Research Article
MRI Features of Different Molecular subtypes of Breast Cancer
Issar P1*, Sinha S2, Ravindranath M3 and Issar SK4
1Department of Radiodiagnosis, JLN Hospital and Research Centre, India
2Department of Radiodiagnosis, KIMS Superspeciality Hospital, India
3Depetment of Pathology, JLN Hospital and Research Centre, India
4Director In-charge, JLN Hospital and Research Centre, India
*Corresponding author: Issar P, HOD Radiodiagnosis, JLN Hospital and Research Centre Bhilai Chhattisgarh, DB-8, Talpuri, Bhilai, Chhattisgarh, 490009, Tel: 9407983540; Email: mareesh_23@yahoo.co.in
Copyright: © 2020 Issar P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 25/06/2020; Accepted: 04/09/2020; Published: 10/09/2020
Abstract
Background: Molecular subtypes of breast cancer have different imaging findings on MRI.
Aim: To assess the MRI features of different molecular subtypes of breast cancer.
Setting and Design: A retrospective observational study.
Materials and Methods: 82 patients with histopathologically confirmed breast cancer along with immunohistochemistry were included in this study. MRI
was performed with a 1.5 T Scanner (Signa excite GE healthcare) using a dedicated 8 channel breast coil. MRI findings were correlated with the different
molecular subtypes of breast cancer. Statistical Analysis was performed with statistical software SPSS 17.0, p-Value < 0.05 were considered significant.
Results: The molecular subtypes distribution was Luminal A in 48.78%, Luminal B in 9.76%, Human Epidermal Receptor 2 positive (HER2+) in 14.64%
and Triple Negative Breast Cancer (TNBC) in 26.82% of the patients. Luminal A subtype presented mainly as a mass lesion with an irregular shape, spiculated
margin, and heterogeneous enhancement. TNBC was mainly showing high intratumoral signal intensity (p=0.0003),unifocal lesion (p=0.0002), round or oval
(p=0.006), smooth margin, rim enhancement and having high ADC value (p=0.017). Multifocal or non-mass lesion along with axillary adenopathy, skin,
peritumoral, and prepectoral edema was found to be more common in Luminal B and HER2+ subtypes.
Conclusion: Breast MR Imaging can help in assessing different molecular subtypes of breast cancer, especially in Luminal A, as an irregular mass with spiculated margin and round or oval mass with rim enhancement and high ADC value in TNBC. Multifocal masses with adenopathy and skin involvement in Luminal B and HER2+ molecular subtypes.
Keywords
Breast MRI; HER 2 positive; Luminal A; Luminal B; Triple negative Breast cancer
Introduction
Breast cancer is a heterogeneous disease with many histological
and molecular subtypes that have a different response to therapy
and prognosis. Traditional criteria for treatment choices were the
size of the tumor, histological grade, lymph node involvement, local
invasion, and distant metastasis. However, patients with the same
stage of cancer and similar histopathological characteristics may
show different clinical behavior and prognosis. Advances in gene
expression analysis with DNA microarray technology have provided
new molecular subtypes. Luminal A, Luminal B, Human epidermal
growth factor receptor 2 (HER2) enriched & triple-negative (basallike).
Immunohistochemical (IHC) staining is a reliable surrogate
for these subtypes [1,2]. Luminal A subtype is associated with a low
proliferation index (Ki-67), accounts for 50-60% of all breast cancers, and has the best prognosis. Luminal B subtype is associated with a
high expression of the Ki-67 proliferation index, accounting for
20 % of all breast cancer, and has a poor prognosis as compared to
Luminal A. Luminal B characteristically do not over express HER2/
neu, but approximately 30% of them will be HER2 enriched.HER2+
subtypes account for 10% of all breast cancers and are characterized
by the absence of hormone receptors and high expression of the
HER2/neu gene. Triple-negative subtype accounts for 7-16% of all
breast cancers and is characterized by the absence of expression of
hormone receptors and HER2+, associated with a high expression of
cytokeratin genes of high molecular weight. This subtype is associated
with less differentiated invasive carcinoma and accounts for 70% of
breast cancers on BRCA 1 mutated females. HER2+ and Triplenegative
subtypes show a good response to chemotherapy but have
the worst overall survival [3-5].
Dynamic contrast-enhanced magnetic resonance imaging (DCEMRI)
is an efficient imaging technique in evaluating breast cancer
patients for preoperative surgical planning and treatment choices.
The correlation of imaging findings with molecular subtypes of breast
cancer is an emerging area of recent studies. The purpose of this
study was to assess the MRI features of different molecular subtypes
of breast cancer.
Materials and Methods
This retrospective MRI study included 82 women with
pathologically confirmed breast cancer and different molecular
subtypes by immunohistochemistry from March 2018 to February
2020. Molecular subtype findings based on immunohistochemistry
were correlated with MR findings.
Patients having ductal carcinoma in situ & those who had received
neoadjuvant therapy were excluded from the study.
Methods:
MR images were obtained with the patient in prone position in
a 1.5 T scanner (Signa Excite GE Healthcare, Milwaukee) using a
dedicated 8 channel breast coil. Each study includes pre-contrast as
well as post-contrast sequence. All MRI sequences and parameters
are listed in Table 1. Diffusion-weighted imaging (DWI) at b values0
and 1000 was performed and Apparent Diffusion Coefficient (ADC)
was calculated. Single unenhanced and six serial dynamic contrastenhanced
axial image set was obtained using VIBRANT acquisition technique before and immediately after rapid I.V bolus infusion of
0.1 mmol/Kg body weight of gadodiamide (Omniscan) at a rate of
2 ml/sec with a power injector. Immediately following the contrast
injection, 20c.c. saline was injected to flush all contrast media.
Dynamic contrast-enhanced image acquisition was started just after
the injection. The acquisition time of each phase was 80 seconds. The
total duration of the MRI was 25 minutes. Subtraction and maximum
intensity projection (MIP) sequences were generated.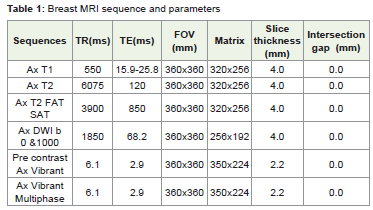
Image analysis:
MR images were retrospectively interpreted by two radiologists
(PI, SS) having 11 and 5 years experienced in breast MRI. Any
disagreement was solved by consensus. The morphological and
enhancement kinetic features were analyzed based on the 5th Edition
of the American College of Radiology (ACR) breast imaging reporting
and data system(BI-RADS) MR lexicon [6]. The morphology included
mass and non-mass type lesions. When a breast had more than one
lesion and those lesions were not connected, it was categorized as
having multiple lesions. The non-mass enhancement was further
described as linear, ductal, segmental, and regional. The evaluation
of the enhancement kinetic curve was based on the initial phase
(within the first 2 minutes) and the late phase (after 2 minutes). The
initial enhancement phase is further categorized into fast, medium,
and slow. The late enhancement phase was described as persistent,
plateau, and washout. On this basis, the tumor was graded with 1,2,
and 3 enhancement kinetics. For the measurement of tumor size, the
longest dimension of the tumor appearing on the post-contrast scan
was recorded. When there were multiple lesions in one breast, only the
biggest lesion was measured. Additionally, in mass lesions, whether
they were showing rim enhancement pattern, were evaluated. The
vessel enhancement could be easily identified and excluded based on
MIP. Axillary lymph nodes were evaluated on pre-contrast non FAT
SAT axial, T1 Weighted Imaging (WI). An enlarged lymph node was
defined as a node, abnormal in shape (round or oval) with irregular
margin, increased cortical thickness (greater than 3mm), completely
or partially effaced fatty hilum [7]. It was considered as suspicious of
Malignancy and confirmed on pathological examination of specimen
received with axillary node dissection.MRI features of different molecular subtypes were compared for
tumor size, shape, and margin, intratumoral signal intensity on T2WI,
Dynamic Contrast Enhancement (DCE) pattern, signal intensity
curve, and multifocal or multicentric disease. We analyzed all lesions
for associated MR Imaging findings such as skin or nipple invasion,
chest wall, or pectoralis muscle invasion. These were described as
abnormal enhancement of these locations. Edema if present, was subclassified
as skin edema, perilesional edema, and prepectoral edema.
Statistical analysis was performed by using statistical software SPSS
17.0, p<0.05 was considered significant.
Histopathologic Assessment:
Histopathologic analysis from the surgical specimen, revealing
histological type, pathological grade, and lymph node status was
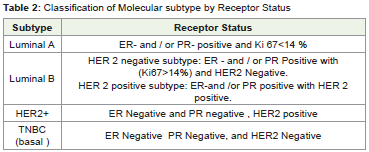
obtained. The molecular subtype of breast cancer was classified
depending on the status of ER, PR, HER 2, and Ki67 index (Table 2).
HER 2 status was scored as 1+, 2+, or 3+ using IHC analysis, as well as fluorescence in situ hybridization (FISH). If the score performed 2+
for IHC, a positive HER 2 result was IHC staining of 3+ or 2+ with a
FISH result confirmed gene amplification.Statistical Analysis:
Statistical Analysis was performed with statistical software
SPSS 17.0, p-Value < 0.05 were considered significant. The study
was approved by the institutional ethical committee and informed
consent was waived due to the retrospective design of the study.Results
The study includes 82 breast cancer women with ages ranged from
32 to 80 years. Breast cancer was classified into molecular subtype
as Luminal A (40/82,48.78%), Luminal B (8/82,9.76%), HER2+
(12/82,14.64%), TNBC (22/82,26.82%) with mean age 55.88 ±14.01
for Luminal A (LA), 64.7 ±13.26 for Luminal B (LB), 59.17 ±9.86 for
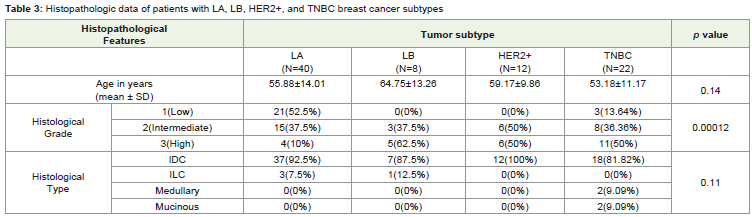
HER2+ and 53.18 ±11.17 for TNBC. Histologically grade I cancer was
found in 29.27% cases, grade II in 39.02%, and grade III in 31.71%
cases. Regarding the results comparing the pathological variable
among the four tumor subtypes (Table 3), tumor histological grade
was significantly different among them. The percentage of histological
grade 3 in LA (10%) was quite low as compare to LB (62.5%), HER2+
(50%), and TNBC (50%). All breast cancers histological types were
as follows: invasive ductal carcinoma (IDC,n=74), invasive lobular
carcinoma (ILC,n = 4), mucinous carcinoma (n= 2), medullary
carcinoma (n=2).
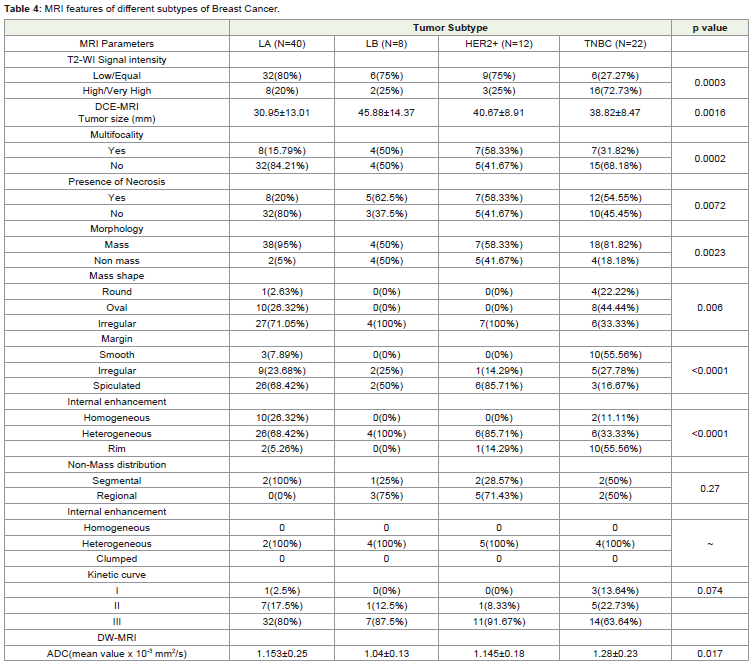
Regarding MRI features (Table 4), all tumors were detected as
an area of abnormal enhancement. The majority of the lesions in
LA and TNBC subtype showed mass-like enhancement 38/40(95%)
in LA,18/22(81.82%), in TNBC, as compared to 4/8(50%)for LB and
7/12(58.33%) for HER2+ with p=0.0023. On DCE MRI larger tumor
size was found in LB subtype, 45.88±14.3mm in LB Vs. 40.67±8.91mm in HER2+, 38.82±8.47mm in TNBC, and 30.95±13.01mm in LA
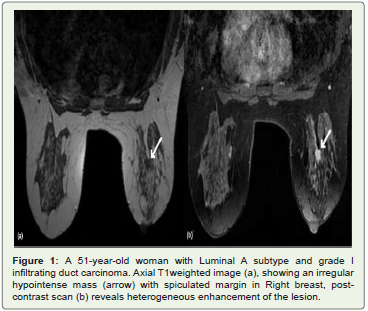
respectively with p=0.0016. Most of the LA (84.21%), (Figure 1)
and TNBC (68.18%) tumors were unifocal as compare to HER2+
(41.67%) and LB (50%) with p=0.0002. Intratumoral necrosis was
more common in LB (62.5%), HER2+ (58.33%) and TNBC (54.55%)
as compare to LA (20%) with p=0.0072. Most of the TNBC with
mass-like enhancement had oval shape (44.44%),p=0.006 while
100% of LB, 100% of HER2+, and 71.05% of LA had irregular
shapes. The margins of the TNBCs subtype were smooth (55.56%),
p<0.0001 as compared to LA (68.42%) which were mainly spiculated.
The predominant internal enhancement of the TNBC was rim
enhancement, identified in (55.56%), p<0.0001, while heterogeneous
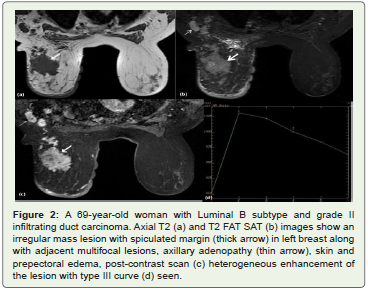
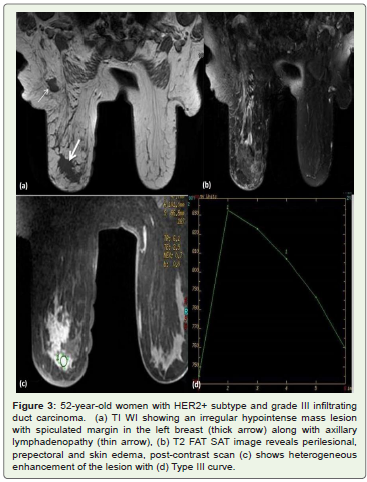
internal enhancement was predominant in LB (Figure 2), HER2+
(Figure 3) and LA subtypes, 100%, 85.71%, and 68.42% respectively.
No statistically significant difference was found regarding the
distribution and internal enhancement of non-mass like cancer
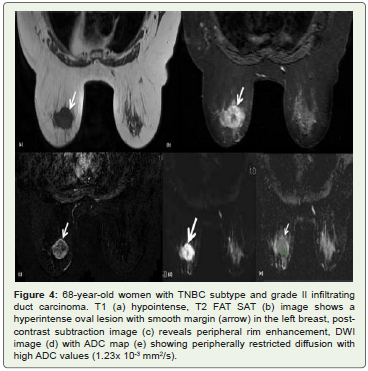
among the different subtypes, p=0.27.The intratumoral high signal
intensity on unenhanced fat-suppressed T2-weighted images was
identified in 16/22(72.73%) of TNBCs (Figure 4) which correspond
to morphologically and pathologically intratumoral necrosis,
as compared to 8/40(20%), 2/8(25%), 3/12(25%) in LA, LB and
HER2+subtypes, p=0.0003. No significant difference was identified among the Time-intensity curve analysis among different subtypes,
p=0.074. The visual detectability of the different subtypes at DWI was
not significantly different among tumor subtypes. ADC values were
significantly different among tumor subtypes, p=0.017, the mean ADC
value of TNBC was 1.28±0.23×10-3mm2/s which was higher than
that of LA (1.153±0.25×10-3mm2/s), LB (1.04±0.13×10-3mm2/s)
and HER2+ (1.14±0.18×10-3mm2/s).
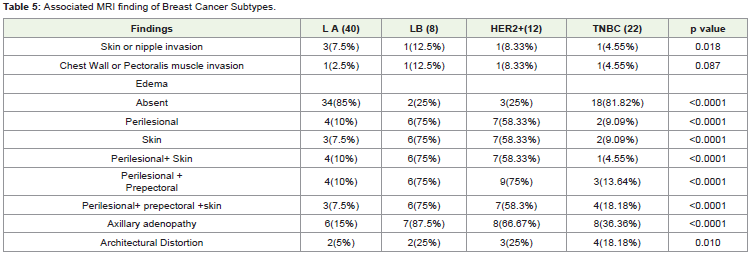
Among the associated features (Table 5) axillary adenopathy
was more common in LB (87.5%) as compare to HER2+(66.67%),
TNBC (36.36%), and LA (15%) with p=0.0001. Skin, perilesional
and prepectoral edema were more common in LB (75%) and HER2+
(58.33%) as compared to TNBC (18.18%) and LA (7.5%).
Discussion
Breast cancer with different molecular subtypes has a different
pattern of initial disease presentation and metastatic spread. Different
subtypes respond differently to radiation and chemotherapy [8,9].
Our study may help in guiding different MRI features helpful in
diagnosing molecular subtypes of breast cancer, which would further
improve the potential for presurgical personalized medical care.
In our study, we could not find significant age differences among
different subtypes as compared to previous study conducted by
Osman NM et al where it was found that TNBC was more common
at a younger age (43.1 ± 8.2) as compared to ER (45 ± 6.1) and HER2+
(47.4 ± 6.6) [10].
The present study showed that histologically high grade tumors
were more common in LB, HER2+ and TNBC subtypes as compared
to LA which was consistent with previous studies conducted by
Lacroix BM et al and Uematsu T et al. [11,25]
Luminal A tumors were more common in our study (48.78%),with
histological grade I (52.5%), presenting as a mass lesion with an
irregular shape, spiculated margin, and heterogeneous enhancement
along with type III curve. These observations were similar to the study
conducted by Youk JH et al [26]. Overall, Luminal A breast cancer is
associated with the most favorable prognosis, with a 5-year survival
rate of more than 80%. This excellent prognosis is in part because the
expression of the steroid hormone receptor is predictive of a favorable
response to hormonal therapy [16,17,18] .
Grimm et al. and Agarwal G et al. reported that multicentric
or multifocal disease was significantly more frequent in Luminal B
and HER2 positive tumors. These tumors were also associated with
axillary adenopathy, skin, perilesional, and prepectoral edema as
compared to LA and TNBC which indicate a more invasive behavior
and greater metastatic potential. The present study also shows similar
observations. Perifocal edema can often be detected around tumors
which are mainly caused by the immunohistopathologic response of
the body against tumors through emitting cytotoxic T-Cells natural
killer cells and macrophages. Tumor-associated macrophages (TAM)
are known to induce tumor angiogenesis by emitting vascular
endothelial growth factor. Prepectoral edema may be explained
pathophysiologically through the anatomy of the lymphatic drainage
pathway, indicating a possible correlation between prepectoral edema
and lymphatic spread. Blocked lymphatic trails and nodes could be
responsible for some sort of lymphatic obstruction within the breast
and explain the formation of pectoral edema [19,20,22].
HER2 nue overexpression may be linked with overall increased
tumor viability and a significant increase in the population of
visible hypoxic cells, leading to hypoxia inducible factor-2 alpha
overexpression which is related to high metastatic potential.
Identification of multifocal disease in the breast is important because
these findings may represent contradictions to breast conservation
therapy. Four (33.3%) of our HER2+ cases and two of LB (25.9%)
with HER2 enrich had microcalcification on mammography. It
is mentioned in the literature that calcification is encountered in
majority of HER 2 positive cancer whereas it is uncommon in triplenegative
breast cancer [21,22].
TNBC showed a high T2 signal intensity (72.73%) and rim
enhancement (55.54%) in our series as compared to 71.4% and
61.6% in the study conducted by Osman NM et al .The hyperintense
signal corresponded to intratumoral necrosis, which is a prognostic
factor in invasive breast cancer. It is reported that the presence of
moderate to marked central tumoral necrosis decreases relapse-free
survival and increases mortality in both patients with node-negative
and node-positive disease. Centrally necrotizing breast cancers were
characterized by early systemic metastasis and an accelerated clinical
course [10,25].
Two TNBC were hyperintense on T2WI without necrosis,
their histopathological analysis revealed that they were mucinous
carcinoma and was similar to the study of Osman NM et al. Uematsu
et al reported that 66% of TNBC were unifocal in contrast to 81.82%
in our study [25] Two medullary carcinomas were also of TNBC
subtype which is in agreement with previous study [25]. Two patients
of TNBC were BRACA I positive. One had associated ovarian
malignancy with hepatic and peritoneal metastasis.
TNBC subtype had high ADC value (1.28 ± 0.23) as compared
to other subtypes may be due to tumor necrosis causing increase
diffusion and higher ADC value, another explanation for increased
ADC value is that in ER positive tumors the ADC value becomes
less than in ER-negative as the estrogen receptors inhibit the tumor
angiogenesis decreasing perfusion and thus affecting the ADC value
[26-29].
In conclusion, MR imaging helps diagnose Luminal A tumors
which present as a mass with an irregular shape, spiculated margin,
and heterogeneous enhancement. TNBC presents several MRI
predictors on DCE-MRI such as unifocal, rim enhancing mass with
round or oval shape, smooth margin, center high signal intensity on
T2 weighted images, and higher ADC values on DWI. A multifocal
or non-mass lesion with lymph node involvement, skin, peritumoral
and prepectoral edema are more common in Luminal B and HER2
molecular subtypes breast cancer.
Strength and Limitation: We have taken different types of edema
patterns as well as ADC values of the tumors in the study along with
their morphological features on MR imaging which further helps in
the characterization of different molecular subtypes. This study has
less number of Luminal B and HER2+ subtype breast cancer. Further
studies are needed to see the specific pattern in these subtypes.
References
Citation
Issar P, Sinha S, Ravindranath M, Issar SK. MRI Features of Different Molecular subtypes of Breast Cancer. Indian J Appl Radiol. 2020;6(1): 151.