Case Report
Severe Hemorrhage Due to Rupture of Uterine Artery Pseudoaneurysm: Post Miscarriage of Scar Pregnancy: A Rare Case Report
Ashwini G*, Samra Q, Sanaa Badr, Arabo Bayo and Reda R Yousef
Department of Clinical Imaging, Women Wellness and Research Center (WWRC), Hamad Medical Corporation, Qatar
*Corresponding author: Ashwini G, Department of Clinical Imaging, Women’s Hospital, Hamad Medical Corporation, Doha, Qatar, Tel no: 00974-33544845; E-mail: Agujrathi@hamad.qa
Copyright: © 2020 Ashwini G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 21/11/2019; Accepted: 12/03/2020; Published: 16/03/2020
Abstract
Uterine Artery Pseudo aneurysm (UAP) is a rare cause of secondary postpartum hemorrhage but it is potentially life-threatening. It can occur after caesarean section, myomectomy or dilatation and curettage (D and C) [1,2].
We present a case of 20 years old lady with previous 2 C-sections presented with severe vaginal bleeding post D and C due to incomplete abortion of previous diagnosed Scar pregnancy. US color Doppler showed a pseudoaneurysm in the lower uterine cavity. Exploratory laparotomy was performed as patient was in hemorrhagic shock and Retained Products of Conception (RPOC) adherent to the scar were removed.
In order to avert life-threatening bleeding due to UAP prompt and accurate diagnosis should be made using color Doppler US, as it plays a significant role in demonstrating the vascular nature of this anechoic uterine lesion.
Keywords
Uterine Artery pseudoaneurysm; Postpartum hemorrhage; US Doppler; Uterine artery embolization
Introduction
Secondary post-partum hemorrhage is defined as excessive vaginal bleeding 24 hours to 6 weeks post pelvic intervention [3]. The most common causes are RPOC, sub involution of placental bed and
endometritis [4]. Rare causes include Pseudoaneurysm of Uterine Artery (UAP) or its branches, Arterio-Venous Malformations (AVMs) and choriocarcinoma [5-8].
Uterine Artery Pseudoaneurysm (UAP) is a rare cause of
postpartum hemorrhage. A Pseudoaneurysm is an extra-luminal
collection of blood with turbulent flow that has a small defect
connecting it to the vessel of origin. UAPs are known to occur
after C-sections or pelvic surgery [9]. Unlike true aneurysm,
pseudoaneurysm does not have the three layers of arterial wall lining
and they tend to be more common than true aneurysms.
UAP are either asymptomatic or present with symptoms such as
vaginal bleeding, abdominal pain, hypovolemic shock or fever when it
gets infected. Diagnosis is suspected on ultrasonography and contrast
-enhanced Computer Tomography (CT). Conventional angiography
confidently confirms the diagnosis.
Transcatheter uterine artery embolization is ideally the treatment
of choice. However, in case of acute hemorrhage emergency
laparotomy with packing, bilateral internal artery or uterine artery
ligation or in severe cases hysterectomy is performed [9,10].
Case Report
A 20-years old G3P2 woman (12 weeks by LMP) was brought to
our emergency with severe vaginal bleeding. On examination she had
past history of,
1) Previous 2 C-sections, last elective C-section was done 6
months ago for Placenta Previa Major with Accreta changes.
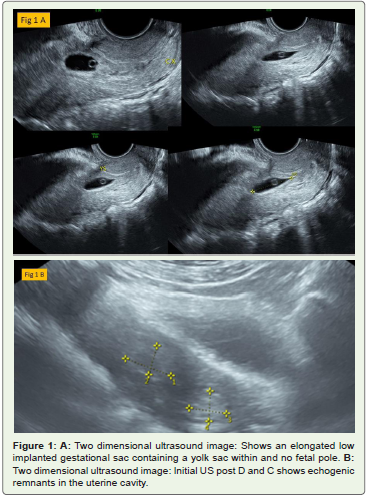
2) On ultrasound scan done at 4weeks in this pregnancy, showed
and confirmed a low implanted gestational sac (Figure 1A), She had
miscarriage with successive ultrasound showing incomplete abortion
(Figure 1B), for which ultrasound guided dilatation and evacuation
of products of conception was performed under spinal anesthesia .
There was active bleeding (EBL 1700ml) during the procedure and
evacuation of large products was done. Patient was given Methergine,
Tranexamic acid and IV Syntocinon. Bimanual compression was
done for 15 minutes and vaginal packs were kept for 12 hours. Her
hemoglobin level was 6 g/dl.
3) Four units of PRBC transfusion were done after which Hb
got increased to 8.9 g/dl. Patient was discharged on antibiotics with
minimal vaginal bleeding and stable vitals.
4) The surgical pathology report confirmed the products as
‘Retained Products of Conception’ (RPOC).
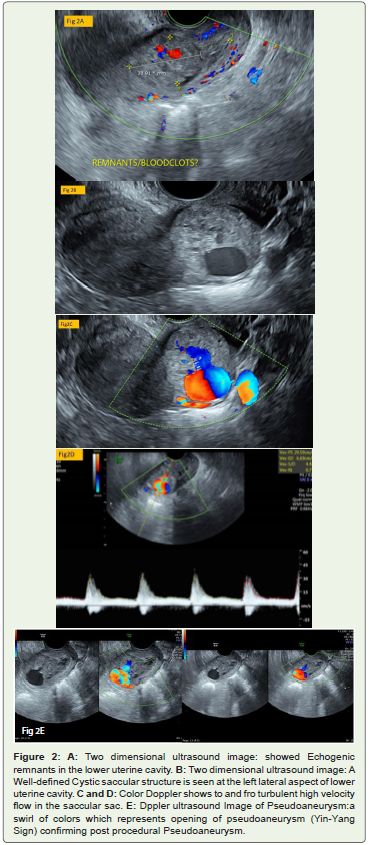
After 6 weeks of D & C patient presented to the emergency again with severe vaginal bleeding. Per vaginum examination showed no tissue or products. US was performed, and it showed mixed echogenic structure in the lower uterine cavity suggesting remnants along with a large cystic vascular saccular sac in the left lateral aspect
of the lower uterine cavity (Figure 2A and 2B). On color Doppler the sac demonstrated to and fro turbulent blood flow and Yin-Yang sign with high velocity waveforms (Figure 2C-2E). These imaging findings suggested post procedural pseudoaneurysm formation with remnants.
Patient was clinically stable. Patient was admitted and MRI
,embolization were scheduled the following day. she suddenly started
severe bleeding and lost about 2 liters (total loss of over 3 liters) of
blood. On call Doctor was informed about the patient. The patient
was taken to the operation theatre for examination under anesthesia
and further management.
While in theatre, she bled profusely due to rupture of aneurysm,
losing about 4 liters of blood in theatre with sudden stoppage of
bleeding.
Emergency Exploratory laparotomy was done. During the
surgery, there were extensive omental adhesions and obliteration
of vesicovaginal pouch with thick band of adhesions. After careful
dissection of these adhesions, an area of bluish necrotic tissue was
found at the lower part of the uterus, at the cesarean scar site. It was
found to be a 3 cm mass of placental tissue with some vasculature
around it occupying the cesarean scar, which was partly into the
uterine cavity and partly projecting outwards. This mass was resected
out, hemostasis was achieved and the resected mass was sent for
histopathology.
Surgical pathology report came as: confirmed products of
conception. Patient was discharged home in a healthy condition.
Discussion
UAPs can present with heavy uncontrollable vaginal bleeding and
cause significant morbidity and mortality. Its accurate diagnosis and
prompt treatment is pertinent to reduce the morbidity.
Gray scale ultrasonography is the first noninvasive diagnostic
modality which shows a pseudoaneurysm as an anechoic saccular
lesion. Ultrasound Color Doppler demonstrates turbulent high
velocity arterial flow with a characteristic to-and-fro pattern (Yin-
Yang sign) [11,12]. US have a diagnostic sensitivity of 97% [13].
Computed Tomography (CT) and Magnetic Resonance Imaging
(MRI) also aid the diagnosis. Angiography remains the standard
method for the diagnosis of UAP and may help in the design of
definitive treatment strategies.
The choice of the therapeutic option depends on the risk of
severe hemorrhage and the possible adverse events. Initial treatment
should include volume replacement and blood transfusions, as well as
vaginal or uterine packing. If bleeding persists, other options include
hysterectomy, surgical uterine artery ligation, or selective uterine
artery embolization.
Uterine artery embolization has become an effective and safe
treatment for postpartum hemorrhage, allowing the preservation
of reproductive function [14]. Recent reports described the use
of thrombin injection directly into the pseudoaneurysm under
ultrasound guidance, as a substitute for arterial embolization; however,
its indications and effectiveness have not yet been determined [15].
The surgical approach may be more suitable in cases of acute and
massive bleeding in which there is no time for embolization and may
depend on the specific resources available. Hysterectomy is one of the
surgical options when the preservation of fertility is not important. On the other hand, uterine artery ligation and extirpation of UAP is
another surgical choice for preserving fertility.
Conclusion
Follow up is necessary in case of scar pregnancy to look for retained
products of conception and if any pseudoaneurysm formation.
Delay in diagnosis of pseudoaneurysm could be life threatening.
Ultrasound and Doppler study should be performed on follow up
visits to rule out pseudoaneurysms which can save patients life and
resort hysterectomy if time allows.
References
Citation
Ashwini G*, Samra Q, Sanaa Badr, Arabo Bayo and Reda R Yousef. Severe Hemorrhage Due to Rupture of Uterine Artery Pseudoaneurysm: Post Miscarriage of Scar Pregnancy: A Rare Case Report. Indian J Appl Radiol. 2020;6(1): 148.