Case Report
Aggressive Angiomyxoma - A Bizarre Tumor of Pelvis
Venkatesh M1*, Sindhuja KLN1, Basha SU2 and Priya J3
1Radiology, Narayana medical college, Nellore, India
2Radiology, SVMCH, Pondicherry, India
3Pathology, Narayana medical college, Nellore, India
*Corresponding author: Venkatesh M, Radiology, Narayana medical college, Nellore, India
Copyright: © 2019 Venkatesh M, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 31/08/2019; Accepted: 31/10/2019; Published: 02/11/2019
Introduction
Aggressive Angiomyxomas (AA) are rare infiltrative mesenchymal
neoplasms that show local recurrence. They are benign tumors with
strong preponderance in the reproductive age women in the pelvic
and perineal regions. Due to its location, examination findings and
rarity it can be misdiagnosed as other gynecological malignancies/
groin hernias. The term aggressive is a misnomer due to its nature
of local recurrence and local infiltration. Wide local excision of the
tumor is the treatment of choice.
This case report presents a rare infiltrative mesenchymal
neoplasm of reproductive age group women with complaints of mass
per vagina.
Case Report
A 32year old female came with complaints of low back pain, mass
descending per-vagina, difficulty in micturition and dyspareunia. On
examination a non-tender, reducible mass arising from the posterior
urethral wall extending up to the left labia-major a with positive cough
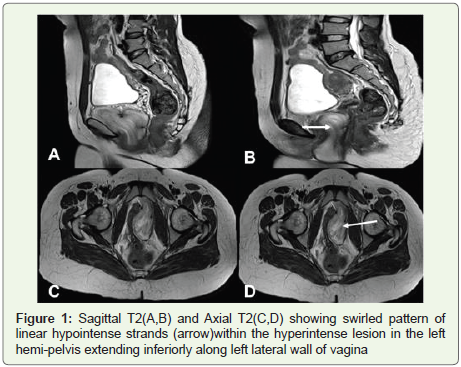
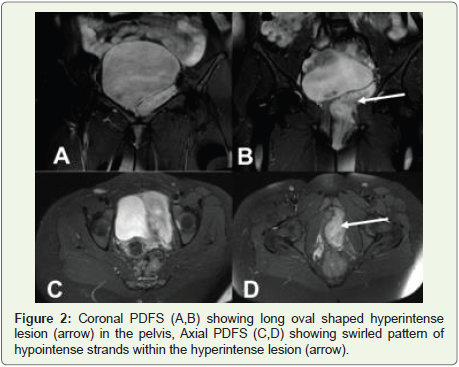
impulse was noted. Patient underwent MRI pelvis showed a welldefined
T2, PDFS iso-hyperintense heterogeneous signal intensity
lesion, T1 hypo intense lesion of size 6X4X3. 7 cm with characteristic
swirled pattern in the left hemi pelvis extending inferiorly along the
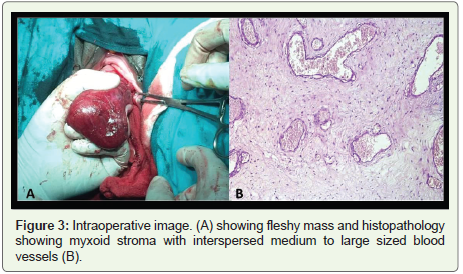
left lateral wall of vagina (Figure 1 and 2). Patient underwent wide
local excision of lesion. Histopathological examination revealed
myxoid stroma with interspersed medium to large sized blood vessels
suggestive of Aggressive Angiomyxoma (Figure 3).
Discussion
Aggressive angiomyxomas are rare infiltrative mesenchymal
neoplasms that commonly-recur locally. The term aggressive is a
misnomer suggesting its high local recurrence after resection and not of any malignant characteristics of the lesion [1,2].
The female-to-male ratio has been reported as 6.6/1 [3].
Aggressive angiomyxomas mainly affect women of reproductive
age with a peak incidence in the fourth to fifth decades of life [1,4].
It was first described in 1983 by Steeper and Rosai [5]. Aggressive
angiomyxoma is an uncommon mesenchymal tumor which is mostly
derived from the pelvic and perineal regions including vulva, vagina,
bladder, and rectum [6,7]. However uncommon locations have also
been reported like lung, liver, larynx, and orbit [8].
The main pathogenesis proposed by Nucci and Fletcher suggested
that a translocation at the level of chromosome 12 is responsible
where the high mobility group protein HMGA2 is located [9].
Aggressive angiomyxoma is regarded as an aggressive tumor
due to neoplastic nature of blood vessels, its high tendency of local
infiltration and local recurrence. It is a benign tumor, but a few cases
with metastasis to lungs causing death have been reported. It can
be distinguished from the other lesions by its immunohistological
findings. AA is derived from myofibroblasts as a phenotypic variant
of the basic fibroblast with a prominent vascular component.
Immunohistochemical staining of the tumor reveals high positivity
for desmin, vimentin, ER, and PR receptor; however, it usually reveals
negativity for S-100 protein [6,8].
The tumor tends to grow around the structures of the pelvic
floor without penetrating the muscular is of the vagina or rectum
[10]. Angiomyxoma remains asymptomatic until the tumor reaches
large size. Urinary, gynecologic and gastro-intestinal symptoms
like dysuria, dysmenorrhea, constipation, and chronic abdominal/
pelvicpain occur when the tumor begins to compress the adjacent
organs including bladder, rectum, ureter, and uterus. . It is presented
as painless mass in genito-femoral region or as a mass causing local
pressure effect. For this reason, it is often misdiagnosed as vaginal
prolapse, Bartholin’s gland cyst, vulvar abscess, gynecological
malignancy, femoral/groin hernia which leads to unnecessary surgical
interventions.
Pre-operative imaging plays an important role in the diagnosis of
aggressive angiomyxoma. On USG it appears as a hypoechoic cystic
mass and is not of diagnostic importance. On CT it appears as a welldefined,
hypoattenuated enhancing mass with swirling appearance in
only 83% of patients [11]. MRI is more helpful than any other imaging
modalities to characterize and to determine the extent of lesion. On
T1W images, it appears isointense, on T2 it appears hyperintense
due to high myxoid matrix and high water content [11]. Imaging
not only helps in diagnosis but also helps in planning for surgery.
Dynamiccontrast-enhanced MRI may be beneficial and helps to
better understand tumor hemodynamics. Other non-specific findings
may be internal cystic changes, background laminated appearance,
large internal vessels.
In our case, the lesion was is to hypointense to the adjacent muscle
on T1W, characteristic swirled pattern of linear hypointense strands
within hyperintense lesion on T2W with similar appearance on PDFS.
Reproductive age group woman, with painless mass descending pervagina
with characteristic swirled appearance on MRI helped in the
diagnosis of Aggressive Angiomyxoma.
The characteristic MR imaging appearance of Angiomyxoma
may aid in the differential diagnosis. The differential diagnosis of a
pelvic or perineal softtissue mass in an adult female patient includes
angiomyofibroblastoma, myxoma, infiltrating angiolipoma and
myxoid lipoma. On DWI and FDG PET/CT reflects the low mitotic
activity of Aggressive Angiomyxoma.
The main choice of treatment remains complete surgical excision
alone with the tumor free margins. The rate of recurrence varies
from 33% to 83%. Recurrence has been mostly occurred within 3
years of post-operative period3 .The patients having positive margins
have more chances of recurrence than those with negative margins.
Incomplete/partial excision, distant metastasis in some cases also
have possibility of recurrence. In our case, wide local excision of
the lesion was done with no recurrence till date. Few of the surgical
complications may be present like infertility, colostomy.
Chemotherapy has no beneficial results for adjuvant therapy.
Embolization remains insufficient due to vascular network of tumor.
Pertaining to the reproductive organ of origin, positive ER and PR
status, considering it as hormone responsive neoplasm, Tamoxifen or
gonadotropin releasing hormone agonist had some beneficial effect
[6,12].
Conclusion
The reproductive age of the women with painless swelling
in the genito-femoral region, pressure symptoms must raise the
suspicion of Aggressive Angiomyxoma. The clinical symptoms and
examination may mislead the diagnosis as gynecological malignant
lesions or groin/femoral hernias. Imaging with MRI plays a major
role in confirming the diagnosis by its characteristic swirled pattern
on T2W. Conservative en-bloc resection with microscopic positive
margins achieves good local control. Histopathological correlation
confirms the diagnosis.
References
Citation
Venkatesh M, Sindhuja KLN, Basha SU, Priya J. Aggressive Angiomyxoma - A Bizarre Tumor of Pelvis. Indian J Appl Radiol. 2019;5(1): 142.