Case Report
Right Ectopic Cervical Thymus-A Rare Case Report
Vasudha N1* and Balkrishna K2
1Department of Anatomy, University Kasaba Bawada, India
2Department of Radiology,Alliance Hospital, Ichalkaranji and Eureka Diagnostic centre, India
*Corresponding author: Vasudha N, Department of Anatomy, D. Y. Patil Medical College, Dr. D.Y.Patil Education Society;
University Kasaba Bawada; Kolhapur, India; Tel- 9665730990; Email: dr.vasudhanikam@gmail.com
Copyright: © 2021 Vasudha N, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 06/03/2021; Accepted: 13/07/2021; Published: 16/07/2021
Abstract
Cervical ectopic thymus is rare cause of solid neck masses and are the silent majority. Cervical ectopic thymus many times diagnosed incidentally and
mistaken for neoplasm. Here we are reporting a case of 45 years old female presented with a history of slowly enlarging mass on the right side of the neck
in paratracheal region. The patient complained of pain at the site of the enlarged mass. Thyroid function tests were within normal limits. On ultrasonography,
right cervical ectopic thymus was revealed in the paratracheal region in relation to right side of thyroid gland.
Keywords
Neck mass; Ultrasonography; Ectopic Thymus; Neoplasm; Aberrant thymus; Thymus hyperplasia
Introduction
The thymus is first lymphoid organ, which grows substantially
in infants [1,2]. Cervical ectopic thymus as neck lump is rarely
considered in the differential diagnosis of neck swellings. It is, a
prevailing anomaly identified incidentally at autopsy [3]. However,
the presence of ectopic thymus tissue is acclaimed pathological
essence along the embryological descending track in the neck [4].
Ectopic thymic tissue may come across anywhere along the path
of descent of the thymopharyngeal ducts (e.g-cervical, retrocaval,
posterior mediastinal) [5].
Ectopic thymic tissue adjoining to the thyroid gland is a rare
entity and completely incidental finding either preoperatively or
at autopsy [6]. Thymic remnants when found in the neck, they are
unusual cause of patient presentation at the clinic and the diagnosis is
difficult to accomplish in a pre-surgical walk up [7].
Here we report a case of adult female with ectopic cervical thymus
and was an incidental finding which encountered in association with
neck mass.
Case Report
A 45 years old female was referred for radiological scanning for
the swelling in the neck.
Clinical Examination
A patient was afebrile with all parameters normal. She complained
of the mass in the neck on the right side since last 4 months and was
increased since last one month.On palpation of neck revealed soft,
tender and fluctuating mass, which was approximately 3 to 4 cms in
diameter; below the right angle of the mandible and anterior border
of upper 1/3rd of right sternocleidomastoid muscle. It was difficult to
portray exact outline of the neck mass. The overlying skin showed no
discolouration and there was no intraoral swelling noted.
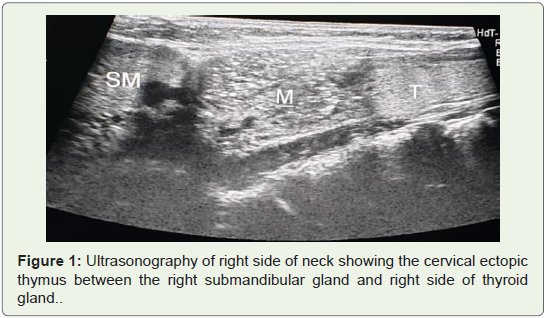
The patient was then scanned on ultrasonography, which
revealed an enlarged lymph node on the right side. During scanning
incidentally detected a mass (0.6x0.5x0.2cm) on right paratracheal
region, which was situated between right submandibular gland and
right side of thyroid gland (Figure 1).
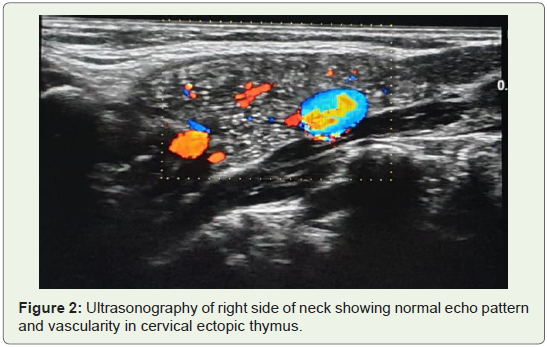
The mass showed homogeneous echo pattern similar to normal
thymic tissue with normal vascularity (Figure 2) with no other
abnormalities.
No other lymph nodes were palpable and were noticed on USG.
The thyroid function test was within normal range. Hence, ectopic
cervical thymus was identified. The patient was sent to the surgery
department for further management of necrotic lymph node. Our
case is unique in that ectopic cervical thymus was seen on the right
paratracheal region. This has been rarely documented in the literature.
Discussion
Ectopic and accessory thymic remnants can be found anywhere
along the course of migration of the thymo-pharyngeal duct from the
3rd and 4th branchial arches to the superior mediastinum. In case of
ectopic thymus, the mediastinal thymus may be small orabsent [1]. In
our case, it was absent.
Cervical ectopic thymus is an uncommon cause of neck lump
and is usually described in sporadic case reports [3]. Tovi and Mares
reviewed 68 reported cases of ectopic thymus in 1978 [3,8]. Ten years
later in a collective review of 91 cases by Nowak et al, 76 presented
as neck masses while the rest were mediastinal in location [3]. In
our case, ectopic thymus was situated in neck on the right side of the
thyroid gland.The majority of the cases are seen between 2 to 15 years
of age, with a male preponderance [9]. In our case, it was incidentally
detected in 41 years old female.
Ectopic thymic masses are located along the pathway of descent
of the thymus. Hence it could be sited anywhere from the angle of
the mouth or base of the skull to the superior mediastinum. These
thymic vestiges are relatively common anomalies but since they are
asymptomatic they are detected occasionally [10]. In our case, ectopic
thymus was present on right paratracheal region, below the right
angle of the mandible between right submandibular gland and right
side of thyroid gland.
Cervical ectopic thymus is often asymptomatic with only 10% of
patients being symptomatic in the form of pain or pressure symptoms
like strider, dyspnoea, dysphagia and hoarseness of voice [11].
However, in our case the neck swelling was due to necrotic lymph
node while the ectopic cervical thymus had normal echogenicity.
Most cervical thymus are unilateral and for unknown reasons are
more commonly reported on left side and in male patients they have
been known to occur as high as the mandibular angle and as low as
the thoracic inlet and superior mediastinum. Thymic masses in the
trachea, pharynx and at the base of skull have been reported [12]. In
our case, also it was unilateral and presented on the right side in a
female patient. It was high upto the right mandibular angle.
The characteristic appearance in an ultrasound scan is the finding
of a remnant between the thyroid gland and the neck muscles with
multiple linear structures and echogenic foci that give it a starry sky
appearance [8]. Probably due to the presence of Hassall’s corpuscles.
This is however variable as it has been shown that the thymic
parenchyma may sometimes be hypoechoic and less characteristics.
In our study ectopic cervical thymus showed normal homogeneous
echo pattern on USG with no any significant changes in the tissue;
however at superior mediastinum thymic tissue was not traceable.
Embryological Basis
Knowledge of the embryologic development of the thymus is
essential in understanding the pathogenesis of the aberrant / ectopic
thymus [4]. The primordial thymus begins to appear early in the
6th week of fetal life from the ventral wing of the third pharyngeal
pouch on each side of the most cephalad portion of the thymus
are derived from the fourthpharyngeal pouch. The proliferation of
endodermal calls within the outpouchings gives rise to paired solid
structures. By the 7th week of generation, the thymic primordia lose
their connections with the pharyngeal wall & join in the midline.
A mesenchymal capsule surrounding the developing thymus and
maintains the organ in close association with the partial pericardium.
Together these structures descend to their final anatomic positions in
the anterior mediastinum.
The medial caudal migration pathway forms the thymophalyngeal
tract, which runs from the angle of mandible to the manubrium
of the sternum bilaterally. Normally this tract involutes by the
completion of development; however, thymic vestiges may persist
anywhere along its course. Lymphocyte invasion occurs at 10 week
of gestation, whereas subsequent endodermal regression from the
Hassall’scorpuscle [12].
Cervical thymic anomalies may occur because of an arrest in
medial caudal migration of thymic primordia and persistence of remnants of thymopharyngeal tract [8]. In case of an undescended
thymus due to migrationarrest, only half of the normally bilobed
thymus is present in the mediastinum. However, a normal chest
radiography, which lacks the absence or diminution of thymic
shadow, suggests cervical sequestration of thymic remnants. In
addition, several reports have demonstrated the coexistence of the
thymus and parathyroid glands in lateral cervical masses [8].
Conclusion
A cervical thymic remnant is a rare cause of neck masses;however,
it must be considered in the differential diagnosis in neck masses.
As they are common and rarely considered in the preoperative
differential of neck mass. It is important to identify these thymic rests
for what they are by their typical US appearance so that they will not
be confused with other neck masses arising from the thyroid, para
thyroid or lymphatic systems.
However, invasive surgical procedures may result in unhealthy
problems and rise for developing immune dysregulation. If surgery
is the choice in such patients, we recommend preoperative imaging
studies to assess the presence of mediastinal thymic tissue.
Acknowledgement
Thanks to Chancellor, Vice Chancellor, Pro-Vice-Chancellor,
Dean of the Medical College, D.Y. Patil Medical College; Kolhapur,
Eureka Diagnostic Centre; Kolhapur.
References
Citation
Vasudha N, Balkrishna K. Right Ectopic Cervical Thymus-A Rare Case Report. Indian J Appl Radiol. 2021;7(1): 165.