Case Series
Accessory and Cavitated Uterine Mass - Demystifying the Entity with a Case Series of Two Cases
Panchal V1, Arora R2* and Rathod Y3
1 Department of Radio diagnosis and Imaging, Government medical college and New Civil Hospital, India
2Department of Radio diagnosis and Imaging, Government medical college and New Civil Hospital, India
3Department of Radio diagnosis and Imaging Government medical college and New Civil Hospital, India
*Corresponding author: Arora R, Senior Resident, Department of Radio diagnosis and Imaging, Government medical
college and new civil hospital, Bunglow no. 2 , behind kapadia health club , janta nagar-B , New civil road , Surat, India;
Email: rajatarora180@gmail.com
Copyright: © 2021 Panchal V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 02/05/2021; Accepted: 05/06/2021; Published: 08/06/2021
Abstract
We present a case-series of 2 cases, of ACUM, which is a non-communicating functional cavity within a normal uterus, which resembles endometrial
cavity. It is considered to be a developmental anomaly, which characteristically presents at a younger age, with severe dysmennorhea. USG and MRI are
useful in diagnosis, which can be confirmed on laparohysteroscopy.
Keywords
ACUM (Accessory and cavitated uterine mass); Endometrial Cavity: MRI
Case 1
Clinical History: A 25 years old nulliparous female with chief
complaint of severe dysmenorrhea and chronic pelvic pain, which
aggravated during the days of menses. However no irregularity in her
menstrual cycles was seen. USG pelvis was advised.
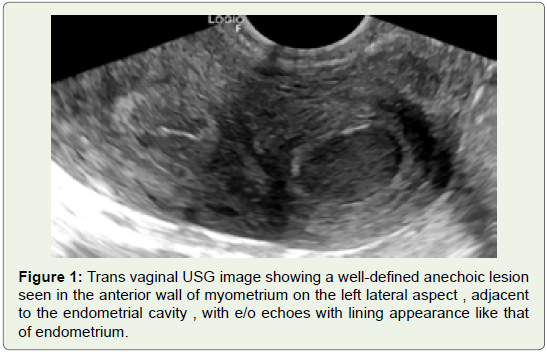
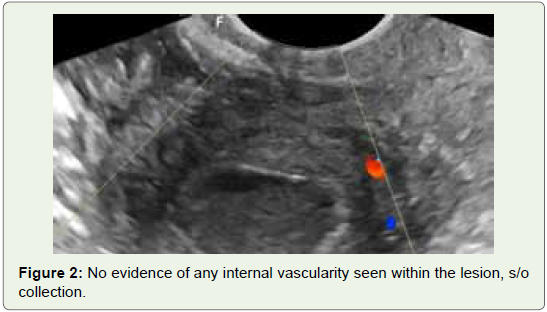
Imaging Findings: Her ultrasound pelvis revealed an anechoic
lesion in the myometrium just adjacent to the endometrial cavity
with e/o echoes and debris like internal material, without any internal
vascularity. This lesion simulated the characteristics of an endometrial
cavity.
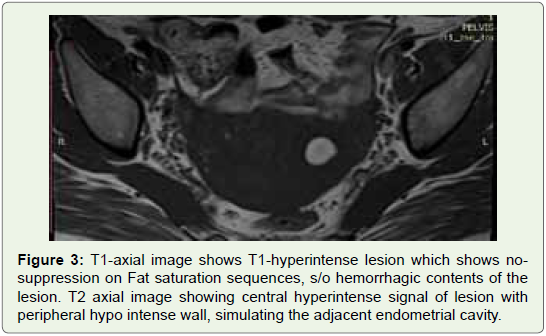
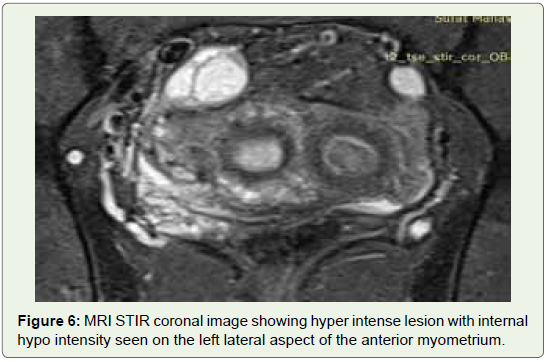
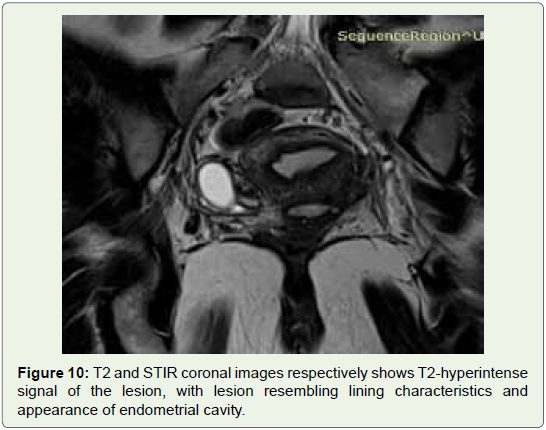
MR-pelvis showed approx 25 x 30 mm sized T2-STIR centrally
hyper intense and peripheral hypo intense and T1 hyper intense lesion,
which simulated the signal intensity characteristics of the endometrial
lining. T1-hyperintensity was representive of hemmorhagic contents
of this lesion; the lesion was intra-mural, involving the anterior wall
of myometrium on left lateral aspect;
CASE 2
Clinical History: A 21-year-old, nulliparous female patient
presented with a history of chronic pelvic pain worsening every
year, for more than 3 years. Her menstrual cycle was regular with
normal flow. There was no history suggestive of pelvic inflammatory
disease. She was treated with non-steroidal anti-inflammatory drugs
(NSAIDS) earlier and with oral contraceptive pills (OCP) for the
last few months. There was history of recurrent renal calculi. Per
abdomen examination was normal (Figure 1).
Imaging Findings:
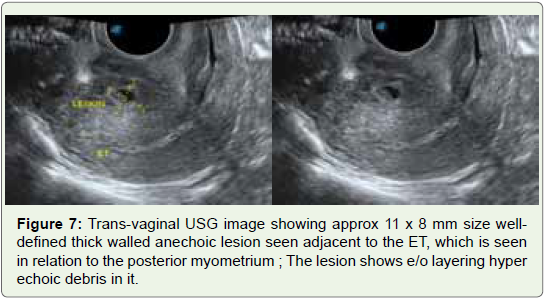
USG pelvis showed approx 11 x 8 mm size well-defined thick
walled anechoic lesion seen adjacent to the ET, which is seen in
relation to the posterior myometrium; the lesion shows e/o layering
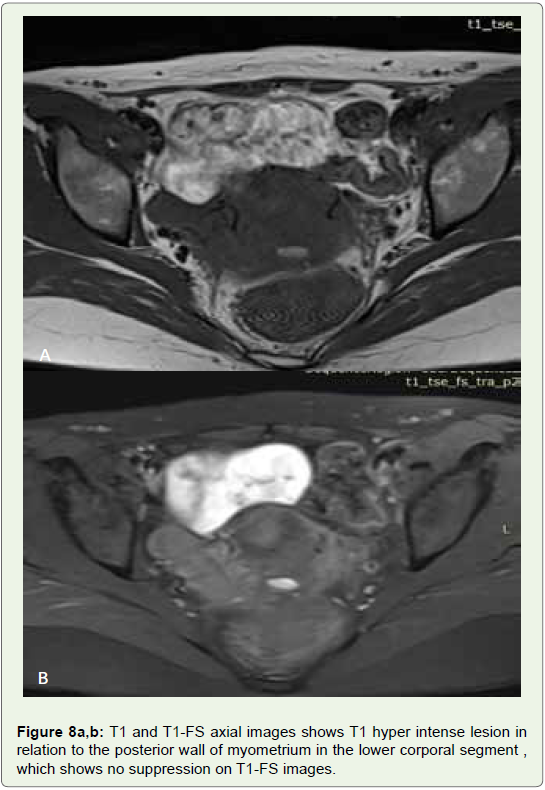
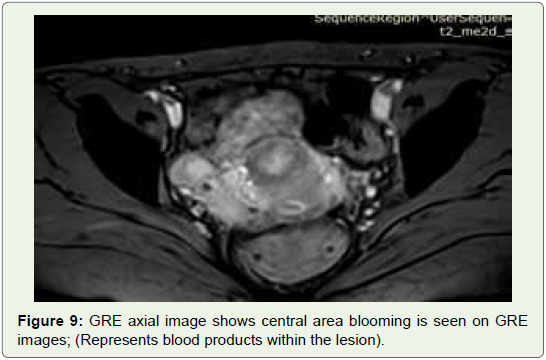
hyper echoic debris in it;MRI pelvis showed a T1-T2-hyperintense lesion in relation to the posterior wall of myometrium in the lower corporal segment ,
which shows no suppression on T1-FS images(Rules out fat signal
intensity); Intralesional central area blooming is seen on GRE
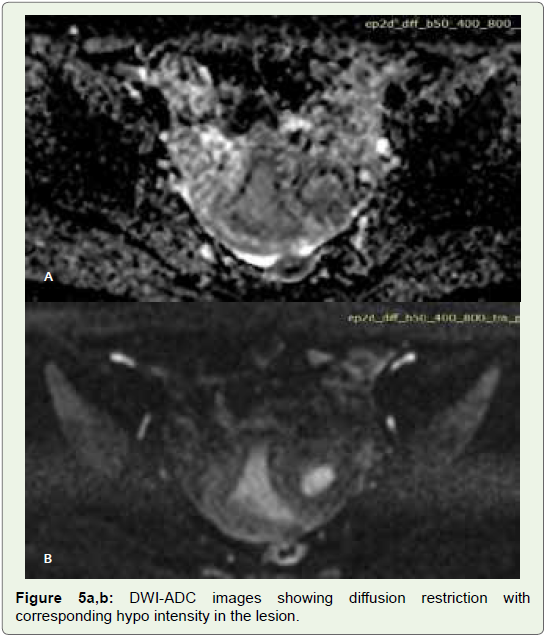
images; (Represents blood products within the lesion). The lesion
shows heterogeneous diffusion restriction with corresponding hypo
intensity seen on ADC images;
Based on the imaging findings in both the above-mentioned
cases, diagnosis of ACUM (Accessory and cavitated uterine mass)
was made; However second rare differential kept was that of a
necrotic fibroid.
Subsequent laparoscopic assessment confirmed the imaging
finding of ACUM (Figure 2,3).
Discussion
ACUM is a non-communicating ULM (Uterus like mass) arising
in the uterus itself [1]. The entity needs to be classified separately as the
uterine cavity is otherwise normal unlike other Mullerian anomalies.
It is considered to be a congenital anomaly [1] It characteristically
presents at a younger age, usually less than 30 years, with severe
dysmennorhea and chronic pelvic pain due to distention of the cavity
caused by repeated bleeding [2].
Out of the imaging modalities, USG is the initial investigation,
MRI is confirmatory and intra-operative laparoscopy is the gold standard
for diagnosis which has added benefit of being therapeutic;
USG is the initial imaging modality that can identify them as solid
iso echoic to predominantly cystic masses resembling endometrioma
arising within the uterus, visualized separately from the ovaries.
On HSG, the mass may not be visualized at all. However, the most
important role of HSG lies primarily in ruling out any Mullerian
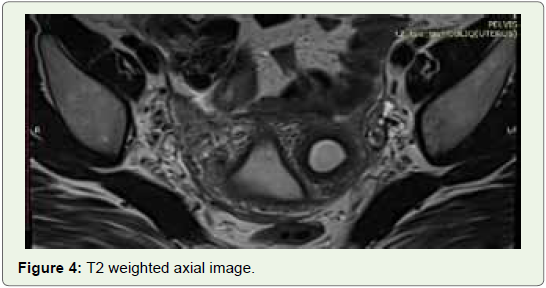
anomaly. MRI is the imaging modality of choice as it non‑invasive
and, hence, preferred over HSG in young unmarried females. It
clearly shows the pelvic anatomy; cavitated mass with hemorrhagic
contents; and the uterus, myometrium, and endo-myometrial
interface. Thin sections (3 mm) should be used as it will also help in
ruling out Mullerian anomalies (Figure 4)
The cavitated mass in ACUM is lined by endometrial glands and
stroma that are surrounded by irregularly arranged smooth muscle
cells. These can arise anywhere within and beyond the uterus at any
age , as was seen in our second case [2].
Laparoscopy remains the only option available for confirmation
and treatment. Regarding therapeutic management, most recent
publications have included laparoscopic excision of the mass (Figure 5,6).
Awareness and adequate knowledge of the entity can help the
radiologist make accurate pre‑operative diagnosis of ACUM, which
is very beneficial for the gynecologist to have maximum pre-operative
information;
Take-home message would be to keep in mind of this entity when
a young female patient with severe dysmenorrhea shows an accessory
Endometrium-like lesion in the myometrium; It is a treatable cause
and is not as rare as thought previously; An accurate pre-operative
diagnosis can be made;
Written informed patient consent for publication has been
obtained
Final Diagnosis: Accessory and cavitated uterine malformation
(ACUM)
Differentials: [3,4]
• Accessory and cavitated uterine malformation
• Cystic area of adenomyosis
• Necrotic intramural fibroid
• Focal adenomyoma
• Obstructed cavitated rudimentary horn with unicornuate
uterus.
The closest differential for ACUM is obstructed cavitated
rudimentary horn with unicornuate uterus. However in unicornuate
uterus, contra lateral tilt of the uterus, banana-shaped small uterine
cavity, favors obstructed horn [5].
Necrotic intramural fibroid will not mimic lining characteristics
of endometrial cavity and will not show T1 hyper intense signal
(Figure 7,8,9,10).
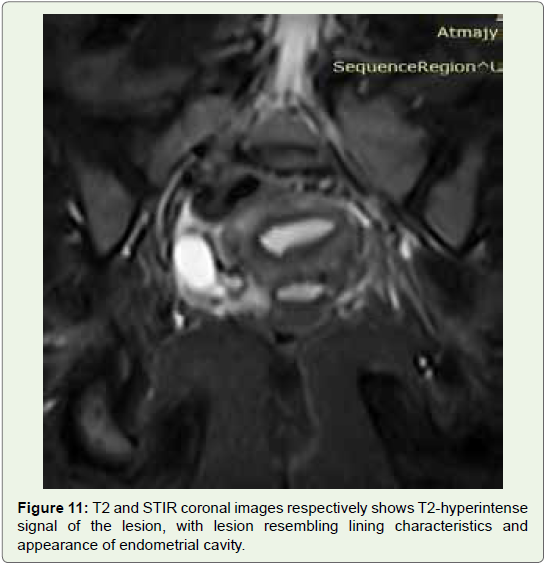
Likewise Cystic adenomyoma will not show T2-hyperintense
endometrial lining and hemorrhagic contents (Figure 11).
Conclusion
Accessory and cavitated uterine malformation (ACUM) is not as
rare as thought previously and an accurate pre-operative diagnosis
can be made , in a young female with clinical complaints of severe
dysmenorrhea, whose imaging findings shows an accessory cavity
which shows endometrium like characteristics. USG is the initial
investigation, with findings confirmed on MRI.
The MRI findings of an ACUM usually show an accessory cavity
with hemorrhagic contents in an otherwise normal-shaped uterus,
without any evidence of adenomyosis, and bilateral normal tubes and
ovaries should suggest the diagnosis of ACUM pre-operatively.
References
Citation
Panchal V, Arora R, Rathod Y. Accessory and Cavitated Uterine Mass - Demystifying the Entity with a Case Series of Two Cases. Indian J Appl Radiol. 2021;7(1): 163.