Pictorial Essay
Imaging Spectrum of Pulmonary Lymphoma
Sawalgi VC1, Patnaik S1*, Shirsha C1, Uppin S2 and Ramachandra Varma S2
1Department of Radiology, NIMS, Hyderabad, India
2Department of Pathology, NIMS, Hyderabad, India
*Corresponding author: Patnaik S, Department of Radiology, 404 Sai Kausalya apt, Gagan mahal Main Road, Hyderabad-500029; Tel: 9490793534; Email: sujata_patnaik222@yahoo.co.in
Copyright: © 2021 Sawalgi VC, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Lung involvement in lymphoma may be primary or secondary. Primary lung involvement is rare and more usually seen in Non-Hodgkin Lymphoma. The
main radiological findings of pulmonary lymphomas include- Pulmonary lesions appearing as a mass or mass like consolidation with or without cavitation
or bronchogram, masses of pleural origin- single or multiple nodules of sub-centimetre size, alveolar or interstitial infiltration and peribronchial, perivascular
thickening with or without atelectasis. The pulmonary lymphoma can be confused with carcinoma lung, metastases, pneumonia, organising pneumonia,
fungal infection and interstitial lung disease. Imaging manifestations of primary and secondary pulmonary lymphomas may be similar. Since the treatment
options of these two are different, it is necessary to differentiate primary pulmonary lymphoma (PPL) from the secondary disease (SPL). Certain characteristic
features like peripheral mass, cavitation, consolidations are more common in PPL. Mediastinal and hilar-adenopathy, central, peripheral lung lesions, nodules
are more observed in SPL.
Introduction
Pulmonary involvement is common especially in secondary and
recurrent disease than in primary lymphoma. The clinical and imaging
diagnosis is critical and is to be differentiated from other conditions.
Lymphomatous proliferation in chest can occur in three ways. It may
be haematogenous dissemination by either Hodgkin’s Lymphoma
(HL), Non-Hodgkin’s Lymphoma (NHL) or by direct extension from
hilar or mediastinal adenopathy. The first two situations occur by
either progression of disease or relapse of a pre-existing lymphoma.
Here treatment focuses on control of haematological spread. The
third pattern is primary pulmonary lymphoma which needs proper
differentiation from other diseases and starting the appropriate
treatment in time.
Lung involvement in lymphoma may be primary or secondary.
Imaging manifestations of these two may be similar. Primary lung
involvement is rare and more usually seen in NHL. When clonal
proliferation occurs in lung parenchyma or bronchi without any
detectable extra-pulmonary lymphoma at the time of diagnosis or in subsequent 3 months of diagnosis, it is called primary pulmonary
lymphoma (PPL)[1]. It may be associated with or without mediastinal
lymphadenopathy. PPL accounts for <1% of all lymphoma and 0.5-
1% of all lung primaries [2]. Most common type of PPL is MALT
(Mucosa associated lymphoid tissue lymphoma). Other frequent
form is Diffuse Large B Cell lymphoma (DLBCL). Primary NHL of
lung is rare subtype of extra-nodal lymphoma and is low grade Bcell
type accounting for <1%of all lymphoma [3]. Secondary pulmonary
lymphoma (SPL) is more common, and it may be HL or NHL.12%
of HL and 4% of NHL involve lung parenchyma on basis of chest
radiographic findings at initial presentation [4]. An autopsy series
demonstrated higher frequency of lung involvement up to 62% [5]. In
HL, the pulmonary involvement is common in recurrent disease and
determines stage 4. It is almost always associated with mediastinal
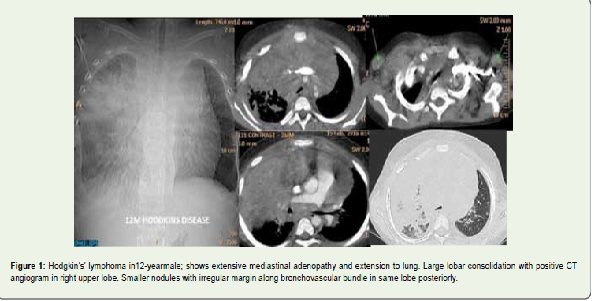
and hilar nodes (Figure 1). In immune-compromised patients
the lymphoma can be aggressive. Lymphoma is the second most
common malignancy after Kaposi’s sarcoma in HIV/AIDS patients.
It is thought to be due to consequence of long stimulation by HIV to
B lymphocyte proliferation. Prevalence of lymphoma is 40-100 times more common in AIDS patients as compared to general population. Transplant related lymphoma (TRL) is uncommon and is related to
Epstein virus and immune suppressant therapy. Most of them are B
Cell NHL.
A wide variety of radiologic findings are described in pulmonary
lymphoma. These findings are explained on basis of anatomy of
lymphatic system in lung. Either retrograde flow spread of tumour
directly from involved hilar or mediastinal node or ante grade spread
from multiple foci can occur. Haematogenous spread is rare [5]. The
main radiological findings include i) Pulmonary lesions appearing
as a mass or mass like consolidation with or without cavitation
or bronchogram, ii) Masses of pleural origin- Single or multiple
nodules of Subcentimeteric size or <3cms,iii) Alveolar or interstitial
infiltration, iv) Peri bronchial, perivascular thickening with or
without atelectasis. The pulmonary lymphoma can be confused with
carcinoma lung, metastases, pneumonia, organising pneumonia,
fungal infection and ILD. For local MALT lymphoma treatment is
surgery and for high grade pulmonary lymphoma the treatment is
chemotherapy. With recent advancements of treatment with bone
marrow transplantation the survival of these patientsis longer. Hence
early diagnosis is important, and CT is extremely useful diagnostic
modality for this clinical challenge. In this review we tried to focus on
important diagnostic clues for pulmonary lymphoma.
Consolidation
Consolidation is another common feature of pulmonary
lymphoma seen frequently in MALT and non-MALT form. Air
bronchogram sign is more frequent in MALTOMA than in non-
MALTOMA. Primary pulmonary MALTOMA is monoclonal B
cell proliferation in sub mucosal collection of B and T cells present
beneath areas of specialised bronchial epithelium throughout the
airway and especially at bronchial bifurcation. Tumour infiltrate
along sub mucosal epithelium and lumen appear smooth. These
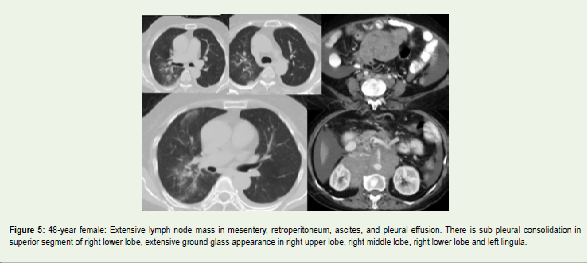
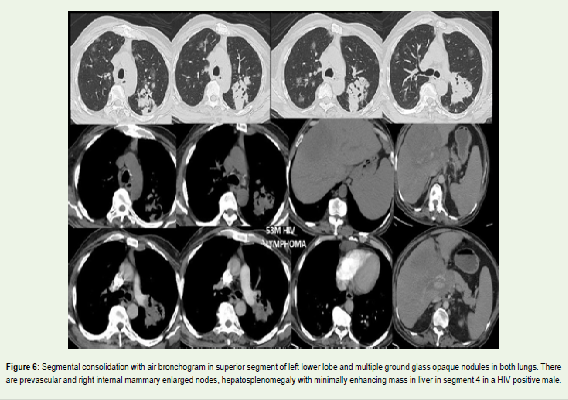
consolidations may be sub pleural (Figure 5) which appear polygonal
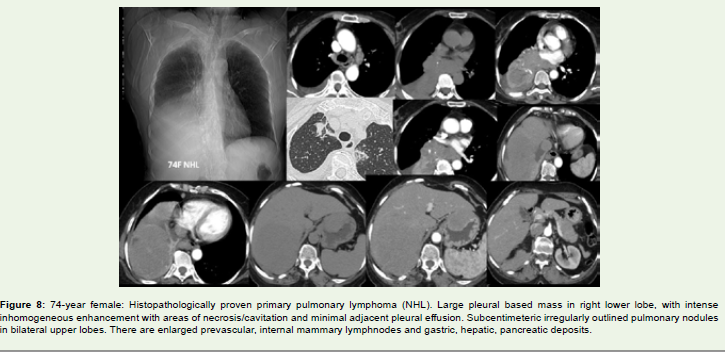
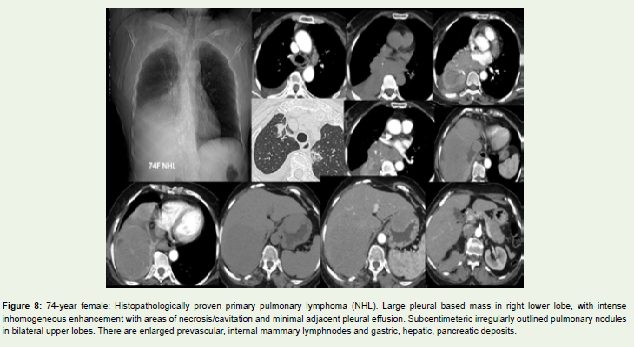
along pleura/fissure, lobular when a segment/lobe is involved (Figure 6), peribronchial when consolidation is distributed along the bronchovascular bundle with a tapered shape with tip towards hilum (Figure 7). Halo of ground-glass opacity (GGO) may be observed surrounding
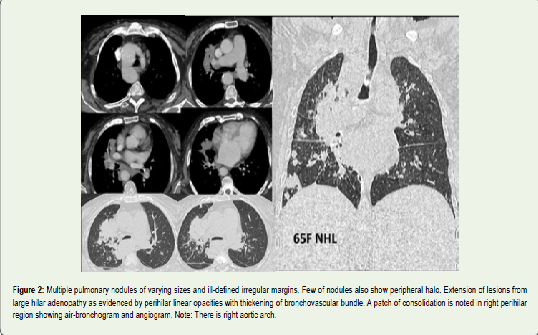
the consolidation. CT- angiogram sign is normal pulmonary vessels
within consolidation or mass after enhancement (Figures 1,2). This
is a specific sign in bronchiole-alveolar carcinoma and is more
commonly seen in MALTOMA. It is seen when lymphoma infiltrates
along Peribronchovascular interstitium without invading the vascular
wall. However high-grade malignant lymphoma can develop rapidly
and invade pulmonary vessels. An important differential at this stage
is lung cancer. Here the cancer cells infiltrate the vessel wall to cause
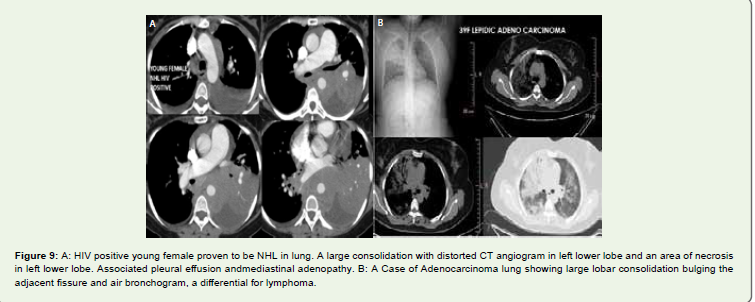
vascular distortion and destructions. Even in aggressive lymphoma
pulmonary vessels show distortion and destruction as in consolidation
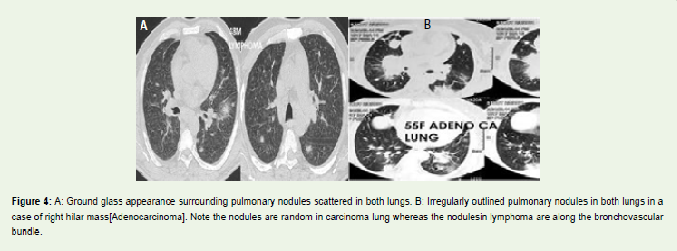
(Figure 8, 9A). Hence in non-MALTOMA, CT angiogram sign is less observed. Lesions cross lobes, fissures and infiltrate the adjacent lobes
on CT. Distribution from hilum to periphery across lobe fissure is
defined as butterfly sign. This sign is due to Lymphangitic spread
along pleura, Interlobular septa and bronchovascular bundle [7].
Similar phenomenon is seen in Carcinoma lung as well. Bulging
fissure due to massive consolidation is also observed in lymphoma.
Kliebsilla pneumonia is also a differential at this stage. Clinical
scenario differentiates the two. Lung cancer with distal collapse also
can present with bulging fissure (Figure 9A).
Mass
There may be mass or mass like consolidation in lungs. It may be
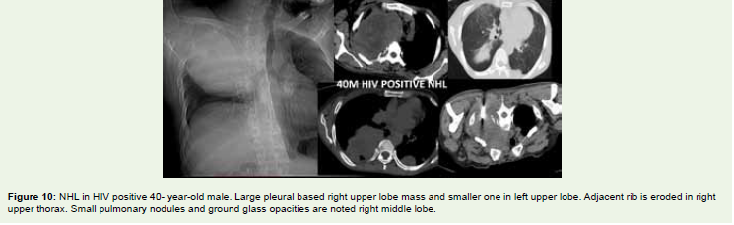
single or multiple. Size may vary from 0.5 to 8cms.Pleural based mass
predominantly seen in PPL (Figure 10). Pleural based masses seen
in 32% cases in HL and 31% in NHL [8]. Size is more than 3cms and
lesions may be associated with air bronchogram and CT angiogram
sign [9,11]. On contrast administration there may be intense
homogenous or heterogeneous enhancement. Jung et al studied 24
cases of PPL, 29.2 % patients had single or multiple nodules, 16.7%
had masses,41.7 % had infiltrates and 20.8% showed consolidation.
Hilar adenopathy was found in 5 of 24 cases and one had chest wall
invasion [9]. Mass invades the chest wall and erodes the bone as seen
in (Figure 10).Cavitation may be observed in the mass (Figure 11) and
usually seen in DLBCL. HL is usually associated with mediastinal
adenopathy. DLBCL are associated with mediastinal adenopathy and
pleural effusion than the low-grade form of PPL.
Interstitial Disease Pattern
Diffuse ground glass opacities are often seen imaging finding
in lymphoma. They may be seen as patchy areas of GGO randomly
distributed in both lungs(Figure 5,10). CT findings of MALT
lymphoma have varied pattern. Interstitial disease pattern presenting
as GGO is not uncommon with an incidence of 6 to 10% in pulmonary
MALT lymphoma [10]. On histology masses, consolidation, nodules
represent alveolar infiltration and GGO is lymphomatous infiltration
of interlobular septae and alveolar wall [10].The spread is via vascular
rather lymphatic pathway. Pathologically tumour cells in DLBCL,
form sheets that distort or destroy lung architecture. Differentials
are infection, diffuse alveolar hemorrhage and interstitial diseases. A
few reports described diffuse GGO in DLBCL without lung nodules,
masses, or consolidations [11]. Intravascular large B-cell lymphoma
(IVLBCL) is characterised by tumour cells located almost entirely in the intravascular, peripheral blood and bone marrow which makes it difficult to differentiate from other tumours. It is classified as special
type of lymphoma. In 2008, WHO identified it as a rare type of NHL.
There is diffuse occlusive proliferation especially in capillaries, small
arteries, and veins [12]. CNS, skin, lung, and kidney are usually
involved, and liver, spleen and lymph nodes are rarely involved.
Lung involvement can present as GGO, centrilobular nodules,
interlobular septal thickening, interstitial shadow and thickening of
bronchovascular bundle suggesting lymphatic and or haematological
spread. The differentials of GGO are infections, alveolar hemorrhage,
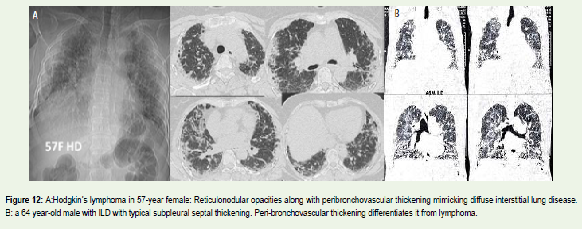
and interstitial lung disease (Figure 12A,B). The differentiation is
made on clinical grounds and other associated imaging features. Less
than 10% of patients have bilateral diffuse reticulo-nodular opacities,
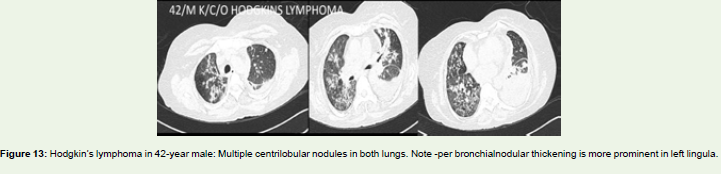
atelectasis, or pleural effusion (Figure 13). Miliary densities <3mm nodules
in linear fashion distributed diffusely throughout the lungs along the
bronchi may be observed. A well described imaging findings of lung
involvement in lymphoma are lymphangitic spread characterised
by nodular thickening along pleura, interlobular septal thickening
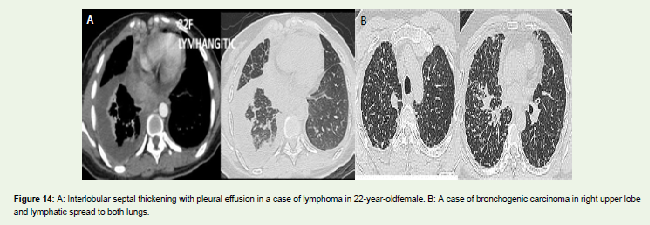
and thickening along bronchovascular bundle(Figure 13,14A). SPL
is known to present as thickening of bronchovascular bundle and
interlobular septal thickening in 41% of cases (Figure 14). This represents
the retrograde spread of lymphoma from involved hilar/mediastinal
lymphadenopathy. Sarcoidosis and lymphangitis carcinomatosis are
differentials (Figure 14B).
HIV Lymphoma and Transplant Related Lymphoma:
25-40%HIV patients develop malignancy and 10% will develop
NHL [3] (Figure 9,10). The NHL is aggressive diffuse large B cell
lymphoma (DLBCL). Imaging findings are primarily mass and
lymphadenopathy (15). Usually, the nodes show central necrosis,
and the mass is large and may have bone destruction (Figure 10). Lung involvement is usually secondary. Transplant related lymphoma (TRL) is uncommon and is related to Epstein virus and
immunosuppressant therapy. Most of them are B Cell NHL. It is
relatively uncommon, but when occurs, it is fatal. Imaging findings
of TRL are similar to that of lymphoma without transplantation.
Lymphadenopathy, pulmonary nodules, and mass may be observed.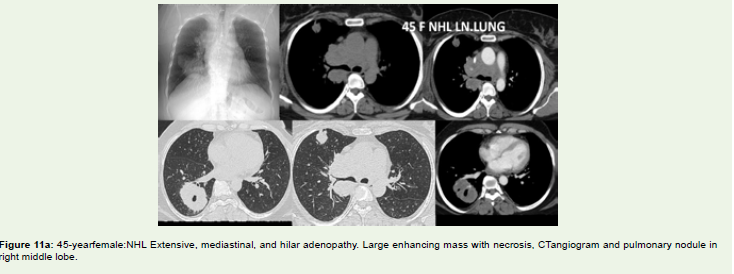
Conclusion
Pulmonary manifestations of lymphoma are varied. Distribution
of lesions is typical. When there are multiple findings with typical
distribution one has to think of pulmonary lymphoma. Since the
treatment option of PPL and SPL are different, it is necessary to
differentiate PPL from SPL. Certain characteristic features like
peripheral mass, cavitation, consolidations are more common in PPL.
Mediastinal and hilar adenopathy, central, peripheral lung lesions,
nodules are more observed in SPL.
References
Citation
Sawalgi VC, Patnaik S, Shirsha C, Uppin S, Ramachandra Varma S. Imaging Spectrum of Pulmonary Lymphoma. Indian J Appl Radiol. 05 2021;7(1): 161.