Research Article
Role of Sclerotherapy in the Management of Various Types of Vascular Anomalies in a Tertiary Health Care Center
Sharma N* and Sharma MS
Department of Radiodiagonisis, SRMS-IMS, India
*Corresponding author: Sharma N, Department of Radiodiagonisis, SRMS-IMS, Bhojipura, Bareilly, India
Copyright: © 2019 Sharma N, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is is properly cited.
Article Information: Submission: 03/07/2019; Accepted: 10/10/2019; Published: 14/10/2019
Abstract
Introduction: In the population the vascular malformations are around 4.5%. These malformations can be classified into arterial malformations, venous
malformations, arterio-venous malformations, lymphatic malformations, and capillary malformations and combined vascular defects.
Aims and objectives: To study the Role of sclerotherapy in the management of various types of vascular anomalies at a tertiary health care center
Methodology: This was a cross-sectional study carried out in the department of Interventional Radiology of a tertiary health care centre during the six
month period i.e. august 2018 to January 2019. In the six month period there were 50 patients enrolled for study. Patients had undergone Sclerotherapy
with sodium tetradecyl sulfate alone (Group A) (n=25) versus sodium tetradecyl sulfate and lipiodol (Group B) (n=25) randomly. The statistical analysis was
done by SPSS 19 version software.
Result: The majority of the patients in the age group of <10 years were 46%, followed by 10-20 years were 30%, 20-30 years were 14%, 30-40 years
were 10%. The majority of the patients were Females i.e. 64% and males 36%. The various sites of vascular malformations found were Upper limb extremity
in 38%, followed by Head and Neck in 28%, Lower limb extremity in 16%, Buttocks in 10%, Genital area in 8%.The majority of the patients with successful
Sclerotherapy in first attempt were in Group B i.e. 38% as compared 24% in Group A while 26% in Group A versus only 10% in Group B patients required
Re-embolization. This observed difference was statistically significant (X2
=5.11, df=1, p<0.02).No major complications were found in our study but the mild
complications were comparable in both the groups (X2
=0.46, df=6, p>0.05)
Conclusion: It can be concluded from our study that both the groups of sclerosants were effective in the treatment of various malformations but
success in first attempt was more to combined sodium tetradecyl sulfate and lipiodol versus sodium tetradecyl sulfate alone and both the groups were having
comparable complications
Keywords
Sclerotherapy; Vascular Anomaly; Sodium tetradecyl sulfate; Lipiodol
Introduction
Vascular anomalies are congenital anomalies categorized into
vascular tumor and vascular dysmorphogenesis (Vascular anomalies).
The Vascular Malformations (VMs) are found in 4.5% of the
population [1]. These malformations can be classified into Arterial
Malformations (AMs), Venous Malformations (VMs), Arterio- Venous Malformations (AVMs), Lymphatic Malformations (LMs),
and Capillary Malformations (CMs) and combined vascular defects.
These malformations are known to manifest in all parts of the human
body. In addition, these malformations are present at birth; that is,
they are congenital, but they usually induce clinical symptoms and
findings after childhood, in early adulthood, or in later stage of life
by the influence of various factors such as trauma, infection, or hormones [2-4]. Diagnosis of a vascular malformation is primarily
clinical, but ultrasound and especially Magnetic Resonance Imaging
(MRI) has an important role [1]. Treatment options can include
minimal therapies such as elevation, compression garments, and
aspirin whereas medical management of LMs can require antibiotics
and steroids [5].
Sclerotherapy has become an important tool in the treatment of
vascular malformations. However, there has not been any evidence to
suggest that any single sclerosing agent is more effective than others
in clinical trials; thus the radiologist’s personal preference does play a
role in the selection of the sclerosing agent [6].
Sclerotherapy refers to the introduction of a sclerosing agent into
the lumen of a vessel producing endothelial damage, which leads
to thrombosis and subsequent fibrosis. It has been extensively used
in the management of superficial varicose veins and other venous
abnormalities [6,7].
Sclerotherapy is the injection of a chemical solution (sclerosant)
into a vein, damaging the endothelial lining and causing vessel
occlusion and the development of fibrous tissue [8].
Sclerosing solutions are classified into three groups, based on the
mechanism of action - detergent agents, osmotic agents and chemical
irritants. The various sclerosants include STS (Sodium Tetrodecly
Sulfate), polidocanol, hypertonic saline, sodium morrhuate, etc. It
causes destruction of endothelium by altering the surface tension
around the endothelial cells by a process known as protein theft
mechanism [9].
So we have studied the role of Sclerotherapy in the management of
various types of vascular malformation at tertiary health care center.
Methodology
This was a cross-sectional study carried out in the department
of Interventional Radiology at Jawaharlal Nehru Medical College &
Acharaya Vinoba Bhave Rural Hospital, Sawangi (Meghe), Wardha
during the six month period i.e. august 2018 to January 2019. Patients
of all ages and both sexes were included in the study. Patients with
vascular anomalies diagnosed on Ultrasonography, MRI or CT were
included. Poor surgical candidate were excluded from our study.
In the six month period 50 patients with various types of vascular
malformations all over the body were diagnosed and enrolled in the
study with written and informed consent. Each patient underwent all
routine investigations including CBC, PT-INR, KFT, HbsAg, HCV
and HIV. Each patient was subjected to Angiography of the affected
limb under standard protocol. The arterial and venous tributaries were
documented along with the geography of the lesion. Sclerotherapy
was then done with sodium tetradecyl sulfate alone (Group A)
(n=25) versus sodium tetradecyl sulfate and lipiodol (ethiodized oil)
(Group B) (n=25) randomly. Patients were followed up frequently
(5 days, 15 days, 1 month and later if needed) and re-embolization
(re-sclerotherapy) was done in patients when needed. The various
complications if any were noted. Procedure was performed on Philips
Aurora FD 20/10 machine. In patient where only STS was used as an
embolizing agent, doses between 0.5 ml to 2 ml were used, where in a
2 ml syringe STS was mixed with contrast medium slowly (No foam preparation). In patient where sclerotherapy was performed using
STS and lipiodol, 0.5 ml lipiodol and 2 ml Setrol was mixed slowly in
2-3 ml syringes and used for sclerotherapy. The procedure was done
under fluoroscopy. The peripheral vascular anomalies were punctured
per-cutaneously using scalp vein 23/24 in number. After puncturing
the vascular lesion, contrast shoot was taken to characterize the lesion
and its boundaries. Contrast was then aspirated back using the same
syringe. Sclerotherapy was then started by connecting the syringe
containing sclerosant to scalp vein. Agent was injected in the form
of pulses under fluoroscopy. Sclerotherapy was stopped before the
agent entered deep vessels. The statistical analysis was done by SPSS
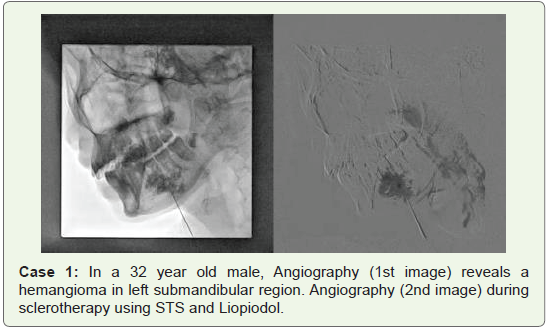
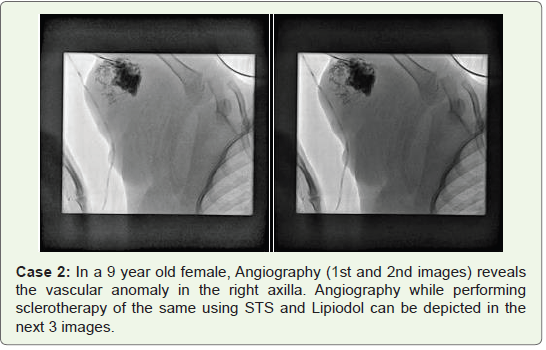
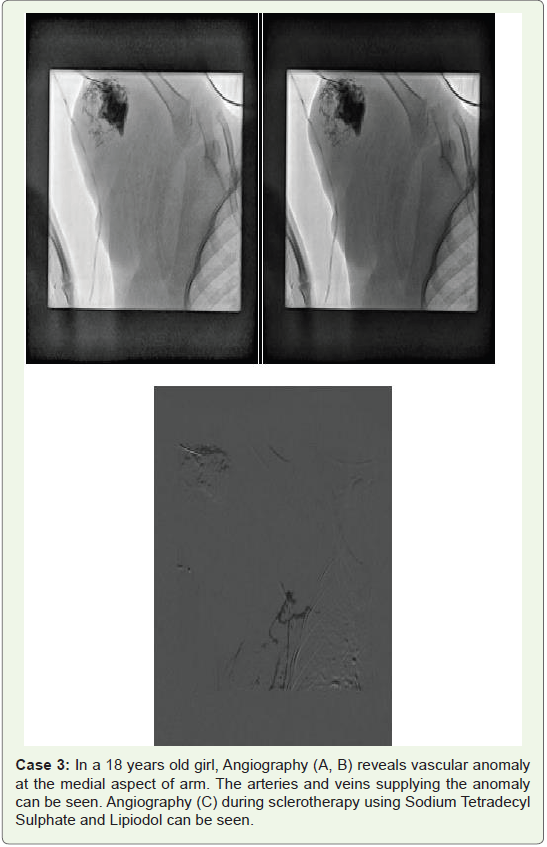
19 version software (Cases 1-3).
Result
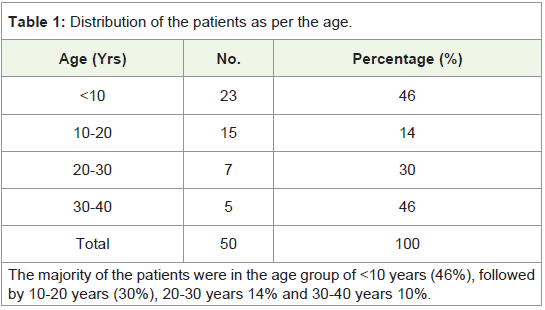
(Table 1) The majority of the patients were in the age group of
<10 years (46%), followed by 10-20 years (30%), 20-30 years 14% and
30-40 years 10%.
(Table 2) The majority of the patients were Females i.e. 64% and
males 36%.
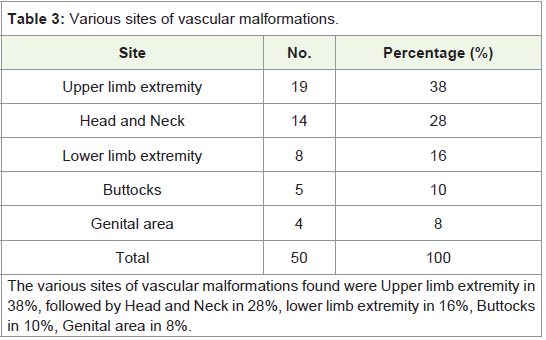
(Table 3) The various sites of vascular malformations found were
Upper limb extremity in 38%, followed by Head and Neck in 28%,
lower limb extremity in 16%, Buttocks in 10%, Genital area in 8%
(Table 4).
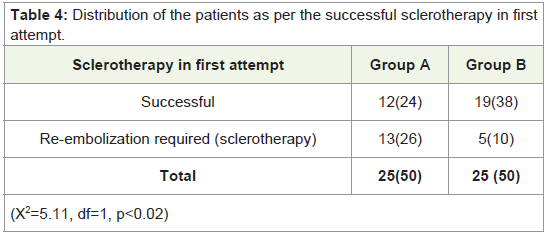
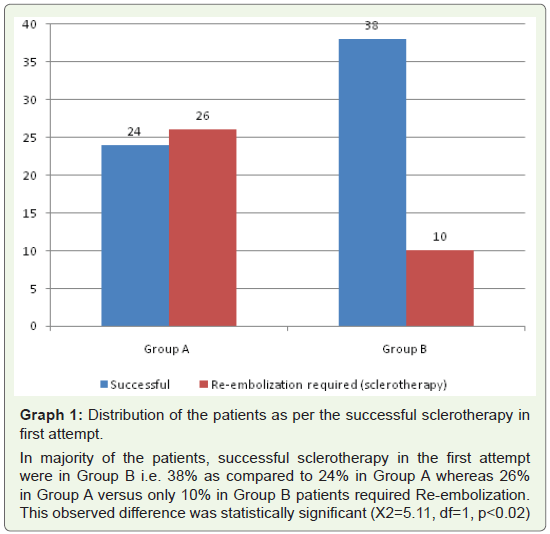
(Graph 1) In majority of the patients, successful sclerotherapy
in the first attempt were in Group B i.e. 38% as compared to 24% in Group A whereas 26% in Group A versus only 10% in Group B patients required Re-embolization. This observed difference was
statistically significant (X2=5.11, df=1, p<0.02
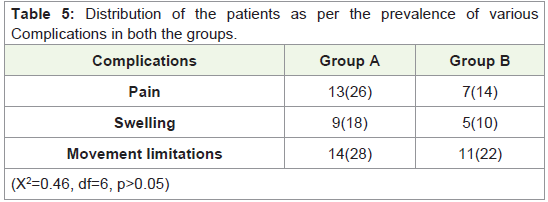
(Table 5) No major complications were found in our study. Only
the minor complications like pain and swelling at embolization site
and limitation of movements were seen in both groups, in whom Pain
was found in 26% and 14%; Swelling in 18% and 10% and Movement
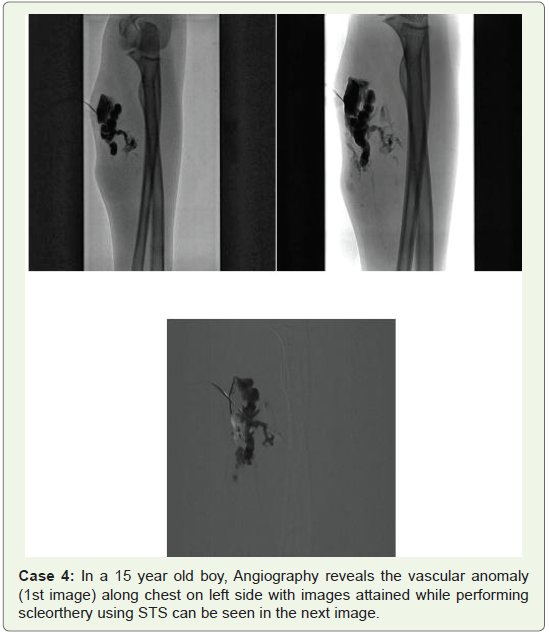
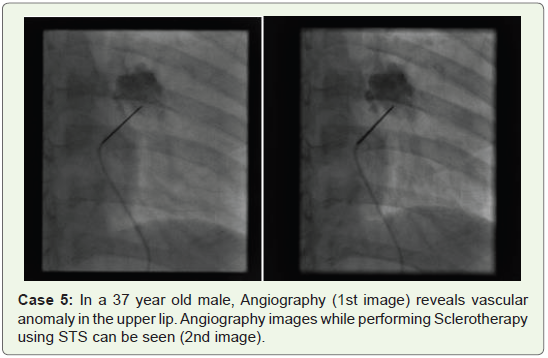
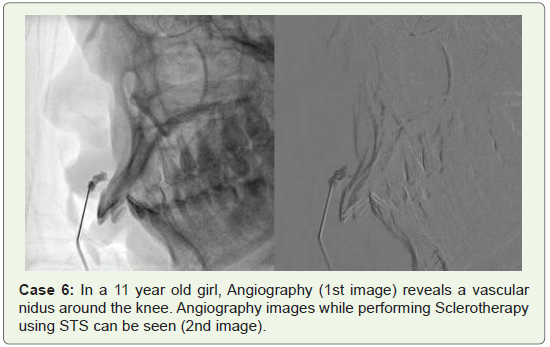
limitations in 28% and 22% in Group A and Group B respectively, but the complications were comparable in both the groups (X2=0.46, df=6, p>0.05) (Cases 4-6).
Discussion
Vascular malformations being true in-born errors of development
in the vascular tree are all present since birth, though all may not be
clinically apparent [10]. The commonest of all the vascular anomalies
are the venous malformations with a higher propensity for the head
and neck region [10]. They can cause pain, bleeding, restriction
of movement, pressure on adjacent structures, consumptive
coagulopathy and aesthetic concern. They can either be discrete or
extensive. The overall incidence of venous malformations is reported
to be 1-4% of the population with no sex predilection. They are usually
singular, isolated presentations but may occur in multiple areas. They
may clinically manifest in infancy, childhood, adulthood or they may
remain asymptomatic throughout life. Unlike hemangiomas they do
not regress and grow correspondingly as the child develops. Venous
malformations may occur in solitary form or they may be combined
with capillary or lymphatic malformations. The microscopic
examination reveals dilated vascular channels in proliferation lined by normal flattened endothelial with normal mast cells count. These
endothelial cells characteristically have normal turn-over rate. MRI
is the best investigation for venous malformations and gives off
decreased signal intensity on the T1-weighted image hyperintense
signal intensity on the T2-weighted image [11].
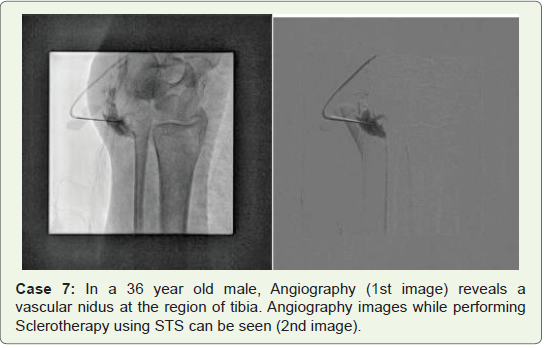
MRI can distinguish low-flow venous malformations from highflow arterio-venous malformations and fistulas. It can also provide
information about delineation of the neurovascular structures and
their involvement with the malformations (Case 7).
Management of venous malformations is quite challenging
because treatment carries a significant risk of morbidity and the
recurrence. Surgical resection, though definitive treatment, is often
not feasible except for smaller lesions because of deeper involvement
of neurovascular structures particularly in the head and neck and
extremity malformations. Recurrence of Incompletely excised lesions
is very frequent.
Laser treatment of venous malformations has also been attempted
with varying success rate. Laser photocoagulation with argon, NdYag or combination lasers have been found to be somehow effective
for tiny superficial venous or capillary-venous lesions but not for
significantly sized lesions. Recurrence is common and often repeated
treatments are necessary. Hence they may be useful in select group of
patients [11,12].
Sclerotherapy alone or in combination with surgical excision
is now the accepted modality of treatment in symptomatic venous
malformations. Localized areas can be treated without an incision
and diffuse, extensive lesions may be symptomatically palliated.
Conservative management with numerous sclerosing agents (boiling
water, alcohol, sodium morrhuate, quinine, urethan, silver nitrate,
iron, zinc chloride, liquid vegetable protein) have been used since the
18th century for the treatment of a wide variety of vascular anomalies
[8,10-14].
In 1946, Sodium Tetradecyl Sulfate (STS) was introduced in,
and it is still widely used today. Over 13,000 patients treated by STS
were reported by George Fegan in the 1960s, significantly advancing
the technique by concentrating on fibrosis of the vein rather than
thrombosis, focusing on controlling significant points of reflux, and
emphasizing the importance of compression of the treated limb
[15]. The procedure became medically accepted in mainland Europe
during that time. However it was poorly understood or accepted in
England or the United States, a situation that continues to this day
amongst some sections of the medical community [16].
Lipiodol (labeled Ethiodol in the USA), also known as ethiodized
oil, is a poppy seed oil used to outline structures in radiological
investigations by injection as a radio-opaque contrast agent [17,18].
It is used in chemo-embolization and as a contrast agent in follow-up
imaging [19,20]. Lipiodol is also used in lymphangiography [21-22].
It has an additional use in gastric variceal obliteration as a dilutant
that does not affect polymerization of cyanoacrylate.
Comopsition of ethiodized oil is ethyl esters of fatty acids of poppy
seed oil, primarily as ethyl mono and di-iodostearate combined
with iodine. The precise structure is unknown. Lipiodol was first
synthesized in the Paris School of Pharmacy in 1901 by Marcel
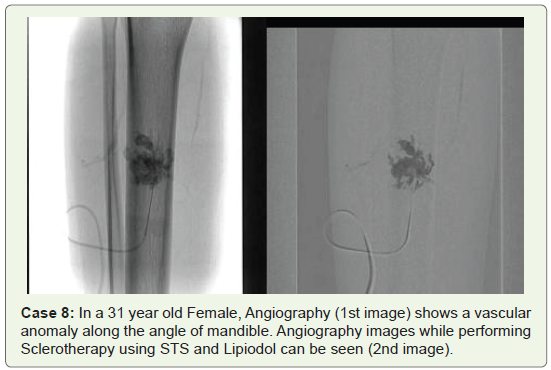
Guerbet. Historically, Lipiodol was the first iodinated contrast agent
(used for myelography by two French physicians, Jacques Forestier
and Jean Sicard in 1921) (Case 8)
In our study the majority of the patients were in the age group
of <10 years (46%), followed by 10-20 years (30%), 20-30 years were
14% and 30-40 years were 10%. The majority of the patients were
females in my study i.e. 64% and males were 36%. The various sites
of vascular malformations found were Upper limb extremity in 38%,
Lower limb extremity in16%, Head and Neck in 28%, Buttocks in
10%, Genital area in 8%.
The majority of the patients with successful Sclerotherapy in
first attempt were in Group B i.e. 38% as compared to 24% in Group
A whereas 26% in Group A versus only 10% in Group B patients
required Re-embolization. This observed difference was statistically
significant (X2=5.11, df=1, p<0.02).
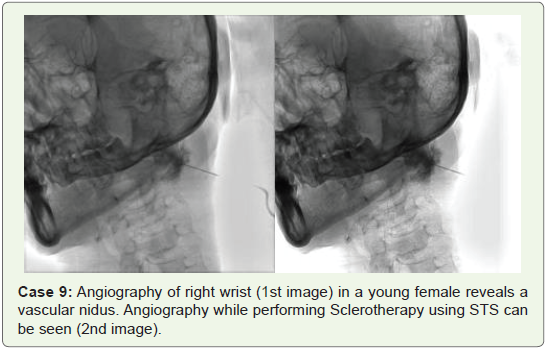
No major complications were found in our study, only the minor
complications in both groups were Pain in 26% and 14%; Swelling in
18% and 10%; Movement limitations in 28% and 22% in Group A and
Group B respectively, but the complications were comparable in both
the groups (X2=0.46, df=6, p>0.05) (Case 9).
These findings are similar to EskoVeräjänkorva15 who found
that Out of the 63 patients investigated, 83% (53) had Venous
Malformations (VMs) and 9% (5) were defined as having ArterioVenous Malformations (AVMs). Patients with a VM were operated
on, in 14% (8) out of all VM cases. Hence 86% (45) of patients
with a VM received adequate help to their symptoms solely from
sclerotherapy. The duration of treatment for the 14% of the VM
patients that needed a surgical procedure was prolonged by 7-9
months, that is, by 41%.
Conclusion
It can be concluded from our study that both the groups of
sclerosants were effective in the treatment for various malformations
but success in first attempt was more to combined sodium tetradecyl sulfate and lipiodol versus sodium tetradecyl sulfate alone and both the groups were having comparable complications.
References
Citation
Sharma N, Sharma MS. Role of Sclerotherapy in the Management of Various Types of Vascular Anomalies in a Tertiary Health Care Center. Indian J Appl Radiol. 2019;5(1): 141.