Case Report
Jejunojejunal Intussusception - A Rare Case in Adults
Shailaja P*
Department of Radiodiagnosis, Andaman and Nicobar Islands Institute of Medical Sciences, India
*Corresponding author: Shailaja P, Department of Radiodiagnosis, ANIIMS and GB PANT Hospital, Port Blair - 744104,
India; Tel: 9434284322; Email: pshailaja@gmail.com
Copyright: © 2021 Shailaja P. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 23/07/2021; Accepted: 07/10/2021; Published: 09/10/2021
Abstract
Intussusception is a rarely encountered cause of intestinal obstruction in adults. It is a clinically difficult diagnosis to make since the symptoms can be
very variable, unlike the pediatric presentation triad of abdominal pain, palpable abdominal mass and blood stained stool. A majority of adult intussusceptions
(AI) are secondary to a definable lesion. A 48 year old woman with three months history of intermittent colicky pain underwent CECT scan and was found
to have small bowel intussusception with a fat density rounded lesion at the lead point. Exploratory laparotomy revealed jejunojejunal intussusception
secondary to a lipoma situated 40 cm distal to the duodenojejunal junction, which was treated by with segmental intestinal resection. CT scan proved to be
the decisive factor for surgical treatment in an undiagnosed case of abdominal pain and provided the correct diagnosis pre-operatively.
Introduction
Intussusception is defined as telescoping of a segment of the
gastrointestinal tract into an adjacent segment. Intussusception is
a rare cause of intestinal obstruction in adults, accounting for only
1% of all obstructive causes, and 5% of all intussusceptions. It is a
clinically difficult diagnosis to make since the symptoms can be very
variable, unlike the pediatric presentation triad of abdominal pain,
palpable
abdominal mass and bloody stool. A majority of adult
intussusceptions (AI) are secondary to a definable lesion. Lipomas are
a cause of AI, commonly found in the ileum. This is a report of a rare
case of lipoma in the jejunum, causing jejunojejunalintussuception.
Narrative
A 48-year old woman presented with more than three months’
history of intermittent colicky pain in the abdomen. Clinical
examination revealed a vague lump in the left side of abdomen.
Ultrasound examination done in a private diagnostic centre reported
a bowel related mass, with a possible diagnosis of typhlitis. She
was sent for a CT scan to our department confirms the diagnosis.
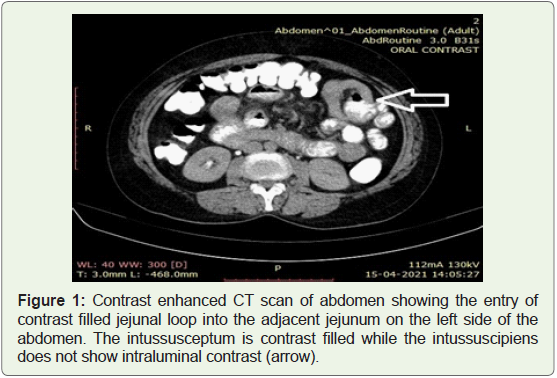
CT scan was performed after administration of oral contrast, with
images acquired before and after 80ml of non-ionic intravenous (IV) contrast injection, on a Siemens Emotion 16-slice CT scanner (Figure 1). Intussusception was noted with a segment of contrast filled small
bowel loop (jejunum) herniating into the adjoining small bowel loop
in the umbilical quadrant. A 2.8cm x 2cm x 1.8cm fat density smooth
lesion (HU -70 to -90) was seen in the internal loop (intussusceptum),
s/o mesenteric /luminal lipoma. No post-contrast enhancement
was seen in this fat-density lesion. The proximal small bowel loops were prominent and edematous. Exploratory laparotomy revealed
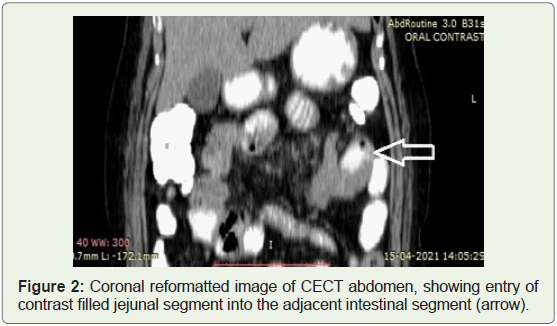
jejunojejunal intussusception secondary to a lipoma situated 40 cm
distal to the duodenojejunal junction, which was successfully treated
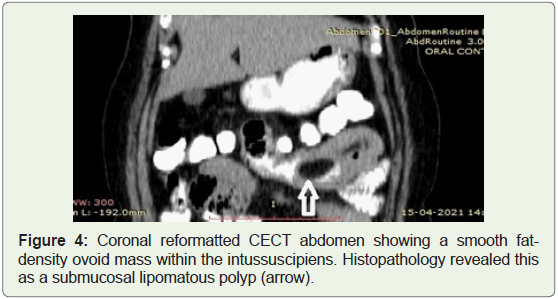
by with segmental intestinal resection (Figure 2). Histopathology
revealed features consistent with a submucosal lipomatous polyp
with focal ulceration covered with fibrinous exudates.
Discussion
Adult intussusception (AI) is a rare cause of intestinal obstruction,
unlike pediatric intussusception. In adults, intussusception makes up
only 1% of all intestinal obstructions whereas in children, it is the
leading cause of obstruction [1]. Unlike the pediatric population where
a definable cause of intussusception is not found in the majority, the
vast majority of AI are secondary to a benign or malignant tumour
[1-4]. Intussusceptions can be classified as idiopathic and secondary
or lead point intussusceptions, and the secondary intussusceptions
as benign and malignant enteric, ileocolic, colonic, depending on the
nature of the lead point lesion. When intussusceptions do occur in
adults, the most common type is enteroenteric, followed by ileocolic
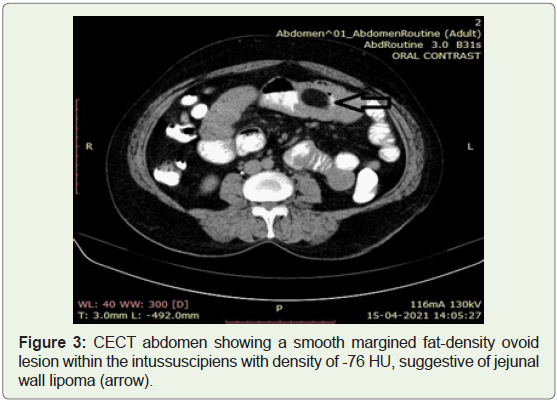
and colonocolic. The most common benign lead-point in AI is a
gastrointestinal lipoma. 50% of them are seen in the ileum (50%)
while jejunum is the least common (Figure 3). The maximum age
of incidence is the 6th-7th decades, and gender wise, commoner
in females. Malignant degeneration has never been reported. The
clinical presentation in adults can be very varied, thus making this a
difficult condition to diagnose.
Pre-operative diagnosis of AI, and diagnosis of the lead point, if
any, requires the use of imaging. Plain radiographs of the abdomen
are usually normal in adults, unlike the pediatric population, in
which there may be findings of a soft tissue mass surrounded by a
crescent of gas (air crescent sign), and accompanying signs of distal
small bowel obstruction in the form of multiple air-fluid levels [5].
Ultrasound is usually the first investigation but has a sensitivity
of only up to 60% due to bowel gas masking the lesion and high
operator dependency (Figure 4). The diagnosis of intussusception is
made based on the findings of the “target” sign, the “doughnut” sign
when the transducer is oriented transversely to the intussusception,
the “trident” sign with the transducer position longitudinal, and the
“pseudo kidney” sign in oblique visualisation [6-8].
Computed tomography is the radiological investigation of choice
for the diagnosis of intussusceptions. Further, CT can indicate bowel ischemia with indirect signs like the presence of intraperitoneal fluid,
and also the status of fluid or gas collection in the intestinal wall [9].
Submucosal lipomas can be diagnosed if a smooth well-circumscribed
fat density mass (-50 to -100 Hounsfield Units) is detected within
the lumen of the bowel or intussuscipiens. High sensitivity and
specificity of CT scan in the diagnosis of intussusceptions has been
well documented, with 71.4%-87.5% sensitivity and 100% specificity
reported as verified by the subsequent surgery. [10,11]
Differential Diagnosis
Majority (about 90%) of adult intussusceptions have a lead point,
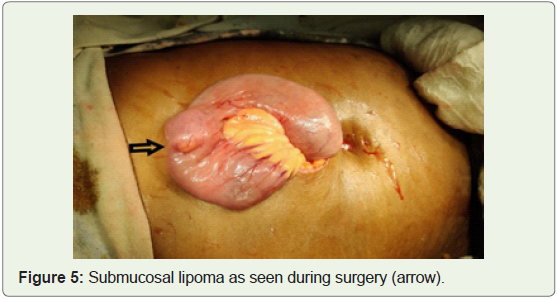
i.e. a definable pathological abnormality. Generally, the majority of
small intestinal lead points are benign lesions, for example, benign
neoplasms, inflammatory lesions, Meckel’s diverticuli, appendix, adhesions, and intestinal tubes (Figure 5). About 30% of reported
cases in the small intestine are malignant lesions (either primary or
metastatic). In contrast, large bowel intussusception is more likely to
have a malignant etiology and represents up to 66% of the cases.
Other possible differentials to be considered in adults include:
• Primary bowel tumor – will not have a typical ‘target-like’ or
‘doughnut’ sign on ultrasound
• Metastases and lymphoma – CT scan will reveal the absence
of telescoping of bowel into the adjacent loop
Intestinal lipoma (without intussusception) – though the typical
fat density lesion can be visualised on USG and CT scan, typical
intussusception signs can be precluded on imaging
Meckel diverticulum
Endometriosis
Conclusion
Adult intussusception is a rare pathology, requiring a high
index of suspicion for correct and timely diagnosis. CT scan and
ultrasonography are the mainstay of diagnosis in today’s medical
world. Gastrointestinal lipomas as a cause of AI can be detected preoperatively
with a high sensitivity and specificity. Surgical resection
after reduction is recommended for benign lesions, whereas enbloc
resection without reduction is the agreed-upon procedure
for malignant lesions. Therefore, an abdominal CT scan is highly
recommended for all cases of adult intestinal obstructions. In our
case, CT scan proved to be the decisive factor for surgical treatment in an undiagnosed case of abdominal pain and provided the correct
diagnosis pre-operatively.
References
Citation
Shailaja P. Jejunojejunal Intussusception - A Rare Case in Adults. Indian J Appl Radiol. 2021;7(1): 167.