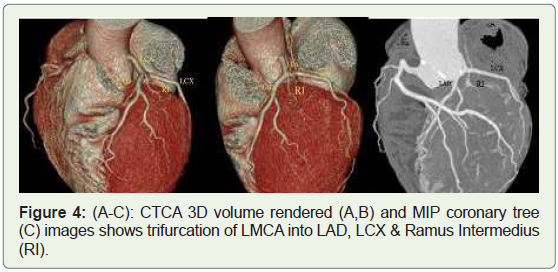
Case 4: 38 years old male with trifurcation of LMCA into LAD,
LCX & Ramus intermedius (Figure 4).
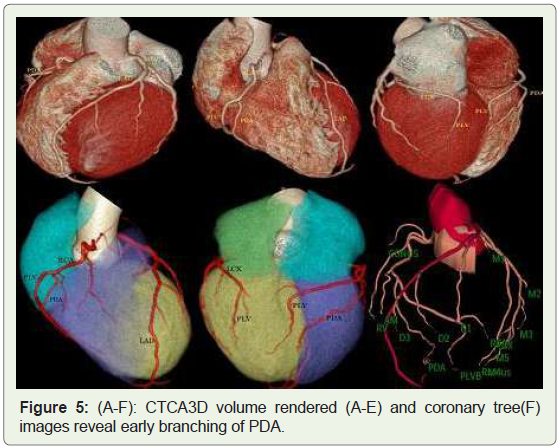
Case 5: 36 years old man with early branching of Posterior
descending artery (Figure 5).
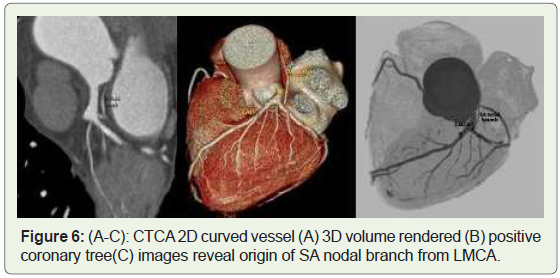
Case 6: 58 years old man with Sinoatrial (SA) node branch from
LMCA (Figure 6).
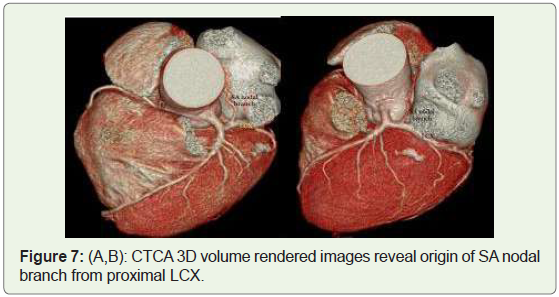
Case 7: 50-year-old man with SA node branch arising from LCX
(Figure 7).
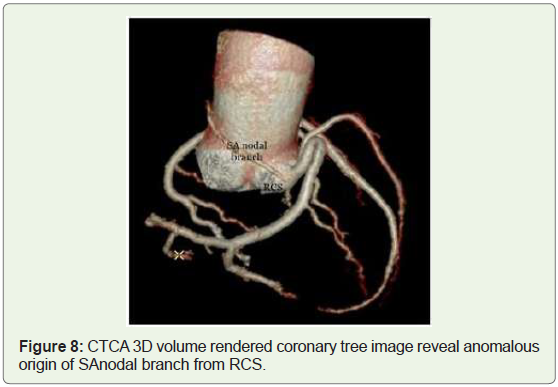
Case 8: 45 year old woman with SA node branch arising from
Right coronary sinus (Figure 8).
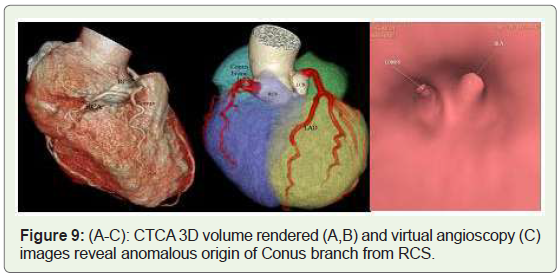
Case 9: 52 year old male with Conus branch from Right coronary
sinus (Figure 9).
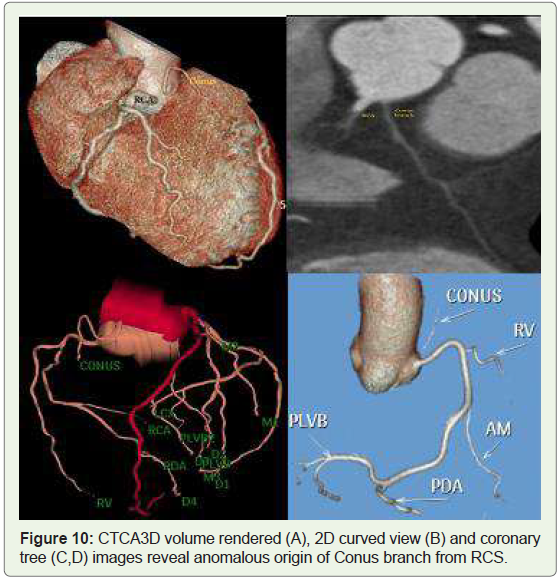
Case 10: 42 year old man with conus branch fromRight coronary
sinus (Figure 10).
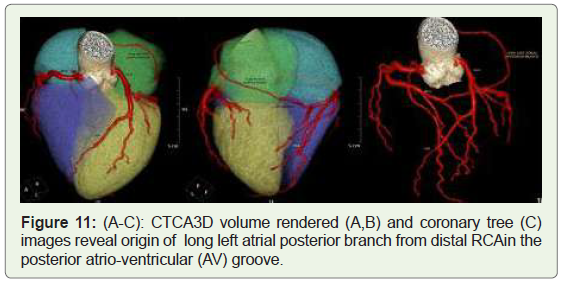
Case 11: old woman with left atrial posterior branch from
distal RCA (Figure 11).
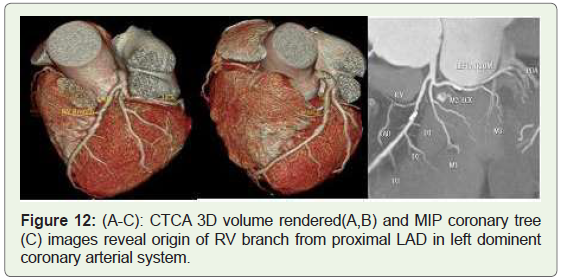
Case 12: 57 years old woman with Right ventricular branch from
LAD (Figure 12).
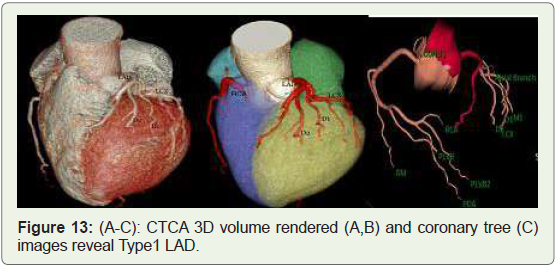
Case 13: 50 years old man with Type 1 LAD (Figure 13).
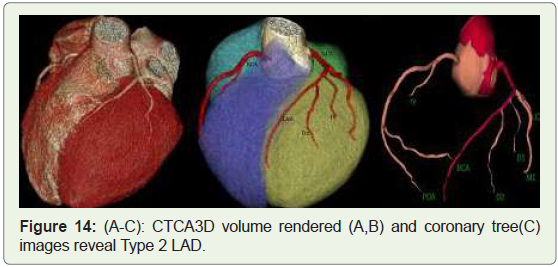
Case 14: 39 years old woman with Type2 LAD (Figure 14).
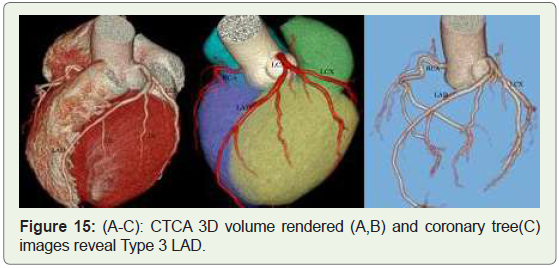
Case 15: 36 years old male with type 3 LAD (Figure 15).
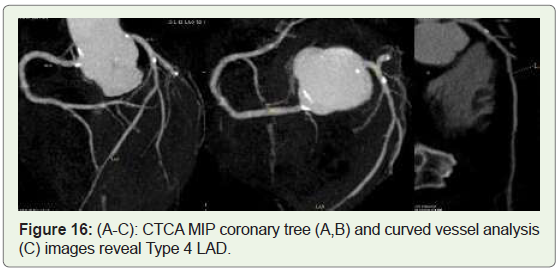
Case 16: 82 years old male with type 4 LAD (Figure 16).
Discussion
The coronary arteries arise from the aortic sinuses, clustering
towards the apex of the heart. Normally, there are three main coronary
arteries, the right coronary artery (RCA)which generally arises
from the right sinus of Valsalva (RSV) of the ascending aorta and
supplies the right side of the heart, left circumflex artery (LCX) and
left anterior descending (LAD), artery arising from a common stem,
the left main coronary artery (LMCA) which arises from left sinus of
Valsalva (LSV). Among these, the origin of the posterior descending
coronary artery (PDA) from either the right (70%) (Figure 1) or the
left (10%) (Figure 2) coronary artery defines the coronary dominance,
co-dominance (Figure 3) in 20% of cases, with the dominant artery
usually providing blood supply to the sino-atrial (SA) and atrioventricular
(AV) nodes, albeit with some exceptions.Other common
possible findings include trifurcation of the LMCA, with a Ramus
intermedius (in ≈20% of the cases) (Figure 4), distributing across a
variable portion of the lateral wall of the left ventricle [3].
Arteries supplying the left atrium (LA) are among the earliest
branches of the Left coronary artery, usually from the LCX, and
originate along the AV groove. Arteries supplying the right atrium
(RA) are among the foremost branches of the RCA after the conus
artery and originate along the right atrio-ventricular (AV) groove.
Arteries supplying the left & right atriumare generally classified into
the anterior, intermediate/marginal and posterior atrial branches [4].
Congenital coronary anomalies (CCA)may be defined as a
coronary pattern or feature that’s encountered in lower than 1% of
the general population.
In summary, we are able to divide the coronary feature in two
groups:
(1) Normal coronary anatomy, defined as any morphological
characteristics seen in > 1% of unselected sample. This group also
includes normal anatomical variants, defined as alternative and
comparatively unusual morphological feature observed in > 1% of
the population; and
(2) Anomalous coronary anatomy, defined as morphological
features found in < 1% of the population [5-7].
For several decades, these anomalous coronary arteries were
identified by conventional catheter coronary angiography. MDCT
coronary angiography has been accepted as the ideal system for
evaluation of patients with atypical chest pain due to its excellent
temporal and spatial resolution [1,8].
Magnetic resonance coronary angiography could be a noninvasive
method that doesn’t require the utilization of contrast
agents or ionizing radiation, and thus is superior compared to
cardiac CT angiography and conventional coronary angiography.
Its disadvantages are lengthy acquisition time and lower spatial
resolution [9].
Congenital coronary variants (CCV) refer to simple variations
within the structural anatomy. Some of the variants include
1. Left coronary dominance (10%) (Figure 2), Co-Dominance
(20%) (Figure 3), LMCA trifurcates (20%) into Ramus intermedius
(RI) (Figure 4), LAD & LCX [7],
2. Early branching of the PDA (early take off) from the RCA
(Figure 5) before the crux of the heart.
3. Duplication of branches, e.g., two PDAs getting in the septum.
4. Shepherd’s crook RCA-In this variant, the RCA has a normal
origin, but takes a tortuous and high course, immediately after the
origin. The prevalence of this variant is estimated of roughly 5%.The
shepherd’s crook isn’t clinically significant, but its presence may
complicate percutaneous interventions within the RCA [10].
5. Presence of a descending septal branch originating from the
RCA that supplies part of the basal interventricular septum [10].
6. SA nodal artery from LMCA (Figure 6), proximal LCX (Figure 7), distal LCX, distal RCA [11], or right coronary sinus (Figure 8). In
55% of human hearts, the RCA supplies the SA nodal artery within 2
cm of the coronary ostium and corresponds to the right anterior atrial
branch [12]. In 45% of cases, it originates within the first few mm
of the LMCA (Figure 6), and usually corresponds to the left anterior
atrial branch [13].
7. Origin of Conus branch from aorta or directly from the right
sinus of Valsalva (Figures 9,10) [13,14].
8. Left posterior atrial branch from Distal RCA (Figures 11).
9.Right ventricular branch from LAD (Figures 12).
Type-I – does not supply the left ventricular (LV) apex (Figures 13),
Type-2 – supplies a part of the apex (Figures 14) the remainder
being supplied by the right coronary
Type-3 – supplies the entire apex (Figures 15), and
Type-4 – wrap around apex, supplies the apex and >25% of the
inferior wall (wrap around LAD)(10) (Figures 16).
Variations in coronary anatomy are frequently seen in association
with structural styles of congenital cardiovascular disease like Fallot’s
tetralogy, transposition of the great vessels, Taussig-Bing heart
(double-outlet right ventricle), or common arterial trunk [14].
All forenamed variants are clinically benign and pose no threat to patients. At utmost, some of them, like the shepherd’s crook RCA,
may present technical challenges during coronary intervention for
other issues, due to difficulty in engaging angiographic catheters and
guides. In addition, a descending septal branch, which originates
from the RCA and supplies part of the interventricular septum, may
be used as a target for alcohol septal ablation in symptomatic patients
with hypertrophic obstructive cardiomyopathy whose basal septum
is supplied by this branch of the RCA. In addition, a descending
septal branch from the RCA may be an important source of collateral
retrograde filling of a proximally occluded LAD [15].
Conclusion
Increasing the employment of MDCT in cardiac imaging may
yield diagnostic information on congenital coronary artery variants
not obtained with invasive coronary angiography. Axial sections,
multi planar reconstructions, virtual angioscopy, and 3D volumerendered
images should aid in the detection and ameliorate the
interpretation of such coronary variants, which can be of immense
help to the clinician planning interventional procedures.
References
Citation
Kumar K, Priyadarshini V, Dharan Venkatesh KA, Senthilnathan V. MDCT Evaluation of Coronary Artery Variants: Pictorial Essay. Indian J Appl Radiol. 2023;9(1): 178.