Case Report
A Rare Case of Omphalocele with Multiple Complex Congenital Anomalies in Intrauterine Fetus
Anusha G1, Baru RR1, Vedaraju KS1 and Samireddypalle Y1*
Department of Radiology, Narayana medical college, Nellore, Andhra Pradesh, India
*Corresponding author: Samireddypalle Y, Department of Radiology, Narayana Medical College, Nellore, Andhra Pradesh, E-mail: yugu.samireddypalle@gmail.com
Copyright: © 2020 Anusha G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 27/09/2019; Accepted: 13/01/2020; Published: 16/01/2020
Abstract
In recent times with development of advanced ultrasound equipment and techniques early detection of various fetal anomalies are made easier.
Dedicated sonographic technique and interpretation is necessary for early diagnosis of various anomalies. Omphalocele is a type of anterior abdominal
wall defect, which is an infrequently reported rare congenital deformity, if detected earlier can help in emergency intervention which can be carried out for
a better integrated management for fetus, Mother and family. Special importance needs to be made for Omphalocele as they are associated with multiple
other jeopardizing congenital defects leading to poor prognosis. In this case report, we present antenatal imaging findings & gross fetal specimen correlation
of fetus of a 21 week primigravida with Omphalocele, Cleft lip and cleft palate, Ebstein’s anomaly with hypoplastic left heart, Enlarged posterior fossa of
brain with hypoplastic cerebellum and vermis, Large cisterna magna, Hypoplastic orbits and enlarged hyperechoeic kidneys. Of all the investigations,
ultrasonographic assessment of fetal structure and well being is most reliable along with other investigations like genetic screening. The lack in the dedicated
antenatal examination and poor compliance for routine antenatal checkups leads to a large proportion of undiagnosed cases. Marked reduction in perinatal
morbidity and mortality and avoidance of stigma faced by the parents can be achieved by early detection and proper management.
Keywords
Omphalocele; Congenital deformities; Gastroschisis
Introduction
Anterior abdominal wall defects are a group of rare congenital
deformities. The incidence of Omphalocele, Gastroschisis, and
Exomphalos are worth noting as they frequently turn out to be fatal
for the neonates [1]. Special attention should be made Onomphalocele
as multiple lethal congenital defects are associated with it which leads
to poor prognosis [2].
Omphalocele has been reported to have an incidence of 2-3 in
10,000 pregnancies [3,4]. It is considered to be a defect in regression
of the normal physiological umbilical herniation of abdominal
content during 6th to 10th week of gestation [4]. The major three
diagnostic investigations are targeted fetal anomaly scan for detecting
anomalies, echocardiography for detection of various associated
lethal cardiac anomalies and lastly karyotyping to detect various
chromosomal anomalies which are very often associated with it.
Targeted fetal anomaly scan has been the primary imaging modality
for the diagnosis and can be used for early identification of the cases
by 10th to 12th week of gestation [5].
In developing country like India, where there is lack of perception
for routine antenatal checkups among gravid women and lack of
proper management of such cases, we have to come up with ideas
to increase the efficiency of primary health centres and other health
organizations. The strategic measures to be achieved are dedicated
ultrasound examination, Proper family history and Routine followup
examination to assess fetal well-being, awareness programs, and
possible genetic screening. A few viable fetuses may be considered,
after dedicated assessment, and can be allowed for the continuation
of pregnancy with proper surgical and medical follow ups to limit
associated complications in such cases. With this marked reduction
in perinatal morbidity and mortality can be achieved. We herein
report a case of a single live fetus with Omphalocele and multiple
associated congenital abnormalities.
Case Report
Written informed consent was taken from the parents of the fetus.
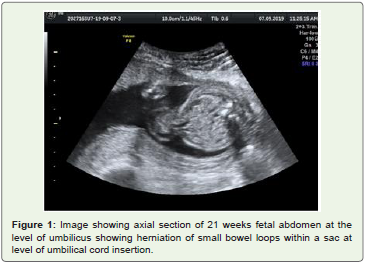
A 20 yr old female of gestational age around 22 weeks came for routine fetal anomaly scan. The anomaly scan showed a single live intrauterine fetus corresponding to gestational age 21 weeks 3 days
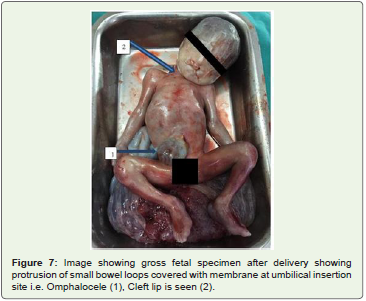
with multiple anomalies as follows: a midline fetal abdominal wall
defect is noted at base of umbilical cord insertion with herniation
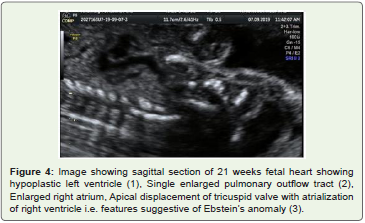
small bowel loops covered with a sac i.e. Omphalocele Fetal echo
demonstrates Hypoplastic left atrium and left ventricle, Right atrium
is enlarged with apical attachment of tricuspid valve (Atrialization
of right ventricle), Single pulmonary trunk is identified from right
ventricle i.e. Ebstein’s anomaly with hypoplastic left heart. A vertical
hypo-echoic region is noted through upper lip in angled coronal view
and similar defect is noted in the hard palate in axial plane, i.e. cleft lip
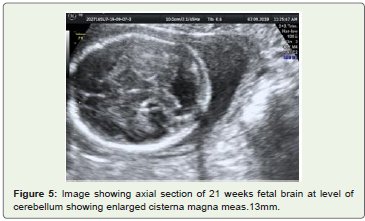
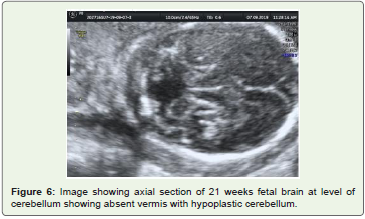
and palat. In brain there is enlarged posterior fossa with hypoplastic
cerebellum and absent vermis, Note is made of enlarged cisterna
magna meas. 13mm. Bilateral kidneys are enlarged and echogenic.
Both orbits are small and hypoplastic. No neural tube defects are
noted (Figures 1-6).
Discussion
Improper closure or absence of midline anterior abdominal wall which may leads to herniation of abdominal contents which results
in Omphalocele. According to position of defect they are subdivided
into epigastric, Central and infraumbilical omphalocele of which
central type is the most common [1]. Studies have showed a strong
association of chromosomal abnormalities (69%) with central type of
defect of which Trisomy 18 was most frequently noted [2]. Very few
patients with such central defect were associated with good prognosis
(8%) [1].


Some suggest that Omphalocele may occur due to the failure of
the medial segments of the two lateral embryonic wall folds to fuse at
approximately 3-4 weeks post conception. This defect at the umbilical
ring allows the abdominal content to herniate into a sac comprised of
an outer layer of amnion and an inner layer of peritoneum and often
Wharton’s jelly. General pathogenesis includes teratogenic effects by
early pregnancy use of anti thyroid drugs.
Omphalocele (1 in 4000) is rarer than Gastroschisis (1 in 2000)
[5]. Etiopathogenesis of Omphalocele and Gastroschisis are debatable
and have different theories for origin. Gastroschisis is believed
to be formed due to defect in the closure of lateral body wall folds
comprised parietal layer of lateral plate mesoderm and overlying
ectoderm during the 4th week of gestation [4]. Omphalocele is highly
associated with anomalies, and more often small Omphaloceles are
more often associated with anomalies. It is associated with multiple
chromosomal anomalies like Trisomy 18 (most common), Trisomy
13, Trisomy 21, Turner syndrome, Klinefelter syndrome and Pallister
killian syndrome. Other syndrome associations are Beckwith-
Wiedemann syndrome, Pentalogy of Cantrell, OEIS complex
(Omphalocele, Bladder/cloacal exstrophy, Imperforate anus, spinal
anomalies) Lethal Omphalocele- cleft palate syndrome.
After studying 827 cases of Omphalocele from the year 1996 to
2006, Deng et al. established that 52.4% of pregnancies terminated
with late fetal death with upward trend in successive years and 37.4%
resulted in early neonatal death [2]. The incidence of nonisolated
Omphalocele (27.9%) was very less compared to isolated cases
(72.1%) evidencing the lesser incidence of syndromic feature of the defect supporting the rarity of our case [2]. The mortality rate for
patients in the gestational age of 28-36 weeks was 2.42 times higher
than 37-42 weeks and hence earlier diagnosis will give us increased
chances toward effective management of more cases well within time
[2].
It is associated with various other fetal gastrointestinal anomalies
which confer a poor prognosis, fetal anomalies, fetal cardiac anomalies
can occur in 50% of cases, Fetal genitourinary anomalies like bladder
exstrophy and cloacal exstrophy and fetal skeletal anomalies like
Omphalocele-radial ray (ORR) complex.
Higher morbidity and mortality rates are associated with
Omphalocele than a Gastroschisis, Primarily due to a higher
incidence of associated congenital anomalies. Smaller Omphaloceles
are thought to carry a worse prognosis due to increased risk of
associated abnormalities.
Mortality rates can approach 80% when associated anomalies are
present and increase to ~100% when chromosomal or cardiovascular
anomalies exist. However, If found in isolation, then the associated
mortality rate decreases to ~10%.
Of all the available investigations, Ultrasonographic assessment
of fetal structure and well being is most reliable but the lack in the
proper examination and infrequent routine checkups leads to a large
proportion of undiagnosed cases. Only about 39.3% of cases are being
diagnosed in the health centers and the rest 60.6% are confirmed by
physical examination after birth [2]. Proper awareness and proper
diagnosis are required to prevent morbidity and social burden on
patient’s family.
Conclusion
Omphalocele is a rare congenital anterior abdominal wall
abnormality associated with multiple congenital anomalies which
effects infant mortality and quality of life. Timely diagnosis of this
entity and evaluation of other associated anomalies is necessary,
which will help in implementation of the optimal treatment protocol
and elective termination of the pregnancy. Due to lack of awareness
and proper diagnosis, more efficient training of health practitioner,
Meticulous reporting, Utilization of modern diagnostic tools such as
advanced ultrasound examination and genetic screening should be
implemented to reduce the perinatal morbidity and mortality.
References
Citation
Anusha G, Baru RR Vedaraju KS, Samireddypalle Y. A Rare Case of Omphalocele with Multiple Complex Congenital Anomalies in Intrauterine Fetus. Indian J Appl Radiol. 2020;6(1): 144.