Research Article
A Study of Outcome of Patients with Ruptured Intracranial Aneurysm Treated by Endovascular Embolization
Sharma N* and Sharma MS
Department of Radiodiagonisis, SRMS-IMS, India
*Corresponding author: Sharma N, Department of Radiodiagonisis, SRMS-IMS, Bhojipura, Bareilly, India
Copyright: © 2019 Sharma N, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 10/07/2019; Accepted: 26/08/2019; Published: 28/08/2019
Abstract
Introduction: In India, in the past 15 years, the growth of neurosurgery has been very rapid and a large number of neurological interventions are being
attempted. The procedure of cerebral angiography has been widely accepted , But, the diagnosis of intra-cranial aneurysms is much less frequently made in
India as compared to the western countries despite out current population of 132.42 crore.
Aims and objectives: To study outcome of patients with intracranial aneurysm treated by endovascular embolization.
Methodology: This was Prospective study carried out at database of all neuro-interventional cases performed by the interventional neurology team at
AVBRH, Sawangi, Wardha in 6 Months period i.e. April 2018 to September 18 were included for the study. In the six month period there were 25 patients
undergone for intracranial embolization for various types of intracranial aneurysm. All ages, both sexes were selected by non-probability sampling method.
All patients with ruptured intracranial aneurysms were treated by endovascular treatment. The statistical analysis was done by SPSS 19 version software.
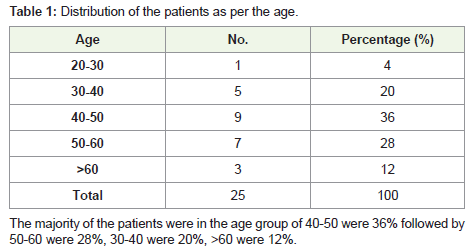
Result: The majority of the patients were in the age group of 40-50 were 36% followed by 50-60 were 28%, 30-40 were 20%, >60 were 12%. The majority
of the patients were Male i.e. 68% followed by Female 32%. The most common symptoms were Headache in 76% followed by, Vertigo in 68%, Seizure In
44%, Tinnitus in 36%, Blurred image in 32%, Difficulty in speaking in 20%, Photophobia In 12%. The majority of the patients were having the GCS in 9-12 were
48%, followed by 12-15 were 28%, 6-9 were 16%, 3-6 were 8%. The average Fisher grade was 13± 3.21, Modified Rankin Scale was 14.32± 2.91, Hunt and
Hess Classification was 12.89 ± 3.92. In our study we have seen that 56% has Cure, 32% no cure and 12% patients lost, the cure was highest to Ist session
i.e. 28%, followed by IInd 12%, at 0; 8%. The majority patients get cure in Ist session as compared others, this observed difference was statistically significant
(χ2 = 6.17,df=1, p<0.013).
Conclusion: It can be concluded from our study that The majority of the patients were in the age group of 40-50 were, The most common symptoms were
Headache followed by, Vertigo Seizure, Tinnitus etc. The overall cure rate was 56% and the majority patients get cure in Ist session as compared others, so it
seems that this procedure is safe and should be performed whenever the intervention is indicated in the patients.
Keywords
Intracranial aneurysm; Endovascular Embolization; Outcome of endovascular embolization
Introduction
In India, in the past 15 years, the growth of neurosurgery has been
very rapid and a large number of neurological interventions are being
attempted. The procedure of cerebral angiography has been widely
accepted [1]. But, the diagnosis of intra-cranial aneurysms is much less frequently made in India as compared to the western countries despite out current population of 132.42 crore [2].
Various causes of subarachnoid haemorrhage are trauma (with
associated cerebral contusion): traumatic subarachnoid haemorrhage
and spontaneous subarachnoid haemorrhage caused by ruptured berry aneurysm, perimesencephalic haemorrhage, arterio-Venous
Malformation (AVM), dural Arterio-Venous Fistula (DAVF), spinal
arterio-venous malformation, venous infarction, intradural arterial
dissection [3].
Aneurysmal Subarachnoid Hemorrhage (aSAH) commonly
occurs due to rupture of saccular aneurysms and is the cause for
an estimated 5-15% of all strokes [4]. A ruptured aneurysm quickly
becomes life-threatening and requires prompt medical treatment. The
key symptom of a ruptured aneurysm is a sudden, severe headache
described as the worst headache ever experienced [5]. Considering
the annual incidence of aneurysmal SAH between 6 and 16/100,000
population [6], about 76,500-204,100 new cases occur in India each
year. Awareness and healthcare accessibility determines the diagnosis
and management of these patients.
Cerebral angiography is the gold standard for diagnosis of
cerebral aneurysm. However the diagnosis of unruptured AVM’s and
Aneurysm’s is still difficult due to absence of symptoms that make
the patient come to the hospital for check up and investigations. Our
study is with aim of study of possible outcome and clinical features
of patients with intracranial aneurysm treated by endovascular
embolization.
Methodology
This was Prospective study carried out at database of all neurointerventional cases performed by the interventional neurology team
at AVBRH, Sawangi, Wardha in 6 Months period i.e. April 2018 to
September 18 were included for the study. In the six month period
there were 25 patients undergone for intracranial embolization for
various types of intracranial aneurysm. All ages, both sexes were
selected by non-probability sampling method. All patients with
ruptured intracranial aneurysms were included in the study and
treated by endovascular treatment (Coiling). Patients protected
by law, Patients already treated by endovascular approach for an
intracranial aneurysm, Patients having a dissecting aneurysm, Poor
surgical candidates were not included into the study. This data was
prospectively collected during the study period and includes the
Demographic information like: age, sex. The clinical characteristics
of all the patients with aneurysmal subarachnoid haemorrhage was
graded using the Hunt and Hess grading scale, Fisher grade, and
Glasgow Coma Scale (GCS). Clinically, patients with intra-cranial
Aneurysm present with intracranial hemorrhage, headaches, seizures
and long-term disability etc. was noted. The various scale’s used
for grading was as depicted below. Prior to taking the patient for
endovascular embolization, the patients were graded using these
scales.
The features of the procedure like date of the procedure,
aneurysm size, location and morphology, total radiation exposure,
and endovascular devices were also collected. The coiling was
performed on Philips Alura X per FD 20 machine. Post operative
complications, both intra-procedural and peri-procedural (48h) were
studied if present and classified into major and minor types. The
various complications were categorized as - procedural complications
- thromboembolic events, rupture/perforation and device related problems b) disability at 1 month, studied by the modified Rankin
scale (score >2). The modified rankin scale was used to grade the
outcome of the treated patients with intracranial Aneurysm, assed in
subsequent follow up.
All the patients that underwent endovascular coiling of ruptured
intracranial aneurysms were enrolled in the above-mentioned
database and incorporated into the prospective analysis. The statistical
analysis was done by SPSS 19 version software.
Result
In our study we have seen that 56% has Cure, 32% no cure and
12% patients lost, the cure was highest to Ist session i.e. 28%, followed
by IInd 12%, at 0 ;8%. The majority patients got cured in the Ist session
as compared to others, this observed difference was statistically
significant (χ2 = 6.17, df=1, p<0.013).
Discussion
In general, there are two broad categories of intracranial
aneurysms: (1) those that have already ruptured, causing subarachnoid
hemorrhage, and (2) those that are unruptured. Typically, unruptured
aneurysms are asymptomatic; however, rarely they may become
symptomatic usually due to their size and subsequent mass effect. The
management of these two types of lesions differs dramatically [7].
Ruptured aneurysms: These lesions are almost always treated provided that the patient
is neurologically and physiologically well enough to undergo therapy,
either surgical clipping or endovascular coiling. Subarachnoid
hemorrhage from aneurysm rupture is a devastating event with
a case-fatality rate of 51% and a 50% rate of significant disability
among survivors [8-10]. Treatment is typically carried out urgently
rather than emergently, usually within 24 hours after the arrival of the
patient to the hospital. Initially, there was considerable controversy
with respect to the treatment modality that was best suited for the
right of first refusal for therapy, however, much of this controversy
was settled by the International Subarachnoid Aneurysm Trial
(ISAT), which demonstrated that for aneurysms amenable to either
therapy, patients undergoing coil embolization had better long-term
outcomes than those who underwent open surgical.
Clipping although there were some concerns regarding the
durability of coil embolization as a treatment modality [11-13],
an analysis of the ISAT data demonstrated that the superiority of
endovascular coiling was preserved for at least 7 years after treatment
[14]. For this reason, at most institutions, endovascular coiling is
granted the right of first refusal for ruptured aneurysms amenable to
either treatment modality.
Unruptured aneurysms: The vast majority of aneurysms discovered incidentally are
completely asymptomatic. During the past decade, with the
proliferation of noninvasive cerebro-vascular imaging studies ordered
by referring physicians, we have begun to diagnose small, unruptured
aneurysms with increasing frequency. The diagnosis typically is the cause of great anxiety on the part of the patient and referring physician,
resulting in immediate referral to a cerebrovascular interventionist
for evaluation. At this point, the decision of whether to treat must
be based on the best available evidence regarding the risk of rupture
of an incidentally diagnosed cerebral aneurysm. Unfortunately, the
available evidence and its interpretation are still actively debated, and
these decisions are rarely straightforward. Ultimately, three options
are typically provided-conservative management (with or without
imaging surveillance), open surgical clipping, and endovascular
coil embolization-with the patient making a final decision based
on a fair and unbiased presentation of the available data regarding
all treatment modalities. The largest study of the natural history of
incidentally discovered unruptured intracranial aneurysms (The
International Study of Unruptured Intracranial Aneurysms [ISUIA])
is highly controversial and indicated much lower rates of annual
rupture than the majority of previous studies on this topic [14-21].
We have considered all points regarding the treatments we have
found that , The majority of the patients were in the age group of
40-50 were 36% followed by 50-60 were 28%, 30-40 were 20%, >60
were 12%.
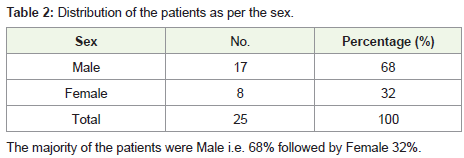
The majority of the patients were Male i.e. 68% followed by
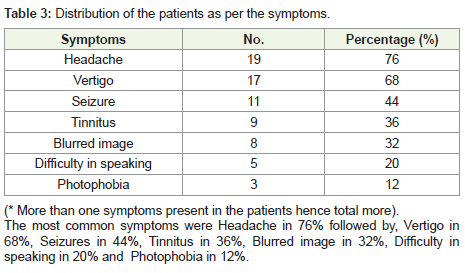
Female 32%. The most common symptoms were Headache in 76%
followed by, Vertigo in 68%, Seizures In 44%, Tinnitus in 36%,
Blurred image in 32%, Difficulty in speaking in 20%, Photophobia
in 12%. The majority of the patients were having the GCS in 9-12
were 48%, followed by 12-15 were 28%, 6-9 were 16%, 3-6 were 8%.
The average Fisher grade was 13±3.21, Modified Rankin Scale was
14.32±2.91, Hunt and Hess Classification was 12.89±3.92.
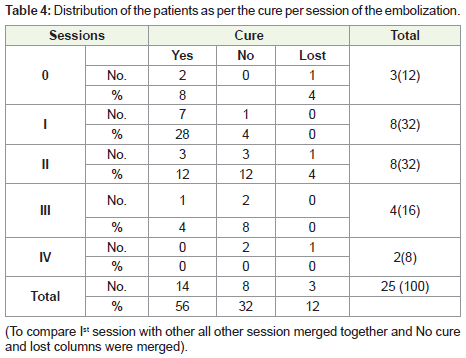
In our study we have seen that 56% has Cure, 32% no cure
and 12% patients lost, the cure was highest to Ist session i.e. 28%,
followed by IInd 12%, at 0; 8%. The majority of patients got cured in
the Ist session as compared to others, this observed difference was
statistically significant (χ2 = 6.17, df=1, p<0.013). These findings are
similar to Juan Carlos Puentes 35 et al. they found A higher cure rate
was achieved with a single embolization session, where a 20% cure
rate was attained with a single session in smaller lesions, compared
to a 6% cure rate when up to three sessions were required for more
complex lesions [21].
Conclusion
Endovascular intervention is an innovative, less invasive
procedure used to treat problems affecting the blood vessels, such
as an aneurysm, which is a swelling or “ballooning” of the blood
vessel. The procedure involves puncturing the femoral artery with
an 18G needle. Super-selective cannulation of the artery from
which the aneurysm is arising is done using micro-catheters and
micro-guidewires. Coiling is done for embolization. In the past, this
condition was treated by open surgery, involving an incision in the
side of the chest or breastbone and a long recovery period. Patients
generally stay in the hospital for seven to 10 days following open
surgery and undergo a three-month recovery. An alternative to open
surgery, endovascular surgery offers many advantages, including a
shorter recovery period, less discomfort, local or regional anesthesia
instead of general anesthesia, smaller incisions, less stress on the heart
and fewer risks for patients with other medical conditions. Also, the overall cure rate in our study was 88.89% and the majority of patients
got cured in the Ist session, so it seems that Embolization is safe and
should be performed whenever the intervention is indicated in the
patients.
References
Citation
Sharma N, Sharma MS. A Study of Outcome of Patients with Ruptured Intracranial Aneurysm Treated by Endovascular Embolization. Indian
02 J Appl Radiol. 2019;5(1): 137.