Case Report
Fibromatosis of the Male Breast: Role of Dynamic MRI
Issar P1*, Ravindranath M2, Gupta P3 and Issar SK4
1HOD, Department of Radiodiagnosis, J.L.N Hospital and Research center, Bhilai, India
2HOD, Department of Pathology, J.L.N Hospital and Research center, Bhilai, India
3Senior Consultant, Department of Surgery, J.L.N Hospital and Research center, Bhilai, India
4Executiove Director, J.L.N Hospital and Research center, Bhilai, India
*Corresponding author:Issar P, Department of Radiodiagnosis, J.L.N Hospital and Research center, Bhilai - 490009,
Chhattisgarh, India; Tel - +91 9407983540 Email: pratibhaissar@gmail.com
Copyright: © 2022 Issar P, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 10/08/2021; Accepted: 11/01/2022; Published: 15/01/2022
Abstract
Fibromatosis of the breast is a non-metastasizing benign, but locally invasive stromal tumor, accounting for less than 0.2% of all primary breast lesions
and is formed by proliferation of fibroblastic and myofibroblastic cells. Mammary fibromatosis in men is extremely rare and may mimic primary breast
malignancy. We report a case of breast fibromatosis in a 52-year old male, where magnetic resonance imaging (MRI) was performed, which was showing
some salient features by which it can be distinguished from breast carcinoma and confirmed on histopathology and Immunohistochemical (IHC) examination.
Keywords
Fibromatosis; Mammography; Ultrasound; Magnetic Resonance Imaging
Case Report
We report a case of a 52-year old male presented with the chief
complaint of a slowly progressive painless left breast lump for one
year. Clinical examination revealed a firm painless swelling in the
upper outer quadrant of the left breast with no palpable lymph nodes
and nipple retraction. Family history was non-contributory and there
was no history of trauma or surgery.
On mammography (Alpha RT-GE), an irregular shape, noncalcified
high-density mass with spiculated margins seen in the left
breast, in the upper outer quadrant, posterior depth and classified as
BIRADS 4C lesion. At the ultrasound (Samsung RS 80A), the mass
was seen as an irregular hypoechoic mass with spiculated margins
and posterior acoustic shadowing suggestive of malignant lesion
BIRADS 4C. There was no involvement of pectoral muscle and the
axilla was normal.
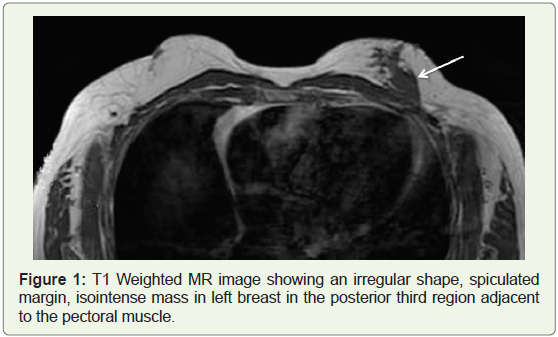
MRI (GE Signa Excite, using a dedicated 8 channel breast coil) was performed to delineate tumor extent and preoperative planning.
It showed an irregular shaped mass with spiculated margins in the left
breast measuring 3.5x 1.7x 2.5cm appearing isointense to muscle on
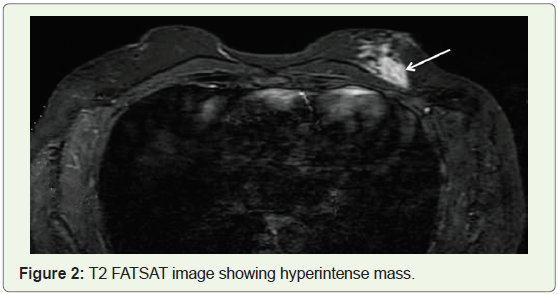
T1 Weighted image (Figure 1), hyperintense on T2, and T2 FAT SAT
images (Figure 2). The mass was seen separate from the pectoral muscle
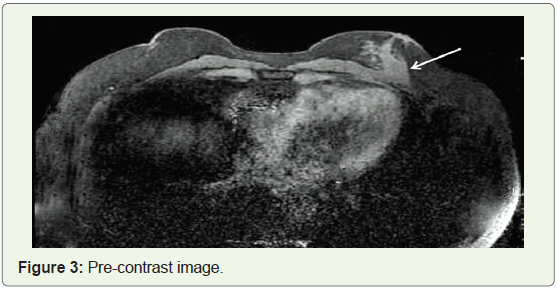
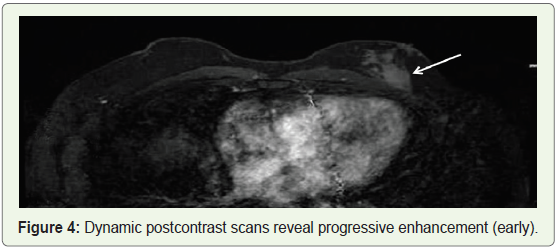
and fascia. Pre contrast image (Figure 3). Dynamic postcontrast scans
reveal progressive homogenous enhancement (early, Figure 4) and
consistent with type I kinetic curve (delayed image, Figure 5). No
evidence of lymphadenopathy was noticed. On Diffusion-weighted
imaging (DWI), restriction with an ADC value of 1.47e -09 was seen.
Diffuse glandular type of gynecomastia of left breast was noticed.
The right breast was normal. Based on MRI possibility of BIRADS
4C lesion was given by looking into its morphology. Sonographic
guided core biopsy of the mass was performed by 14 G trucut needle,
demonstrating a low-grade myofibroblastic proliferation along
with spindle cells consistent with breast fibromatosis. The patient
underwent a simple mastectomy. On gross examination 4.5 x 3x2.5 cm tumors was identified in the upper outer quadrant. Fibrous spicules
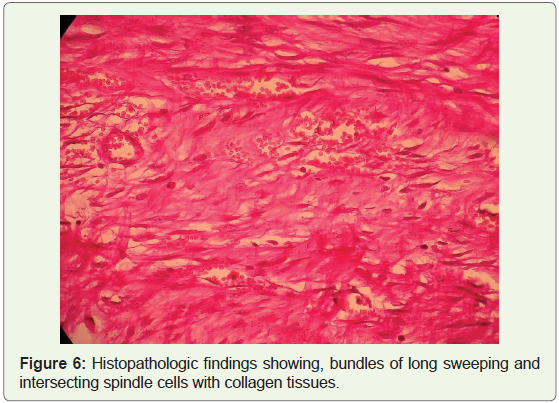
were seen radiating from the tumor. Histopathological sections
studies showed bundles of fibro- collagenous tissue consisting of
benign spindle cells, with sparse mitosis and no evidence of necrosis
(Figure 6). Overlying skin, nipple-areola, and deep surgical margins
were free of infiltration.

Immunohistochemistry was negative for pan-cytokeratin, desmin,
S-100, CD 34. Vimentin and smooth muscle actin were positive with
a Ki67 index of less than 1%. Estrogen (ER) and progesterone (PR)
receptors were absent. Based on histopathology and IHC a diagnosis
of breast fibromatosis was made.
Discussion
Mammary fibromatosis is a rare entity, accounting for less than
0.2% of all breast tumors. The patient’s age ranges from 13 to 83 years
with the vast majority of cases occurring in women. Very few cases
have been reported in men [1].
The etiology of this lesion is not well understood, but an
association with Gardner’s syndrome has been reported. Additional
associations include familial multicentric fibromatosis, silicone and
saline breast implants, incidental, and surgical trauma. Fibromatosis
may arise from the pectoralis muscle or fascia or the mammary tissue.
Clinically, desmoid tumors of the breast present as a firm painless,
movable mass, with or without skin retraction and dimpling. Nipple
retraction is seen if the tumor is close to the nipple. Nipple discharge
and palpable lymphadenopathy are not associated with breast
fibromatosis [2].
Multiple imaging modalities have been used to characterize
breast fibromatosis, however, the final diagnosis is based on
Histopathological findings. On mammography desmoid tumors
present as high-density non-calcified lesions, with irregular shape and spiculated margins mimicking breast carcinoma. On Ultrasound,
breast fibromatosis frequently appears as a poorly defined, hypoechoic
mass with a thick echogenic rim and a posterior attenuation. It is
not associated with adenopathies. Ultrasound Elastography was not
found to be useful in discriminating between mammary fibromatosis
and malignant tumors in the breast, because the composition of
mammary fibromatosis lesion makes it stiffer than normal breast
tissue and may lead to a false diagnosis of malignant tumor based on
the elastographic result [3].
Breast fibromatosis on MRI appears as irregular, hypointense
to isointense on T1 weighted images, and hyperintense on T2-
Weighted images. The lesion usually shows progressive or plateau
type of enhancement on the post-contrast scan as compared to rapid
enhancement of the malignant lesion. Our case also had T1 isointense
and T2 hyperintense irregular mass with progressive contrast
enhancement. MRI is useful to show chest wall involvement, which is
important for surgical planning [4,5].
Cytologic examination by fine-needle aspiration is usually
not diagnostic. Definite diagnosis is made by diagnostic surgical
biopsy. Histologically the lesion is composed of bundles of long
sweeping and intersecting spindle cells with collagen deposition.
Mitotic figures are rare. Differentials include scar or keloid,
nodular fasciitis, schwannoma, leiomyoma, solitary fibrous tumor,
spindle cell lipoma, myofibroblastoma, myoepithelioma, low-grade
fibromyxoid sarcoma, and low-grade fibrosarcoma. The presence of
spindle cells admixed with epithelial cells should raise the possibility
of fibroadenoma, phyllodes tumor, or metaplastic spindle cell
carcinoma. In fibromatosis, myoepithelial markers are absent [6,7].
Immunohistochemically, fibromatosis exhibits positivity for
smooth muscle actin and vimentin and negativity for cytokeratin,
estrogen, progesterone, and androgen receptors. Desmin is rarely
positive, whereas S100 and CD 34 are usually negative [7,8].
Fibromatosis in the breast differs from fibromatosis arising in
another part of the body due to its hormone receptor profile. Although
30 % of extramammary fibromatosis is positive for ERs, only one of
the previously reported cases of mammary fibromatosis expressed
hormonal receptors. A positive reaction of ER and PR in the spindle
cell neoplasm of the breast might help exclude fibromatosis from its
differential diagnosis.
Fibromatosis is a benign entity without metastatic potential but
carries a significant risk for local recurrence. The breast is an unusual
location for the development of this tumor, with relatively few cases
reported in the literature. Although it does not metastasize, it is
frequently locally aggressive and is proven to recur (up to 35%) even
after complete surgical excision with clear margins. Skin retraction is caused by fibrous tissue contraction as compared to the desmoplastic
reaction which is similar to tethering associated with malignancy.
The clinical presentation and the radiological appearance of breast
fibromatosis are highly suspicious for breast carcinoma. The tumor
is best differentiated by histopathology and immune histochemistry
study.
Treatment consists of wide local excision with clear margins,
other options include radiation therapy and chemotherapy in patients
who are not surgical candidates [9,10].
To conclude male breast fibromatosis is a rare, locally aggressive,
benign breast tumor that mimics breast cancer on mammography
and ultrasound but MRI can help in its diagnosis, by showing benign
nature, which can be confirmed with an appropriate histopathology
and immunohistochemistry study.
Acknowledgment
We would like to thank Mr. Arnesh Kumar Issar for his help with
the Manuscript preparation, review, and submission.
References
Citation
Issar P, Ravindranath M, Gupta P, Issar SK. Fibromatosis of the Male Breast: Role of Dynamic MRI. Indian J Appl Radiol. 2022;8(1): 170.