Pictorial Essay
Perforation of Hollow Viscus and MDCT
Patnaik S1*, Howdekar M1, Ramachandra Varma S2 and Jyostnarani Y1
1Department of Radiology, NIMS, Hyderabad, India
2Department of GI Surgery, NIMS, Hyderabad, India
*Corresponding author: Patnaik S, Department of Radiology, 404 Sai Kausalya apt, Gagan mahal Main Road, Hyderabad-500029; Tel: 9490793534; Email-sujata_patnaik222@yahoo.co.in
Copyright: © 2021 Patnaik S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 02/12/2020; Accepted: 17/03/2021; Published: 22/03/2021
Abstract
Perforation of hollow viscus or GIT is common in clinical practice. Plain radiograph, ultrasound and fluoroscopy have limited value in its evaluation.
MDCT is the gold standard for localisation of the site of perforation. Pattern of air collection depends on the site of perforation. In oesophageal perforation
air outlines mediastinum, lesser curvature, or liver. Peptic ulcer perforation commonly occurs in gastric antrum. Collection of free air occurs at midline, along
falciform ligament and ligament teres. In small bowel perforations, escaped air is too small to be appreciated even on MDCT making diagnosis difficult. Air
may be noted in mesenteric folds, anterior surface of liver in mid abdomen. Ascending, transverse and, descending colonic perforations can present with
air in right anterior pararenal space, lesser sac and left anterior pararenal space, respectively. Location of free air/ fluid, bowel wall thickening, discontinuity
and adjacent stranding can help in predicting the site of perforation on MDCT.
Introduction
Perforation of hollow viscus or GIT is common in clinical
practice presenting as acute abdomen. Accurate and early diagnosis
is important as the mortality is high despite advanced treatment
protocols. Sometimes diagnosis may be difficult if there is no or
very minimal extraluminal air. In such situations critical analysis of
images is important to reach a diagnosis. Wide variety of entities such
as inflammatory bowel disease like Crohn’s disease, Ulcerative colitis,
neoplastic diseases, trauma, post- intervention like endoscopy/
colonoscopy, post-operative and FB ingestionare various causes of
perforation. Thispictorial essay and literature review will highlight
the key imaging features for diagnosis and to localise the site of
perforation.
Investigations:
Plain radiograph remains the basic investigation for
demonstrating the free air and FB if radio-opaque (Figure 1). An
erect chest radiograph is the most sensitive tool for detection of free
intra-peritoneal gas. However, localisation of site of perforation is
difficult. MDCT is the gold standard for diagnosis and localisation
of the site of perforation with accuracy from 82-90% [1]. Certain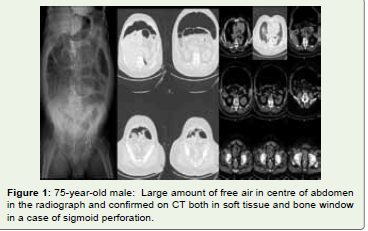
technical modifications are to be done in evaluation of these cases.
Unless there is any contraindication, both oral and IV contrast are
to be performed. Water soluble contrasts do not cause inflammatory
reaction if extravasated. They get rapidly absorbed. Entire abdomen
and pelvic scans are mandatory and for oesophagus or pharynx
entire chest to be scanned. Assessment in both bone window and
lung window in addition to normal are needed (Figure 1) for better
demonstration of air, FB. Multiplanar reconstructions are essential to
localise extraluminal air/area of discontinuity with high accuracy [as
high as 82 to 90%] in detecting extraluminal gas and to localise the
site of perforation [1]. It is also necessary to differentiate contained
perforation from free perforation as the later has to be managed by
immediate surgery.
Ultrasonography (USG) is not the primary modality of choice.
However, it can detect air in peritoneal cavity. The presence of free
fluid can also be detected. Fluoroscopy can detect water-soluble
contrast leak from perforated site and can confirm the diagnosis
when there are equivocal findings on CT.
Imaging features of hollow viscus perforation:
There are many direct and indirect signs of perforation. Free
extraluminal air has been regarded as major finding of perforation
[2]. CT is sensitive to detect free extraluminal air (localise whether
it is intra or extra peritoneal location) [Figure 2A,Figure 2B,Figure 3 ). Air collection depends on site of perforation. Direct visualisation of
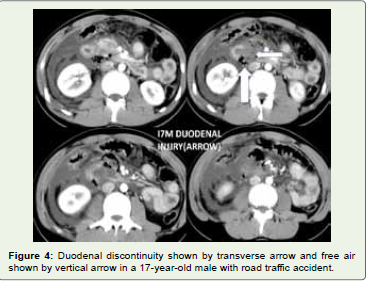
discontinuity of bowel wall is another direct sign and it indicates
exact site of perforation. Discontinuity is a hypodense cleft running
perpendicular to bowel wall on CT [3] (Figure 4). However, the cleft
is demonstrated on CT in less than 50% of cases [2]. Multiplanar
reconstruction is essential as axial images may not be demonstrated.
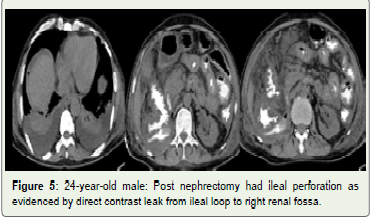
Other signs to localise site may include air collection at the site of
injury (Figure 5), extravasation of contrast (Figure 5), wall thickening,
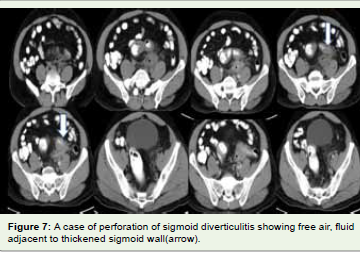
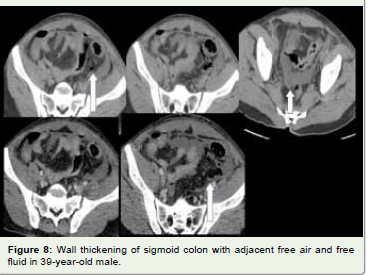
fat standings in adjacent mesentery, fluid collection (Figure 6-8) and
localised phlegmon and abscess are other features. CT has an accuracy
of 82-90% in detection of exact site of perforation [1]. There are
certain imaging features specific to site and etiology of perforations.
Pneumoperitoneum is common after abdominal surgery. It resolves
in 3-6 days after surgery and may persist as long as 24 days. Persistent
or increasing free air and or as cites postoperatively indicate iatrogenic
perforation.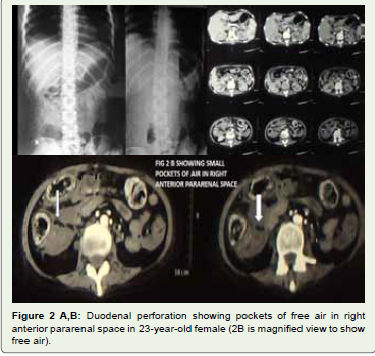
Site specific imaging features:
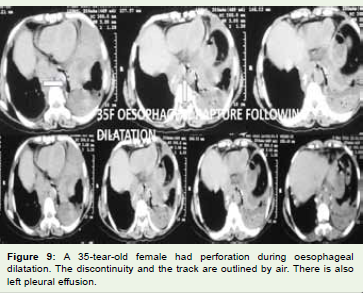
Oesophageal rupture is catastrophic as it leads to mediastinitis and
sepsis very quickly. Mortality is as high as 13.3% and after 24 hours
it still increases [4]. Common cause of oesophageal perforation is
iatrogenic like stenting, dilatation of strictures and sometimes during
endoscopy, post-operative. Other includes trauma, FB ingestion,
corrosive poisoning, and neoplastic conditions. Spontaneous rupture
known as Boerhaave syndrome may be a clinical emergency. Lack
of serosal layer makes the oesophagus and poor arterial supply
causes more susceptible to injury as compared to rest of the GIT. In
oesophageal perforation air seen outlining mediastinum, along lesser
curvature or it may outline the liver and stomach. Extravasation of
oral contrast, pleural, pericardial effusion, and fluid in mediastinum
(Figure 9) are other features. Pleural effusion usually occurs on left
side. Subcutaneous emphysema of chest wall and neck are common.
Thickening of oesophageal wall is also observed like in other parts of
GIT.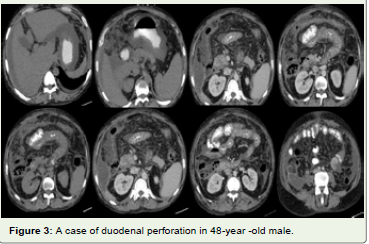
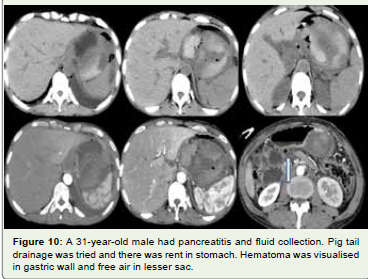
Among various causes peptic ulcer disease is major cause of gastric
perforation followed by necrotic/ulcerated malignancies, iatrogenic
injury (Figure 10) and trauma. Peptic ulcer perforation commonly
occurs in gastric antrum. Collection of free air occurs at midline
Along Falciform ligament (called Falciform ligament sign,) and along
ligament Teres (ligament Teres sign). It may also be observed in lesser
sac. There may be large amount of air and sometimes it collects along
mesenteric leaves. Air in supra-mesocolic compartments indicates
gastro-duodenal perforation, gas in lesser sac indicates posterior
gastric wall perforation, gas along falciform ligament, hepatic fissure,
and ligament Teres indicates intra-peritoneal rupture of gastroduodenal
segment. Hence location or air is important in deciding site
of perforation. Traumatic gastric injury is suspected when there is air
in splenic location and left lobe of liver injury is suspected if the air is
located in diaphragmatic areas in cases of RTA. MDCT can recognise
the injury tract.
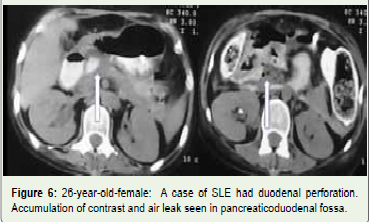
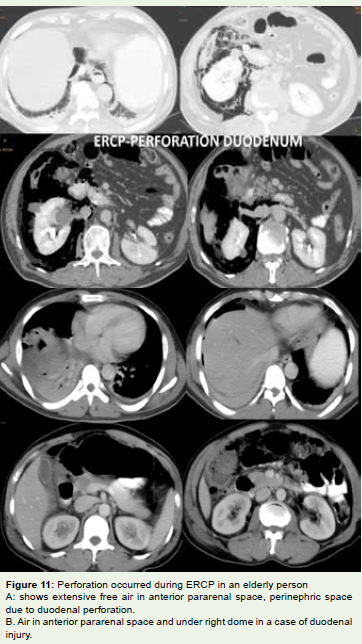
Duodenal perforation mostly due to peptic ulcer disease,
complication of endoscopic procedure (Figure 11A) or due to trauma
(Figure 11B), malignant, inflammatory, and ischaemic causes.
Duodenal perforation may be pre-bulbar or post- bulbar. CT features
of duodenal perforation are extraluminal air or pneumo-peritoneum.
Air collection depends on site of perforation. If it is bulbar free air
collects in midline, along Falciform ligament or ligament Teres. Post
bulbar perforation causes air to collect in left anterior pararenal space.
Traumatic injury /perforation occurs in vertical and horizontal part
of duodenum as this is the site of firm attachment in retroperitoneum.
Acute angles of first and second part of duodenum, acute angle of
third and fourth part of duodenum, and compression against vertebra
predispose for occurrence of perforation (Figure 4,Figure 6 and Figure 11B).
Air collects in retroperitoneum (anterior pararenal space). Diagnosis
is delayed as it is retroperitoneal structure and signs are difficult
to be elicited. Peritonitis develop once the duodenal contents are
extravasated into peritoneal cavity. The early diagnosis is crucial for
prompt management.
Perforation from traumatic injuries occurs predominantly in
the descending and horizontal segments of theduodenum, mostly
by blunt trauma in children and by penetrating trauma in adults,
and cause pneumo-retro-peritoneum in the anterior pararenal
space[8]. CT is helpful in distinguishing a duodenal hematoma
from Gastroduodenal Perforation from traumatic injuries occurs
predominantly in the descending and horizontal segments of the
duodenum, mostly by blunt trauma in children and by penetrating
trauma in adults, and cause pneumo-retro-peritoneum in the anterior
pararenal space [8]. CT is helpful in distinguishing a duodenal
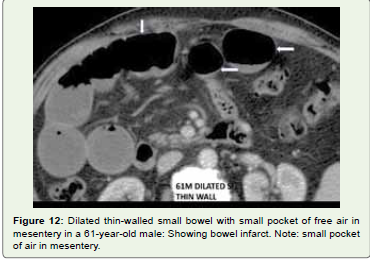
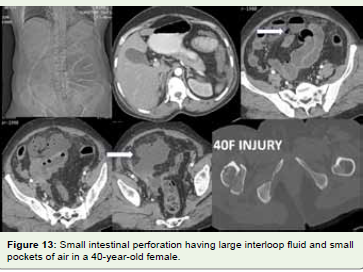
hematoma from perforation. Small bowel perforation is usually
caused by peptic ulcer disease, trauma, FB, iatrogenic, inflammatory
conditions, infarcts, or neoplasia. Usually, the escaped air is too small
to be appreciated even on MDCT. Air may be noted in mesenteric
folds, anterior surface of liver in mid abdomen (Figure 1). Blunt
injury of SI may be indicated by small air bubble in mesentery,
extravasation of oral contrast (Figure 5), bowel wall thickening,
mural discontinuity, moderate to large volume of peritoneal fluid and
mesenteric infiltration. In penetrating trauma leakage of oral contrast
is more specific than only demonstration of free air. Since many times,
the free air is too subtle to be recognised attention must be paid to
localised interloop collection of extraluminal fluid between fluid filled
loops [1]. Hence CT diagnosis of small intestinal injury is challenging
as there are no specific signs. Combination of bowel wall thickening,
bowel wall discontinuity are accurate indicators, Mesenteric fat
stranding and moderate to large volume of intraperitoneal fluid
in absence of solid organ injury suggest small intestinal injury [1]
(Figure 13). FB perforation common to occur at less fixed segments
and with acute angulations like ileum, IC junctionor rectosigmoid
regions. CT signs may be free air, bowel wall thickening, adjacent
fat infiltration and identification of FB [6,7]. Anastomotic leak is
identified by contrast extravasation. Strangulated bowel indicates
infarction. The diagnostic findings are intestinal wall thickening,
mural hypoperfusion, pneumatosis intestinalis, gas in portal vein
and pneumoperitoneum. Inflammatory bowel disease and neoplastic
condition can be diagnosed on CT. Transmural Crohn’s disease may
lead to contained perforation due to presence of adhesions between
the loops. Subsequent phlegmon and abscess formation with localised
peritonitis may develop.
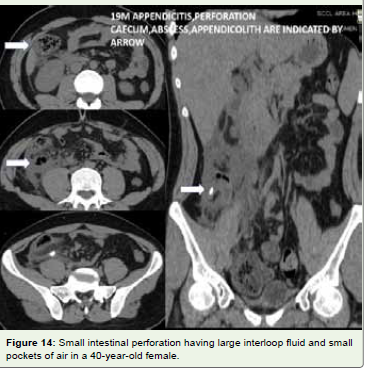
Perforation can be a complication of appendicitis. Usually, small
amount of air not more than 1 to 2ml may be seen [8]. Extraluminal
air, extraluminal appendicolith, abscess, phlegmon and defect in the
wall are diagnostic features of appendiceal perforation (Figure 14).
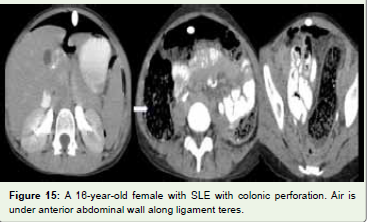
In colonic perforation air is detected in mesenteric folds,
retroperitoneum (Figure 14). In ascending colonic perforation air
is seen in right anterior pararenal space, Perforation of descending
colon shows air in left anterior pararenal space, sigmoid colon in left
anterior pararenal space, rectal in anterior and posterior pararenal
spaces and transverse colon in lesser sac. Air leak may be large in
colonic perforation (Figure 1 and Figure 15). Malignant lesion, diverticulitis
(Figure 7 and Figure 8), trauma and ischemia are common causes of
perforation on left side colon. Inflammatory bowel disease (Figure 15), diverticulitis, penetrating trauma are the aetiologies on right side
colon. Caecum is perforated in bowel obstruction. Iatrogenic injury is
common in rectum and sigmoid colon.
Conclusion
Familiarity with specific features like free air, free fluid, bowel
wall thickening, discontinuity and adjacent mesenteric stranding can
help us in predicting the site of perforation on MDCT.
References
Citation
Patnaik S, Howdekar M, Ramachandra Varma S, Jyostnarani Y. Perforation of Hollow Viscus and MDCT. Indian J Appl Radiol. 05 2021;7(1): 159.