Review Article
Intentional Ingestion, Insertion and Self- Embedding of Foreign Bodies - What a Radiologist Should Know
Chandel K, Kumar S, Bhatia V*, Debi U, Gorsi U and Sandhu MS
Department of Radio diagnosis, PGIMER, Chandigarh, India
*Corresponding author: Bhatia V, Department of Radio diagnosis, PGIMER, Chandigarh, India; E-mail: drvikasbhatia@
gmail.com
Copyright: © 2022 Chandel K, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 23/02/2022; Accepted: 05/04/2022; Published: 09/04/2022
Abstract
Background: Intentional foreign body presence in the human body can occur through various mechanisms and have variable clinical presentations.
Imaging plays an essential role in early diagnosis, localization, characterization and detection of any complications due to the presence of foreign bodies.
Purpose: To review the radiological findings in cases with foreign body insertion.
Material and Methods: A review of the cases with self-insertion of foreign bodies with radiological findings is illustrated. The role of different imaging
modalities and the radiologist is reviewed with appropriate clinical cases.
Results: Multiple cases with appropriate imaging modalities show the importance of radiologists in the early diagnosis and management of foreign
bodies. A comparative evaluation of various imaging modalities in appropriate settings is essential, as reviewed in the study.
Conclusion: Radiologists play a crucial role in diagnosing and treating patients with self-insertion of foreign bodies.
Keywords
Foreign body; Self-insertion; Radiologist
Introduction
The intentional presence of foreign bodies (FB) into the human
body can occur through various mechanisms such as self ingestion,
self-insertion and self-embedding behaviour. Clinical presentation
may vary from a slight injury to dreaded complications such as
perforation, obstruction, bleeding and abscess formation depending
on the location and nature of the foreign body. Imaging plays a vital
role in early diagnosis, localization, characterization and detection
of any complications due to the presence of foreign bodies [1].
Intentional presence of foreign bodies is not familiar; however, their
accurate diagnosis and management are of paramount importance.
Radiologist plays an important role in the early diagnosis, management and follows up of these patients. A variety of imaging
modalities such as radiographs, ultrasound and CT are employed for
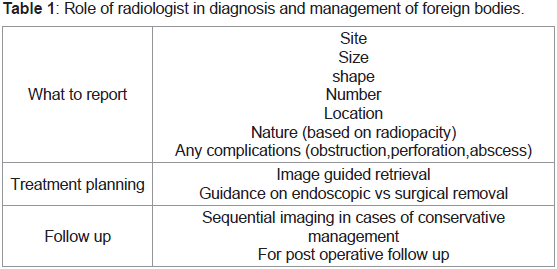
accurate management of these patients. When reporting these cases,
the foreign body should be described for location, number, size,
shape, nature based on attenuation and presence of complications
for optimal management. The role of radiologists in diagnosis and
management is summarized in Table 1.
The use of various imaging modalities in detecting these foreign
bodies with relative advantages and disadvantages is summarized in
Table 2.

Ultrasonography is used primarily for evaluating superficially embedded or radiolucent foreign bodies. It has the advantage of being
portable and lacking any radiation exposure. Both high-frequency
and low-frequency transducers are employed for superficial and deep
located foreign bodies [2]. Imaging may reveal posterior acoustic
shadowing in the case of wooden or stone foreign bodies and ring
down artefact in glass or metal foreign bodies [3].
Fluoroscopy may help in real-time visualization of oesophagal or
diaphragmatic motility; however, its role is limited.
CT is the investigation of choice for these cases to localize and detect complications [4]. On CT imaging, wooden foreign bodies
usually mimic fat or air with negative Hounsfield units (HU).
These may show water attenuation due to their porous nature with
an ability to absorb water with time. The CT attenuation values for
plastic bodies are around 100 to 500 HU, stone foreign bodies more
than 1,000HU, glass bodies from 500 to 2,000, and metallic bodies
show the highest values, usually more than 3,000 HU. Streak artefacts
are common in metallic foreign bodies, while no artefacts are seen in
glass or stone foreign body cases [5-8].
A summary of various foreign bodies and key diagnostic features
on various modalities is summarized in Table 3.
Intentional foreign body ingestion:
Intentional foreign body ingestion is commonly seen in adults
suffering from substance abuse or depressive disorders. In some
cases, it is sometimes done for illicit drug trafficking using balloons
or plastic [9,10]. In most cases, the foreign body can pass down the
intestinal tract without any significant complication and hence no
intervention is required. Few may require endoscopic or surgical
intervention [11].Clinical presentation depends on the location and nature
of the foreign body, organ involved and presence of associated
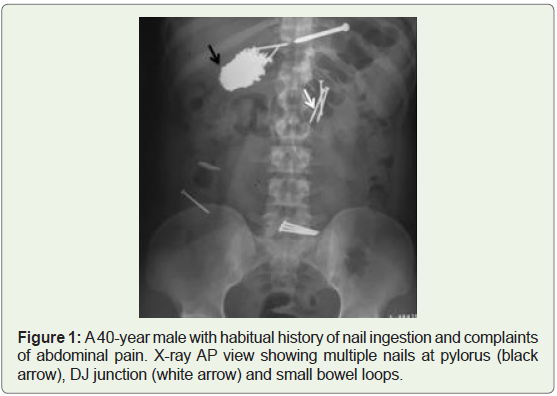
complications. The most common location for ingested foreign body
impaction is in the upper third of the oesophagus. Other locations are
at the level of the aortic arch, left main bronchus, or gastroesophageal junction, pylorus, C-loop of the duodenum, the duodena-jejunal
junction (Figure 1), ileocecal valve and rectosigmoid [12].
An AP and lateral radiograph scan detect radio-opaque foreign
bodies and demonstrate the number, location, size, shape of the
foreign bodies ingested or any complication such as perforation or
obstruction [13].
CT is the imaging of choice in these cases for accurate delineation
of the foreign body and associated complications like perforation,
fistula or abscess. Endoscopic or surgical interventions can be
planned after imaging or a conservative approach with sequential
imaging until the passage of the foreign body can be done [14-15].
Intentional insertion of foreign bodies into body orifices (Polyembolokoilamania):
The self-insertion of variable objects characterizes
Polyembolokoilamania into body orifices such as the rectum, vagina,
urethra. Multiple factors have been implicated for such tendencies,
including autoerotic stimulation, psychiatric disorders and substance
abuse. Diagnosis is usually delayed due to self embarrassment or
neglect and can lead to potential complications such as bowel injury
or perforation. A multidisciplinary approach with radiologists,
surgeons and psychiatrists is required for optimum diagnosis,
management and prevention of relapse. Patient presentation depends
on insertion site and foreign nature and may include pain, dysuria,
and hemorrhage [15,16].An AP and lateral X-ray should be obtained to demonstrate
the shape, size, orientation, location, and type of the foreign body.
Before a digital rectal examination, imaging should be conducted
as a safety precaution to prevent provider injury from sharp foreign
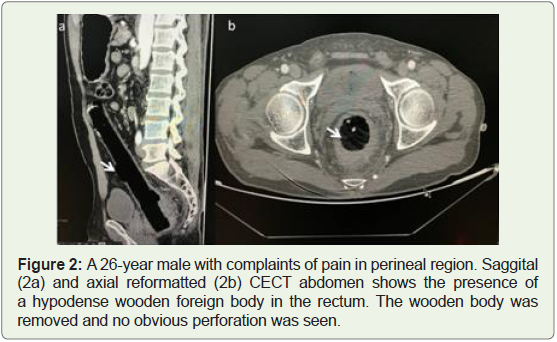
bodies. CT isthe imaging of choice in radiolucent foreign bodies
and demonstrates complications such as perforation or abscess
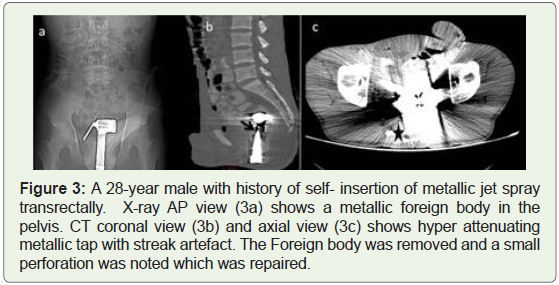
formation (Figure 2). Metallic foreign bodies may show many streak
artefacts rendering limited visibility for assessment (Figure 3). For
genitourinary radiolucent foreign bodies, Ultrasonography has been
shown to have high sensitivity for detecting foreign bodies in the
bladder [17].
Self-embedding:
Self-embedding is a rare underreported medical entity with the
deliberate injury of body tissue by inserting a foreign object. Cases
have been reported with foreign bodies embedded in limbs, abdomen,
chest or cranium (Figure 4) [18,19].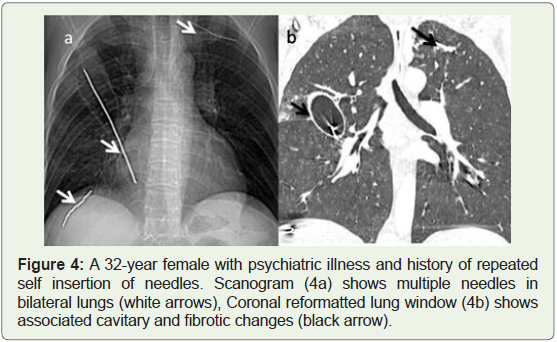
Usually, these cases have underlying psychiatric diseases such
as post-traumatic stress disorders or borderline personality traits.
These patients are more likely to commit suicide [20]. Radiologist
plays a crucial role in early diagnosis and radiological modality
guided or surgical removal of foreign bodies. Plain radiographs are
usually sufficient to diagnose the size, number, location, and foreign
object type. USG has proved to be a critical tool for diagnosing non
radiopaque foreign bodies embedded in the skin and subcutaneous
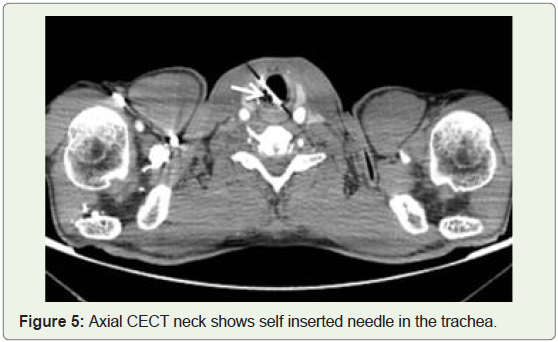
regions using a high-frequency transducer. CT is the investigation
of choice for deeply embedded foreign bodies for localization and
detects complications such as perforation, abscess or sinus formation
(Figure 5) [18-20].
Summary
Radiologists play a crucial role in the diagnosis, management
and follow up of these patients. The radiologists need to utilize the
optimum imaging modality depending on the type and nature of the
foreign body and detect early complications. A multidisciplinary team
effort is required for adequate management and prevention of relapse
by addressing the underlying psychiatric disorder in these patients.
References
Citation
Chandel K, Kumar S, Bhatia V, Debi U, Gorsi U, et al. Intentional Ingestion, Insertion and Self-Embedding of Foreign Bodies - What a Radiologist Should Know. Indian J Appl Radiol. 2022;8(1): 172.