Research Article
Dual Energy Computed Tomography to Determine Composition of Renal Stones
Chidananda Murthy Mangala and Praveen John*
Department Of Radio-Diagnosis, A.J. Institute of Medical Sciences and Research Centre, India
Corresponding author: Praveen John, Associate Professor, Department of Radio-Diagnosis, A.J. Institute of Medical Sciences and Research Centre, NH 17, Kuntikana, Mangalore -575004, India
Citation: Murthy MC, John P. Dual Energy Computed Tomography to Determine Composition of Renal Stones. Indian J Appl Radiol. 2019;5(1): 133.
Copyright ©2019 Chidananda Murthy Mangala, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 5, Issue: 1
Submission: 07/03/2019; Accepted: 05/04/2019; Published: 09/04/2019
Abstract
Aim: To evaluate the utility of dual energy computed tomography (DECT) to characterize the chemical composition of renal stones.
Material and methods: A single tertiary care center cross-sectional study with consecutive enrolment of eligible subjects. Subjects were initially scanned using a standard low dose renal stone CT, and DECT was performed after confirmation of the renal stone and only on the area of the stone. Images acquired with the DECT were processed using a dedicated workstation and dedicated software.
Results: The study included 49 subjects with a mean age ± SD of 45.35 ± 14.77 years; 39 (79.59%) of subjects were males. The mean size of renal stones was 16.16mm ± 10.88 (median 12) and ranged from 5 to 60mm. Attenuation ratios for uric acid stones were the smallest, ranging from 0.98 to 1.02 (mean 1.00 ± 0.02) and differed significantly (student t-test p < 0.001) from calcium stones that had the largest attenuation ratios ranging from 1.33 to 1.86 (mean 1.50 ± 0.09). There was only 1 cysteine stone and it had an attenuation ratio of 1.18. DECT had 100% (95% CI: 54.1, 100) sensitivity and 100% specificity (95% CI: 91.8, 100) and a kappa value of 1.0 indicating perfect agreement in this study to differentiate uric acid from non uric acid stones.
Conclusion: Dual energy CT can be used to characterize chemical composition of renal stones providing useful information in their clinical management and to differentiate uric acid from non uric acid stones.
Keywords: Renal stones; Urinary calculi; Dual energy computed tomography; Computed tomography
Introduction
Renal stones are a common clinical condition affecting 10-14% of the population [1-3]. Patients symptomatic with renal stones may complain of intermittent flank pain, urinary urgency, hematuria, nausea and vomiting [1]. Untreated urinary stones may cause urinary tract obstruction and consequently, infection, renal insufficiency and end stage renal disease [1]. Renal stones are commonly calcium oxalate (70%), calcium phosphate (20%), and uric acid (8%) and cysteine (2%) stones [4].
Dual Energy Computed Tomography (DECT) relies on the chemical characterization of renal stones in addition to assessment of size, location and stone surface. The measurement involves perfect breath hold as the values obtained with even slight motion are significantly different from those obtained with no motion [5,6]. DECT has been reported to have nearly 100% sensitivity and specificity for characterizing the chemical composition of stones >3 mm [7]. Recent studies have shown that DECT can distinguish calcium oxalate, calcium phosphate and cysteine stones in addition to uric stones [8,9]. The aim of the current study was to evaluate the utility of DECT to characterize the chemical composition of renal stones among patients presenting to a single tertiary care center in south India.
Material and Methods
A cross sectional study design was used to determine the effectiveness of DECT in chemical characterization of renal stones. The study was carried out at a tertiary care center in south India. The study protocol was approved by the institutional ethics committee and informed consent was obtained from all study participants prior to enrolment. A convenience sample size of 49 subjects was chosen for the study and were recruited consecutively. Subjects with renal stones ≥ 5 mm were included in the study. The study did not exclude subjects based on sex or age. Subjects with any potential contraindications to radiation like pregnancy were excluded from the study. A detailed personal history including risk behaviours, clinical signs and symptoms of the current illness, any past clinical history including co-morbidities was obtained from each subject. Each subject had a detailed abdominal and pelvic examination including an initial ultrasound exam for assessment of renal stones and to look for any renal changes.
All subjects were initially assessed using a multidetector DECT scanner (Siemens SOMATOM Definition 128 slice dual source with dual energy CT scanner) with the subject lying in the supine position, with head fixed and arms above the head. The subject was encouraged to hold breath on instruction. Subjects were scanned from the xiphi-sternum to the symphysis pubis with a scan delay of 0.5 seconds. Three sets of images were acquired (Set A at 140 kV, Set B at 80 kV and Set M mixed) at slice thickness of 3mm. Images were reconstructed to produce 0.6 to 1.5 mm slice thick sections. The Care Dose 4D Auto mA protocol was used to adjust the mA to reduce the radiation dose to the patient. Patients were initially scanned using a standard low dose renal stone CT, and DECT was performed after confirmation of the renal stone and only on the area of the stone. Images acquired with the DECT were processed suing a dedicated Siemens workstation and dedicated Somaris / 7 Syngo CT2012B software. All exams were visualized on the axial, coronal and sagittal planes.
Data were entered initially into a MS excel spreadsheet and then exported into STATA (v10.0, College Station, Tx, USA) for statistical analysis. The mean and standard deviation were determined for continuous variables and frequency distributions and proportions for categorical variables. Statistical inferential testing of continuous variables was done using the students t-test. A p value < 0.05 was considered as statistically significant. The diagnostic effectiveness of DECT to differentiate uric acid and non uric acid stones was determined using sensitivity and specificity (point estimates and 95% confidence intervals around the point estimates). The attenuation ratio and the correlation of DECT and Fourier Transform Infrared Spectroscopy (FTIR) was assessed. FTIR analysis or spectroscopy is an analytic technique used to identify organic, polymeric and in some cases inorganic materials. The FTIR analysis method uses infrared light to scan test samples and observe chemical properties. The agreement pertaining to the chemical characterization was assessed using the Kappa statistic.
Results
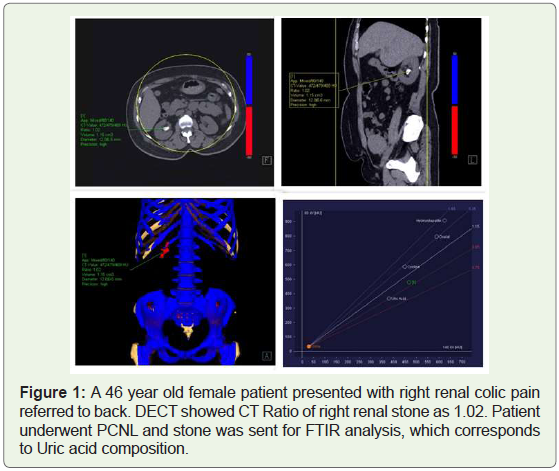
The study included 49 subjects with a mean age ± SD of 45.35 ± 14.77 years; 39 (79.59%) of subjects were males. Twenty Nine (59.18%) subjects had a Ureteroscopic Lithotripsy (URSL), 17 (34.69%) subjects had a PCNL Percutaneous Nephrolithotomy (PCNL) and 3 subjects had a CLT Cystolithotripsy (CLT) ( Figure 1).
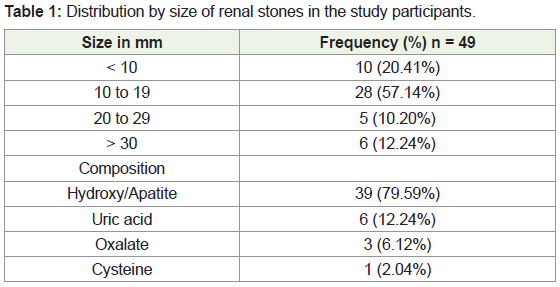
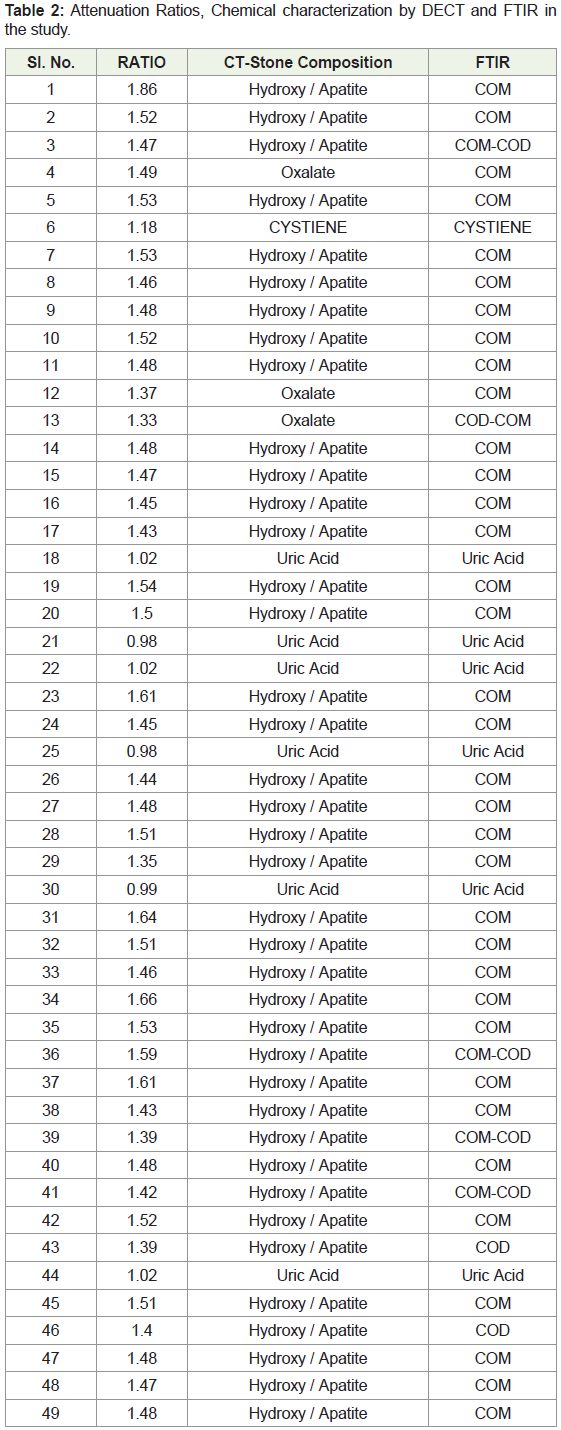
The mean size of renal stones was 16.16 ± 10.88 (median 12) and ranged from 5 to 60 mm. Table 1 shows the distribution of stones by size and the composition of stones as determined by computerized tomography. Table 2 shows the attenuation ratio and the correlation between DECT characterization and Fourier Transform Infrared Spectroscopy (FTIR). FTIR Analysis or spectroscopy is an analytic technique used to identify organic, polymeric, and in some cases inorganic materials. The FTIR analysis method uses infrared light to scan test samples and observe chemical properties. Attenuation ratios for uric acid stones were the smallest, ranging from 0.98 to 1.02 (mean 1.00 ± 0.02) and differed significantly (student t-test p < 0.001) from calcium stones that had the largest attenuation ratios ranging from 1.33 to 1.86 (mean 1.50 ± 0.09). There was only 1 cysteine stone and it had an attenuation ratio (1.18) that was larger than uric stones but smaller than the calcium stones (Figure 2). DECT showed a high correlation with the characterization on FITR and had a 100% (95% CI: 54.1, 100) sensitivity and 100% specificity (95% CI: 91.8, 100) specificity and a kappa value of 1.0 indicating perfect agreement in this study to differentiate uric acid from non uric acid stones Table 2.
Discussion
DECT had a very good diagnostic effectiveness for the chemical characterization of renal stones in this study. Attenuation ratios showed a significant difference between uric acid stones and calcium stones indicating their clinical usefulness. These results are consistent with previous studies reported in the global literature [8,13-16].
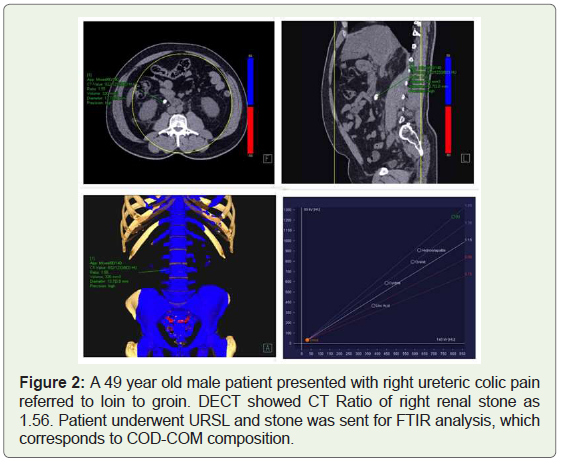
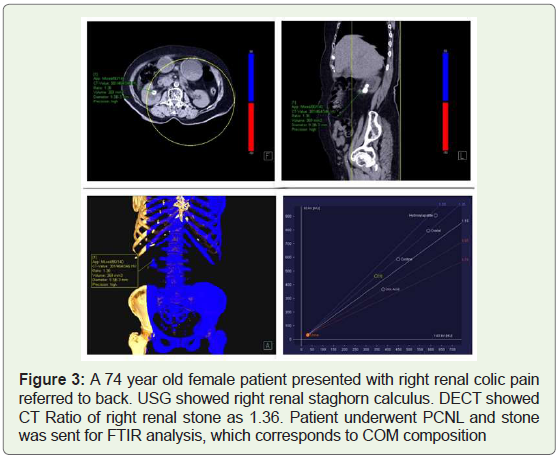
The concept of DECT was described nearly 30 years back and has gained recent importance due to improvements in scanning technology and post processing software [10]. The attenuation ratio helps to differentiate two materials and is defined as the ratio of the CT number of a given material in low energy to the CT number of the same material in a high energy image [11]. CT attenuation does not show a change with beam energy for soft tissues, however, it shows a significant variation for material with large atomic numbers, which allows for its use in the characterization of renal stones [12]. Several studies have reported on the ability of DECT to distinguish between uric acid and non uric acid stones [8,13-15] while another study reported that only the major component can be determined in cases of mixed stones [16] (Figure 3).
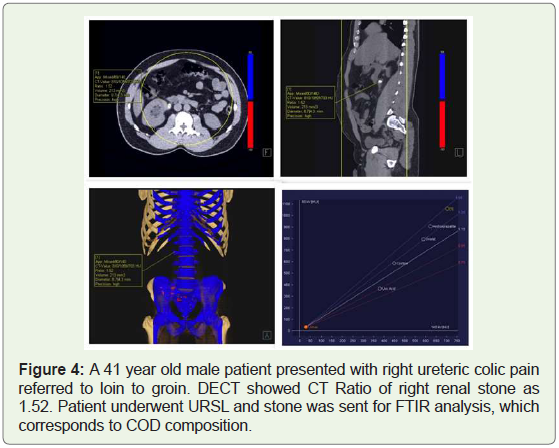
DECT has several limitations including the ability to characterize accurately in stones < 3 mm and stones with mixed composition [16]. Clinically, however, stones < 4 mm tend to pass spontaneously in nearly 80% of cases and hence this limitation may not be very significant [14]. From a clinical perspective, the ability to distinguish between uric acid and non uric acid stones is helpful as uric acid stones may pass out naturally and can be managed without surgical intervention. Larger stones, especially non uric acid stones, may require surgical intervention to alleviate symptoms (Figure 4).
Radiation exposure is a concern that can be limited through the use of radiation protection strategies and focused scanning. It is recommended to start with a low dose abdominal scan to identify and locate the stone before attempting DECT. Respiratory movements is another limitation that requires the full co-operation of the subject during the procedure. Several studies have shown that low dose DECT protocols can distinguish calcified and non-calcified stones [15,17-20].
The small sample size and recruitment of subjects from a single center may be considered limitations, however, even with these limitations; we were able to demonstrate an excellent diagnostic effectiveness for DECT that is consistent with existing knowledge.
Conclusion
Dual energy CT can be used to characterize chemical composition of renal stones providing useful information in their clinical management and to differentiate uric acid from non uric acid stones.
References
- Curhan GC (2007) Epidemiology of stone disease. Urol Clin North Am 34: 287-293.
- Trinchieri A, Coppi F, Montanari E, Del Nero A, Zanetti G, et al. (2000) Increase in the prevalence of symptomatic upper urinary tract stones during the last ten years. Eur Urol 37: 23-25.
- Trinchieri A (2008) Epidemiology of urolithiasis: an update. Clin Cases Miner Bone Metab 5: 101-106.
- Saita A, Bonaccorsi A, Motta M (2007) Stone Composition: where do we stand? Urol Int 79: 16-19.
- Boll DT, Patil NA, Paulson EK, Merkle EM, Simmons WN, et al. (2009) Renal stone assessment with dual-energy multidetector CT and advanced postprocessing techniques: improved characterization of renal stone composition--pilot study. Radiology 250: 813-820.
- Grosjean R, Sauer B, Guerra RM, Daudon M, Blum A, et al. (2008) Characterization of human renal stones with MDCT: advantage of dual energy and limitations due to respiratory motion. AJR Am J Roentgenol 190: 720-728.
- Manglaviti G, Tresoldi S, Guerrer CS, Di Leo G, Montanari E, et al. (2011) In vivo evaluation of the chemical composition of urinary stones using dual energy CT. AJR Am J Roentgenol 197: W76-W83.
- Primak AN, Fletcher JG, Vrtiska TJ, Dzyubak OP, Lieske JC, et al. (2007) Non invasive differentiation of uric acid versus non- uric acid kidney stones using dual energy CT. Acad Radiol 14: 1441-1447.
- Thomas C, Krauss B, Ketelsen D, Tsiflikas I, Reimann A, et al. (2010) Differentiation of urinary calculi with dual energy CT: effect of spectral shaping by high energy tin filter. Invest Radiol 45: 393-398.
- Alvarez RE, Macovski A (1976) Energy-Selective reconstructions in X-ray computed tomography. Phys Med Biol 21: 733-744.
- Primak AN, Giraldo JC, Eusemann C, Schmidt B, Kanotr B, et al. (2010) Dual source dual energy CT with additional tin filtration: dose and image quality evaluation in phantoms and in-vivo. AJR 195: 1164-1174.
- Johnson TR, Krauss B, Sedlmair M, Grasruck M, Bruder H, et al. (2007) Material differentiation by dual energy CT: Initial experience. Eur Radiol 17: 1510-1517.
- Stolzmann P, Kozomara M, Chuck N, Muntener M, Leschka S, et al. (2010) In vivo identification of uric acid stones with dual energy CT: Diagnostic performance evaluation in patients. Abdom Imaging 35: 629-635.
- Graser A, Johnson TR, Bader M, Staehler M, Haseke N, et al. (2008) Dual energy CT characterization of urinary calculi: initial in vitro and clinical experience. Invest Radiol 43: 112-119.
- Ascenti G, Siragusa C, Racchiusa S, Ielo I, Privitera G, et al. (2010) Stone targeted dual energy CT: a new diagnostic approach to urinary calculosis. AJR Am J Roentgenol 195: 953-958.
- Kulkarni NM, Pinho DF, Kambadakone AR, Sahani DV (2013) Emerging technologies in CT-Radiation dose reduction and dual energy CT. Semin Roentgenol 48: 192-202.
- Henzler T, Fink C, Schoenberg SO, Schoepf UJ (2012) Dual energy CT: radiation dose aspects. AJR Am J Roentgenol 199: S16-S25.
- Eiber M, Holzapfel K, Frimberger M, Straub M, Schneider H, et al. (2012) Targeted dual-energy single-source CT for characterisation of urinary calculi: experimental and clinical experience. EurRadiol 22: 251-258.
- Wilhelm K, Schoenthaler M, Hein S, Adams F, Schlager D, et al. (2015) Focused dual-energy CT maintains diagnostic and compositional accuracy for urolithiasis using ultralow dose non contrast CT. Urology 86: 1097-1102.
- Cai X, Zhou Q, Yu J, Xian Z, Feng Y, et al. (2014) Impact of reduced radiation dual energy protocols using 320-detector row computed tomography for analysing urinary calculus components: initial in vivo evaluation. Urology 84: 760-765.