Research Article
Duodenum - a Forgotten Segment of Gastro Intestinal Tract on Abdominal CT Scan
Kavita U. Vaishnav, Janki B Jaradi1* and Pranay Patel
Department of Radiodiagnosis, L.G. Hospital, AMC MET Medical College, India
*Corresponding author: Janki B. Jaradi, Department of Radiodiagnosis, L.G. Hospital, AMC MET medical college, Maninagar, Ahmedabad, India; E-mail: janki_jaradi@yahoo.com
Copyright: © 2019 Kavita UV, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 25/07/2019; Accepted: 05/09/2019; Published: 07/09/2019
Abstract
Introduction: Duodenum is 25-30 cm long segment of small bowel. Computed Tomography (CT) of abdomen is routinely performed to evaluate
gastrointestinal pathologies, in patients presented with abdominal pain. In routine day to day practice CT scan is concentrated on the stomach, colon and ileo
caecal junction than duodenum. Radiology literature is also more focused on the colon, stomach and distal small bowel.
Materials and method: All the patients having abdominal pain and suspecting duodenal lesions were referred for abdomen pelvis CT scan to the
department of Radio diagnosis, LG hospital during the period of January 2012- June 2018 were evaluated to detect lesions of duodenum.
Result: Total 25 patients were included in study. The most common age group involved was 60-69 years followed by 20 to 40 years. Second part of
duodenum was commonly involved segment for pathologies followed by third part and fourth part. Common benign pathology was duodenal diverticulum in
five patients and malignant lesion was adenocarcinomas in seven patients. Other lesions of duodenum occur rarely.
Conclusion: CT scan is more helpful than other modalities for proper evaluation of duodenum and its pathologies.
Keywords
Duodenum; CT scan; Malignancy of duodenum
Introduction
This article presents the CT findings in various pathologies
involving the duodenum. The main aim of this article is to prove
importance of a commonly used modality- abdominal CT scan, in
the diagnosis of various duodenal disorders
In recent era abdominal CT has tremendous role in the detection,
and sometimes as an incidental finding, of various duodenal
pathologies. CT scan provides a three dimensional imaging capability
of Gastrointestinal Tract (GIT) pathology, as it allows visualization
of the lumen, wall abnormality and adjacent extramural structures
as well as distant metastasis. As well as lesions of the other organs,
lymphadenopathy and bony lesions were well evaluated by CT scan.
This article illustrates the various CT features of a different pathology
affecting the duodenum.
Aim: • To evaluate the duodenum and its pathology.
• To diagnose various lesions involving duodenum.
• To provide additional information involving other organs.
Materials and Methods
All the patients presented with abdominal pain, vomiting,
diarrhea and for some other conditions were referred for CT scan
abdomen and pelvis with or without contrast to the department of
1. Radio diagnosis, LG hospital during the period of March 2012 - June
2018 were evaluated to detect various pathologies of duodenum.
This study has been performed using 16 slice Phillips scan machine.
Written informed consent was obtained. Routine pre procedure was
done as per the protocol of the CT scan study.
2. Plain CT scans of abdomen and pelvis followed by
3. Arterial phases were obtained after negative test dose of
the non-ionic contrast by injecting 1-2 ml/kg of bodyweight of
intravenous contrast media through cubital vein by pressure injector
at a rate of 1.5 ml/sec. Scan was obtained 6 sec after starting of the
intravenous contrast
Venous phase- after 45-60 second.
Scan parameters were as follows: Volumetric data was obtained
from the vessels in axial plane and was reconstructed in sagittal,
coronal plane. Slice thickness- 1mm, Collimation- 0.6 mm, Pitch- 1.5,
MAS=200, Kvp120.
Conventional abdominal CT scans are done with the use of radio
opaque oral contrast material to distend the gastrointestinal tract.
When there is suspicion of a duodenal pathology, some techniques
can be used to optimize imaging of duodenum.
Results
Majority of the patients having complaints of abdominal pain,
vomiting, upper GI bleeding were referred to radiology department
for abdomen pelvis CT scan. Out of which 25 patients came across
with duodenal pathology.
Males (14) were more involved than female (11). The most
common age group involved was 60-69 years followed by 20 to 40
years. Second part of duodenum was common in involved in most
of the pathologies followed by third part and fourth part. First part
of the duodenum was least to involve and was commonly involved in
peptic ulcer disease and commonly presented with peptic perforation.
The most common benign pathology was duodenal diverticulum
in five patients and malignant lesion was adenocarcinomas in seven
patients. Out of which two patients had liver metastasis, six patients
had lymph nodal metastasis. Other pathologies were rare like;
groove pancreatitis, lymphoma, tuberculosis, bezoar and carcinoid
were respectively observed in one patient. Two patients had SMA
syndrome (Superior mesenteric artery syndrome) and trauma
respectively. A young Patient with SMA syndrome presented with
bowel obstruction, vomiting and pain (Table 1).
Discussion
To start with brief anatomy of duodenum will help for proper
evaluation and diagnosis of its lesions properly.
The duodenum is a 25-30 cm long C-loop segment of the
Gastrointestinal Tract (GIT) situated in the anterior pararenal space
of retro peritoneum, (except for the duodenal bulb). It extends from the pylorus of stomach (to the right of the midline) to the ligament of
Treitz (to the left of the midline). In this article we will try to discuss
CT scan findings of various pathologies involving duodenum one by
one.
Duodenal pathologies: Developmental pathologies: Duplications and diverticulum:
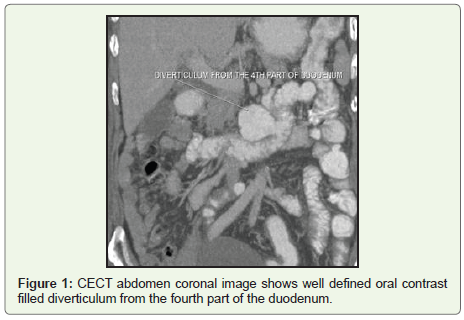
Duodenal diverticulum is a commonly occurring pathology of
duodenum. It may be either congenital or acquired, and is always
an incidental finding on CT scan and is found in 6% of upper GIT
barium studies. The common location of diverticulum is along the
mesenteric border of the second and third part of the duodenum.
The diverticulum is seen on CT as an air-filled and an air-fluid/orally
ingested contrast material level that may contain debris, medial to
the duodenal loop [1-3] (Figure 1). Sometimes the diverticulum may
complicate in to infection, perforation, hemorrhage, pancreatitis or
biliary obstruction and very rarely in malignancy (Table 2).
Duplication cysts are rare in the gastrointestinal tract,
approximately 2 to 12% occur in the gastro duodenal region [4,5].
Duodenal duplication arises most often in the medial wall of the
second and third portions of the duodenum and typically appears
as a well-circumscribed cystic mass with fluid attenuation. The
duplications typically do not communicate with the duodenal lumen
and may communicated with pancreatic and bile ducts [4,5]. Rarely,
carcinoma may arise inside a duplication cyst, and it appears as
vegetation or mural nodules inside the cyst.
Malrotation
Malrotation is defined as a congenital abnormal position of the
bowel within the peritoneal cavity and involves small and the large
bowel. Malrotation is accompanied by abnormal bowel fixation by
mesenteric bands or absence of fixation of portions of the bowel, leading
to increased risks of bowel obstruction, acute or chronic volvulus, and
bowel necrosis. Various degrees of malrotation of the small or large
bowel may occur, and the positions of the duodenojejunal junction
(and, by implication, the ligament of Treitz) and colon depend on
the developmental stage at which normal embryologic rotation failed.
Malrotation of the bowel is associated with a number of syndromes
and other anomalies. Malrotation occurs in approximately 1 in 500
births. Malrotation is usually diagnosed in newborns and young
infants; up to 75% of symptomatic cases occur in newborns, and up
to 90% of symptomatic cases occur within the 1st year of life [6-8].
Infective and inflammatory diseases: Infective diseases in the duodenum are becomes difficult
diagnosed from CT scans. Most infectious processes result in
inflammation of the duodenum and secondary duodenal wall edema.
The most common infectious cause of duodenitis is Helicobacter
pylori. Sometimes, crohn’s disease may involve the duodenum.
Less common infections include giardiasis and tropical sprue. The
imaging findings may be nonspecific, like wall thickening and luminal
dilatation, with or without adjacent nodes enlargement. Clinical
correlation is always helpful in diagnosis.
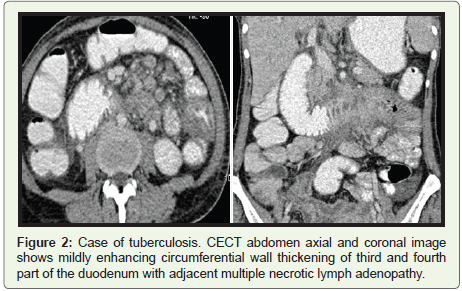
Tuberculosis: Tuberculosis of ileo caecal junction is most common involvement
in gastrointestinal tract. Tubercular involvement of the duodenum
accounts for only 2.3%. Duodenum along with stomach is rare
sites for tuberculosis and is usually a result of secondary spread
from a primary pulmonary disease [9]. The radiological features of
duodenum tuberculosis are usually nonspecific CT scan findings
shows circumferential wall thickening of the part of duodenum
with adjacent fat stranding and may be presented with symptoms of
obstruction and associated with adjacent necrotic mesenteric lymph
adenopathy and ascites [10,11] (Figure 2a and 2b).
Some extrinsic inflammatory diseases affecting the duodenum
like, in close relation to the pancreatic head and gall bladder. So,
infection of the adjacent structure affecting the duodenum, like acute
pancreatitis and cholecystitis may cause edema and mural thickening
of the duodenum.
Mass lesions: Duodenal tumors account for about one-third of small bowel neoplasms, which represent only 5-6% of all GIT neoplasia.
Benign tumors include adenoma, adenomatous polyp, lipoma and
leiomyoma. Amongst all leiomyma is the commonest benign mass
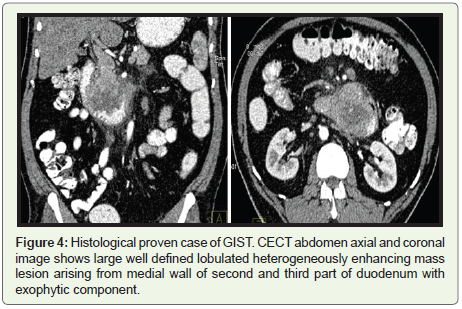
[12]. Gastro Intestinal Stromal Tumor (GIST) of the duodenum
present as an intramural, endoluminal, or exophytic mass, most
commonly in the second or third portion of the Patients with these
tumors often present with gastrointestinal bleeding and, occasionally,
abdominal pain.
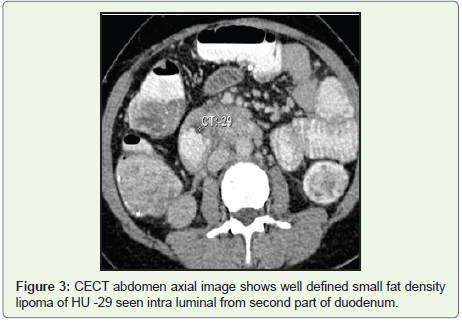
The diagnostic criteria used to predict a benign lesion is the
intraluminal location of a mass. Lipoma presents as characteristic
well defined intraluminal fat density lesion, on CT scan [12] (Figure 3, 4a and 4b).
There are three types of duodenal adenomas: tubular type,
villous adenoma, and Brunner gland adenoma. Villous adenomas
have a malignant potential and are treated with surgical resection
while tubular adenomas and Brunner gland adenomas are typically
surgically resectable.
The small bowel can be involved in various polyposis syndromes,
Peutz-Jeghers syndrome, and gardener syndrome. Presenting
symptoms are bleeding and obstruction from intussusceptions. At
CT, one may see intraluminal polyps, and the multiplicity of these
lesions should suggest a polyposis syndrome.
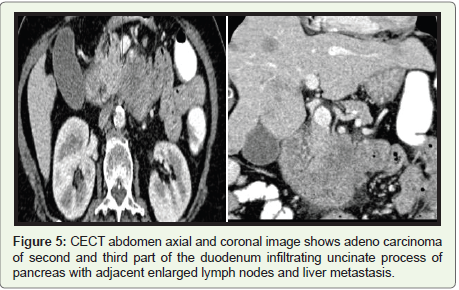
Primary malignant tumors include adenocarcinomas, which
comprise about 80-90% of all primary duodenal malignant neoplasm.
Primary adenocarcinomas of the duodenum is usually found in
the periampullary region [12-14]. Imaging features are as either a
polypoid mass or an irregular, circumferential constricting lesion
with wall thickening causing deformity of the lumen (Figure 5a and 5b). Additional CT findings are like infiltration of adjacent
retroperitoneal fat planes or surrounding organs, adjacent lymph
node enlargement, vascular encasement and distant metastases help
in predicting tumor prognosis [12].
Other rare tumors like, duodenal leiomyosarcoma may appear as
elsewhere in the GIT, typically has a large exophytic heterogeneously
enhancing mass lesion with central necrotic and hemorrhagic
component.
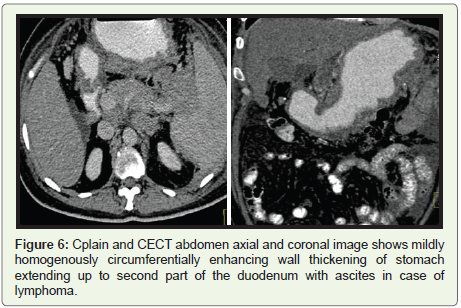
Lymphoma of the duodenum can occur with both primary
lymphoma and secondary involvement from systemic disease.
However, stomach lymphoma extending in to duodenum is common
presentation. CT scan findings are symmetrical circumferential
smooth or nodular large, homogenously enhancing wall thickening,
with normal mucosa. Aneurysmal dilatation of the affected segment
is key feature of lymphoma (Figure 6a and 6b).
Metastatic involvement of the duodenum from other primary
malignancies may occur due to local extension or metastases from
distant sites. Common primaries are from pancreas, colon, ovarian,
melanoma and breast.
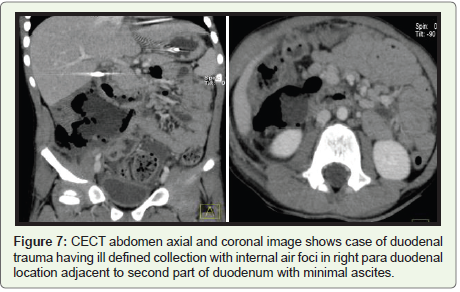
Duodenal trauma: Duodenal trauma may result from penetrating or blunt injury.
During blunt trauma, the duodenum may be crushed against the
vertebral body, causing contusion or transaction. CT scan plays
important role in duodenal trauma. Intramural hematoma without
perforation is usually managed conservatively, but traumatic
duodenal perforation is a surgical emergency. Free air with contrast in
right anterior pararenal space is specific sign of duodenal perforation
[15] (Figure 7a and 7b).
SMA Syndrome: Superior Mesenteric Artery (SMA) syndrome is an uncommon
condition characterized by compression of the third part of the duodenum between the aorta and the superior mesenteric artery.
It is commonly seen in thin and lean patients, and usually presents
with chronic, intermittent, or acute complete or partial duodenal
obstruction. Superior mesenteric artery syndrome was first described
in 1861 by Von Rokitansky, who proposed that its cause was
obstruction of the third part of the duodenum as a result of arterio
mesenteric compression. The incidence of superior mesenteric
artery syndrome is from 0.1-0.3% according to study in literature
[16]. Despite its rarity about 400 cases were described in the English
language literature [17]. In SMA syndrome the fatty tissue between
aorta and mesenteric artery in lost and causes compression of
duodenum between it. The aortomesenteric angle is reduced below
60 0 to 150 between SMA and aorta is reduced.
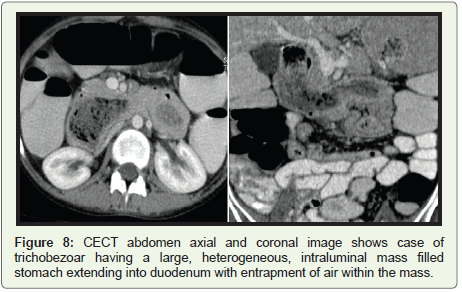
Bezoar: A bezoar is composed of accumulation of foreign material in
the GIT; most commonly in stomach may extend into duodenum.
Amongst all bezoars, trichobezoars and phytobezoars are the two
most common. Trichobezoar, a concentrated ingested hair material,
occurs commonly in young women. It usually fills the stomach and
the first part of the duodenum. The imaging features of a trichobezoar
are characteristic of a large, heterogeneous, intraluminal mass with
entrapment of air within the mass is considered a helpful diagnostic
sign. Phytobezoar is composed of indigested food particles and is
commonly seen in patients having poor digestion and decreased
gastric motility [18] (Figure 8a and 8b).
Postsurgical changes of the duodenum: CT is the mainstay of imaging of the postoperative abdomen.
Most postoperative complications, including abscess, wound
dehiscence, hematoma, hernia, anastomotic leakage, and bowel
obstruction, are well depicted with CT. Afferent loop syndrome,
caused by obstruction of the duodenum and jejunum proximal to the
gastrojejunostomy anastomosis, is an uncommon complication of
subtotal gastrectomy with the Bilroth II procedure.
Conclusion
The duodenum is frequently overlooked during interpretation of
abdominal CT examinations. To avoid it optimal knowledge about
the duodenum and its pathologies is important to increase accuracy
in diagnosis of it on abdominal CT.
References
Citation
Kavita UV, Jaradi JB, Patel P. Duodenum - a Forgotten Segment of Gastro Intestinal Tract on Abdominal CT Scan. Indian J Appl Radiol.
03 2019;5(1): 138.